You might also like
- Newman's Certified Electronic Health Records Technician Study GuideFrom EverandNewman's Certified Electronic Health Records Technician Study GuideNo ratings yet
- Order ### 2672790Document11 pagesOrder ### 2672790Wallace Mandela Ong'ayoNo ratings yet
- Nur 410-Informatics Project 2022Document21 pagesNur 410-Informatics Project 2022api-598192448No ratings yet
- New Electronic Health Records in NursingDocument11 pagesNew Electronic Health Records in Nursingapi-420570400No ratings yet
- Term Paper Complete DraftDocument16 pagesTerm Paper Complete Draftapi-464597952No ratings yet
- EHR WordDocument27 pagesEHR WordALAYSHA ALI100% (1)
- Hcin 540 EssayDocument14 pagesHcin 540 Essayapi-408487557No ratings yet
- Electronic Medical Record/Electronic Health Record System: Problem Based LearningDocument13 pagesElectronic Medical Record/Electronic Health Record System: Problem Based LearningTonmoy Banerjee100% (1)
- Leskovac Week 5 FinalDocument12 pagesLeskovac Week 5 Finalapi-527774673No ratings yet
- Nursing Informatics PaperDocument12 pagesNursing Informatics Paperapi-376040443No ratings yet
- Newsletter and RP STARTDocument4 pagesNewsletter and RP STARTBálint ÁrpádNo ratings yet
- Ehr Recommendation ReportDocument8 pagesEhr Recommendation Reportapi-356200224No ratings yet
- EMR Vs EMRDocument6 pagesEMR Vs EMRisurukalharaNo ratings yet
- Materi Tugas Seminar Bhs Inggris Semeter 4Document3 pagesMateri Tugas Seminar Bhs Inggris Semeter 4Yeni septiana putriNo ratings yet
- Electronic Medical RecordDocument4 pagesElectronic Medical Recordemmy_lineNo ratings yet
- NCM 104 Community Health Nursing 1: Bachelor of Science in NursingDocument8 pagesNCM 104 Community Health Nursing 1: Bachelor of Science in NursingMargarette GeresNo ratings yet
- Running Head: Telehealth Nursing Utilized For 1Document11 pagesRunning Head: Telehealth Nursing Utilized For 1api-385363448No ratings yet
- RiskDocument15 pagesRiskSitota KebedeNo ratings yet
- Nursing InformaticsDocument8 pagesNursing InformaticsWac GunarathnaNo ratings yet
- Chapter Two Literature Review: 2.1 Background Theory of StudyDocument3 pagesChapter Two Literature Review: 2.1 Background Theory of StudyAyinde AbiodunNo ratings yet
- ch2 Electronic Health RecordDocument8 pagesch2 Electronic Health Recordkelilidris70No ratings yet
- Hcin 540 - Term PaperDocument16 pagesHcin 540 - Term Paperapi-428767663No ratings yet
- Proposal For The Implementation of An Electronic HealthDocument14 pagesProposal For The Implementation of An Electronic HealthGraceNo ratings yet
- Adverse Event or Near-Miss Analysis (Nursing) .EditedDocument10 pagesAdverse Event or Near-Miss Analysis (Nursing) .EditedMaina PeterNo ratings yet
- (Student'S Name) (Institution Name) (DATE) : Healthcare Management Action PlanDocument7 pages(Student'S Name) (Institution Name) (DATE) : Healthcare Management Action Planwriter topNo ratings yet
- Electronic Medical RecordDocument10 pagesElectronic Medical RecordPrem Deep100% (1)
- Nursing Technologies - EditedDocument6 pagesNursing Technologies - EditedmelkyNo ratings yet
- Using Informatics To Improve Patient Care and SafetyDocument10 pagesUsing Informatics To Improve Patient Care and Safetyapi-404187614No ratings yet
- CernerDocument10 pagesCernerazul2233No ratings yet
- Knowledge ManagementDocument13 pagesKnowledge ManagementSharonz MuthuveeranNo ratings yet
- Nurses Perceptions of The Impact of The Electronic Health RecordDocument37 pagesNurses Perceptions of The Impact of The Electronic Health RecordElvira GumiNo ratings yet
- Document 20Document3 pagesDocument 20api-586815209No ratings yet
- Electronic Health Record: Types and ComponentsDocument8 pagesElectronic Health Record: Types and ComponentsLassie AbusadoNo ratings yet
- CH 11 - Ehr ActivityDocument4 pagesCH 11 - Ehr ActivityJAY LORENZ CARIDONo ratings yet
- Eng120-Week 14 - Final Essay - FinalDocument9 pagesEng120-Week 14 - Final Essay - Finalapi-626793332No ratings yet
- Running Head: Electronic Health RecordsDocument7 pagesRunning Head: Electronic Health RecordsJefferson KagiriNo ratings yet
- InformaticsprojectfinalDocument10 pagesInformaticsprojectfinalapi-449021066No ratings yet
- Bedside Shift Report and Utilizing The EhrDocument9 pagesBedside Shift Report and Utilizing The Ehrapi-349480325No ratings yet
- Patient Management System (New Reviewed)Document39 pagesPatient Management System (New Reviewed)Ajewole Eben Tope100% (1)
- Ehr Poster 1 1Document1 pageEhr Poster 1 1api-542441070No ratings yet
- EHR DocumentationDocument7 pagesEHR DocumentationNursingNowNo ratings yet
- Nursing Informatics FinalsDocument7 pagesNursing Informatics FinalsAlyNo ratings yet
- Sample Capstone Paper: Health Information ManagementDocument4 pagesSample Capstone Paper: Health Information ManagementRoromdrNo ratings yet
- gjmbsv3n3spl 14Document25 pagesgjmbsv3n3spl 14areeb khanNo ratings yet
- Advantages of Electronic Health RecordsDocument4 pagesAdvantages of Electronic Health RecordsKevin DavidNo ratings yet
- Effects of Electronic Charting and Use of The Mar On Amount of Nursing Errors and Quality of Care For PatientsDocument15 pagesEffects of Electronic Charting and Use of The Mar On Amount of Nursing Errors and Quality of Care For Patientsapi-591190687No ratings yet
- Medical Records AutomationDocument6 pagesMedical Records Automationluv2golf67No ratings yet
- Electronic Health Record Syste1Document5 pagesElectronic Health Record Syste1OMONDI VINCENT OmangoNo ratings yet
- Project 2Document13 pagesProject 2Abdulrahaman AbdulraheemNo ratings yet
- Text 2Document9 pagesText 2Alvin Josh CalingayanNo ratings yet
- Secondary Use of Electronic Health RecordDocument19 pagesSecondary Use of Electronic Health RecordRaksha hiwaNo ratings yet
- HCI 540 Final PaperDocument10 pagesHCI 540 Final PaperJulian CorralNo ratings yet
- Electronic Medical Records PaperDocument12 pagesElectronic Medical Records PaperFreshi DemaroNo ratings yet
- Running Head: Computerized Provider Order Entry 1Document9 pagesRunning Head: Computerized Provider Order Entry 1api-509672908No ratings yet
- Nancy Kamau PDFDocument47 pagesNancy Kamau PDFAri Azhari100% (1)
- 1) Identify The Following Impacts of Information Technology in The Society. Give ExamplesDocument14 pages1) Identify The Following Impacts of Information Technology in The Society. Give ExamplesAbeir A. C. SampornaNo ratings yet
- Benefits and Drawbacks of Electronic Health Record SystemsDocument10 pagesBenefits and Drawbacks of Electronic Health Record Systemstylermichael912No ratings yet
- Nursing Informatics 1 - ScribdDocument3 pagesNursing Informatics 1 - ScribdBianca BalmoresNo ratings yet
- Running Head: HEALTHCARE 1Document3 pagesRunning Head: HEALTHCARE 1Makaveli NjugunaNo ratings yet
- Electronic Health Record Management ExpeDocument5 pagesElectronic Health Record Management Expetylermichael912No ratings yet
- Teryn Green Policy Action PlanDocument7 pagesTeryn Green Policy Action Planapi-549106443No ratings yet
- Green 1: RN To BSN Program: Plan of CareDocument4 pagesGreen 1: RN To BSN Program: Plan of Careapi-549106443No ratings yet
- Nursing Research FinalDocument8 pagesNursing Research Finalapi-549106443No ratings yet
- Global Health FinalDocument10 pagesGlobal Health Finalapi-549106443No ratings yet
- Nursing Leadership Theory Paper - FinalDocument8 pagesNursing Leadership Theory Paper - Finalapi-549106443No ratings yet
- Week 5 - Informatics Final PaperDocument11 pagesWeek 5 - Informatics Final Paperapi-549106443No ratings yet
- Kent County Community School Plan of Care For Student PopulationDocument19 pagesKent County Community School Plan of Care For Student Populationapi-549106443No ratings yet
- Nur 300 PhilosophyDocument7 pagesNur 300 Philosophyapi-549106443No ratings yet
- Virtual Reality Operations Training For Oil and Gas by YASSIR SALIHDocument19 pagesVirtual Reality Operations Training For Oil and Gas by YASSIR SALIHusryNo ratings yet
- Is 1231.1974Document22 pagesIs 1231.1974Jayam Harinatha GupthaNo ratings yet
- FPGA DS 02056 4 1 MachXO2 Family Data SheetDocument119 pagesFPGA DS 02056 4 1 MachXO2 Family Data Sheetjoaica5046No ratings yet
- Fixture Inspection ReportDocument1 pageFixture Inspection ReportAvinash Mulik100% (1)
- 1st Place & Galloway Street NE - Appendix ADocument111 pages1st Place & Galloway Street NE - Appendix ADistrict Department of TransportationNo ratings yet
- 9 - TroubleshootingDocument44 pages9 - TroubleshootingMichele Bacocchia100% (1)
- 523A Finals PDFDocument16 pages523A Finals PDFDexter Custodio0% (1)
- Lab12 PDFDocument6 pagesLab12 PDFAmjad ShahzadNo ratings yet
- Att Bill 2020Document6 pagesAtt Bill 2020CARMEN HULTZNo ratings yet
- Removal of Default Vbe 8 - BBB GraphicsDocument4 pagesRemoval of Default Vbe 8 - BBB Graphicsmario nogueraNo ratings yet
- Kinco VFD Cv100Document119 pagesKinco VFD Cv100N.Vijay kumarNo ratings yet
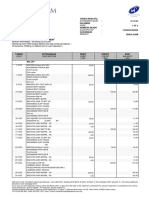
- Estatement-202310 20240118082918Document3 pagesEstatement-202310 20240118082918jooamir70No ratings yet
- VOL 2 SEC 3 1 - SCOPE OF WORKS Rev 2 PDFDocument189 pagesVOL 2 SEC 3 1 - SCOPE OF WORKS Rev 2 PDFsivaguruk250% (2)
- PC Industry Analysis - 2009Document22 pagesPC Industry Analysis - 2009nnshah18No ratings yet
- HP 6220 6050a0066801-Mb-A02 SchematicsDocument68 pagesHP 6220 6050a0066801-Mb-A02 SchematicsGerman ValenciaNo ratings yet
- Lec 1Document45 pagesLec 1JannoNo ratings yet
- A DSL For Collaborative Business ProcessDocument6 pagesA DSL For Collaborative Business ProcesskenNo ratings yet
- Recovering Windows XPDocument43 pagesRecovering Windows XPdavid_kuberaNo ratings yet
- Radar System Using Rduino PDFDocument4 pagesRadar System Using Rduino PDFYasser Auliya PNo ratings yet
- H.R.Steel Industries: Job Card For M 20X2.5X 155 MM Hex Bolt (HSFG)Document1 pageH.R.Steel Industries: Job Card For M 20X2.5X 155 MM Hex Bolt (HSFG)mahesh agarwalNo ratings yet
- RCV STV 2Document1 pageRCV STV 2goss8877No ratings yet
- Mini Project EEE PDFDocument7 pagesMini Project EEE PDFAmit Kr SinghNo ratings yet
- MCBSP SPI TutorialDocument3 pagesMCBSP SPI TutorialS Rizwan HaiderNo ratings yet
- Wi-Fi 6 OFDMA App Notes 091319 WebDocument11 pagesWi-Fi 6 OFDMA App Notes 091319 WebAmir MasoodNo ratings yet
- Memorex MT1191V - MT1131A-32176 PDFDocument23 pagesMemorex MT1191V - MT1131A-32176 PDFdomador1624No ratings yet
- Practical 5: Identify The Business Opportunity Suitable For You. Digital Marketing: A Right Business For Youngster'sDocument5 pagesPractical 5: Identify The Business Opportunity Suitable For You. Digital Marketing: A Right Business For Youngster's02 - CM Ankita AdamNo ratings yet
- Approaches To Design & Implement High Speed-Low Power Digital Filter: ReviewDocument15 pagesApproaches To Design & Implement High Speed-Low Power Digital Filter: ReviewOmran RashNo ratings yet
- 3 - Basics of Electronic CircuitsDocument23 pages3 - Basics of Electronic CircuitsAlisNo ratings yet
- Shichun Yang Xinhua Liu Shen Li Cheng Zhang: Advanced Battery Management System For Electric VehiclesDocument318 pagesShichun Yang Xinhua Liu Shen Li Cheng Zhang: Advanced Battery Management System For Electric VehiclesDennis FielNo ratings yet
- Jet Spray, Warp PrintingDocument3 pagesJet Spray, Warp Printingjoyshree ayekpamNo ratings yet