You might also like
- Fluid Electrolyte Balances and ImbalanceDocument157 pagesFluid Electrolyte Balances and ImbalanceManisha Shakya0% (1)
- Syndrome of Inappropriate Secretion of Anti Diuretic HormoneDocument39 pagesSyndrome of Inappropriate Secretion of Anti Diuretic Hormonefarmasi_hmNo ratings yet
- Chapter 20 - Opthalmic Surgeon On Hong KongDocument6 pagesChapter 20 - Opthalmic Surgeon On Hong KongErica P. Manlunas100% (3)
- How To Make Sodium PerchlorateDocument17 pagesHow To Make Sodium PerchlorateKing90No ratings yet
- CP Kelco - Carrageenan BookDocument28 pagesCP Kelco - Carrageenan BookChee Ghee PingNo ratings yet
- Low Sodium Blood (Hyponatremia) Causes, Symptoms and TreatmentDocument10 pagesLow Sodium Blood (Hyponatremia) Causes, Symptoms and TreatmentMoxie MacadoNo ratings yet
- Alteration in Fluid and Electrolyte ImbalanceDocument118 pagesAlteration in Fluid and Electrolyte ImbalanceRenuga SureshNo ratings yet
- Fluid Electrolyte Imbalance n132 160210135651Document100 pagesFluid Electrolyte Imbalance n132 160210135651Shahan FarooqNo ratings yet
- Lesson 4 - Electrolyte Imbalances Part 1Document74 pagesLesson 4 - Electrolyte Imbalances Part 1Clark SavageNo ratings yet
- Electrolytes Slide 21Document111 pagesElectrolytes Slide 21Elaisha Mae C. CarsulaNo ratings yet
- Electrolytes & FluidimbalancesDocument80 pagesElectrolytes & FluidimbalancesDennis Nyambane MomanyiNo ratings yet
- II. Electrolyte Imbalance: By: Yves Mariel A. Rimando, RN, MN, CNNDocument66 pagesII. Electrolyte Imbalance: By: Yves Mariel A. Rimando, RN, MN, CNNczeremar chanNo ratings yet
- Fluid N Electrolyte BalanceDocument60 pagesFluid N Electrolyte BalanceAnusha Verghese67% (3)
- Hypernatremia: Causes, Symptoms and TreatmentDocument16 pagesHypernatremia: Causes, Symptoms and TreatmentBlessyNo ratings yet
- Pharma ElectrolytesDocument23 pagesPharma ElectrolytesCatherine Martinez AvilaNo ratings yet
- HYPERNATREMIADocument3 pagesHYPERNATREMIAShaira SariaNo ratings yet
- Fluid & Electrolyte Management & Acid Base Disorders: Alice Augustin Amina S Anagha P RDocument47 pagesFluid & Electrolyte Management & Acid Base Disorders: Alice Augustin Amina S Anagha P RAsif AbbasNo ratings yet
- Syndrome of Inapropriate Antidiuretic Hormone (SIADH)Document15 pagesSyndrome of Inapropriate Antidiuretic Hormone (SIADH)Asrul Rahim100% (1)
- Fluid Electrolyte Imbalance NvertedDocument111 pagesFluid Electrolyte Imbalance Nvertedchitrakshi khairnarNo ratings yet
- Hyponatremia: Causes, Evaluation & TreatmentDocument20 pagesHyponatremia: Causes, Evaluation & TreatmentmanjaruNo ratings yet
- Acute Renal FailureDocument30 pagesAcute Renal FailureJerinNo ratings yet
- Diabetes Insipidus: Causes, Symptoms, Diagnosis and TreatmentDocument26 pagesDiabetes Insipidus: Causes, Symptoms, Diagnosis and TreatmentEric Juan MaldiniNo ratings yet
- Drugs Affecting The Renal System I. Diuretics II. Parenteral Fluids (Video) III. Electrolytes (Video)Document44 pagesDrugs Affecting The Renal System I. Diuretics II. Parenteral Fluids (Video) III. Electrolytes (Video)Juliene Hannah FloresNo ratings yet
- electrolytedisturbances-111102083753-phpapp02Document137 pageselectrolytedisturbances-111102083753-phpapp02bobbyfildianNo ratings yet
- Diabetes Insipidus, Siadh and Cerebral Salt-WastingDocument33 pagesDiabetes Insipidus, Siadh and Cerebral Salt-WastingEuphrasiaNo ratings yet
- HyponatremiaDocument21 pagesHyponatremiaselma100% (1)
- Assess & Treat Fluid ImbalanceDocument1 pageAssess & Treat Fluid ImbalanceCharm Dizon BasilioNo ratings yet
- Chronic Kidney DiseaseDocument35 pagesChronic Kidney DiseaseNur'ain Nabila100% (2)
- How To Respond To Abnormal Serum Sodium LevelsDocument3 pagesHow To Respond To Abnormal Serum Sodium LevelsNixNo ratings yet
- Hyponatremia: Q: Discuss Hyponatremia in Clinical PracticeDocument7 pagesHyponatremia: Q: Discuss Hyponatremia in Clinical PracticemyqueenleoNo ratings yet
- Electrolyte Imbalance: Sodium: Submitted By: Milosantos, John Francis D. Tuibeo, Ma. Arlyn P. Yu, Aldrin Anthony LDocument6 pagesElectrolyte Imbalance: Sodium: Submitted By: Milosantos, John Francis D. Tuibeo, Ma. Arlyn P. Yu, Aldrin Anthony Lnospekiko21No ratings yet
- Drugs Acting On The KidneysDocument56 pagesDrugs Acting On The Kidneysbetu tufaNo ratings yet
- Nephrotic Syndrome + ArfDocument64 pagesNephrotic Syndrome + ArfkrishnasreeNo ratings yet
- 09 Diuretics UpdDocument42 pages09 Diuretics UpdYeni Chie Aneuk TuleutNo ratings yet
- ACP Board Review Nephrology 20052ndDocument35 pagesACP Board Review Nephrology 20052nddoctormido2010100% (1)
- Heart Disease Drugs: Cardiac Glycosides, Antihypertensives & DiureticsDocument24 pagesHeart Disease Drugs: Cardiac Glycosides, Antihypertensives & Diureticsblah4020No ratings yet
- Sodium: L.V. Rao, PHDDocument2 pagesSodium: L.V. Rao, PHDAbhilash ReddyNo ratings yet
- Renal Failure Seminar on Acute and Chronic Kidney DiseaseDocument36 pagesRenal Failure Seminar on Acute and Chronic Kidney Diseasesanangamba akhamNo ratings yet
- Hypernatremia: Marielle Adey R. Magcawas BSN-3CDocument28 pagesHypernatremia: Marielle Adey R. Magcawas BSN-3CMarielle Adey Magcawas RNNo ratings yet
- Fluidsandelectrolytes 090224074347 Phpapp02Document102 pagesFluidsandelectrolytes 090224074347 Phpapp02IsaacJ22No ratings yet
- Diabetes InsipidusDocument17 pagesDiabetes InsipidusAditya PrambudhiNo ratings yet
- Fluid and Electrolyte BalanceDocument52 pagesFluid and Electrolyte BalanceFrancis Appau100% (1)
- Fluid and Electrolyte Imbalances Part 2Document46 pagesFluid and Electrolyte Imbalances Part 2Gabrielle Frances FernandezNo ratings yet
- Sodium & Water Disorders: Understanding Hyponatremia and HypernatremiaDocument39 pagesSodium & Water Disorders: Understanding Hyponatremia and HypernatremiaManhal A AbdulkaderNo ratings yet
- Chronic Renal FailureDocument3 pagesChronic Renal FailureJashine DajayNo ratings yet
- Sodium Chloride (Nacl)Document1 pageSodium Chloride (Nacl)Sandrine BarredoNo ratings yet
- FLUIDS AND ELECTROLYTES MNGTDocument44 pagesFLUIDS AND ELECTROLYTES MNGTremerose100% (1)
- Acute Renal FailureDocument11 pagesAcute Renal FailuregeorgejobinputhenpurackalNo ratings yet
- Diuretic Agents Mechanisms and Nursing CareDocument42 pagesDiuretic Agents Mechanisms and Nursing CareKumah WisdomNo ratings yet
- Neuroimaging and DNA Profiling New AvenuesDocument52 pagesNeuroimaging and DNA Profiling New AvenuesDr-Ajay TripathiNo ratings yet
- Drugs Acting On Renal SystemDocument98 pagesDrugs Acting On Renal SystemIsmael JaaniNo ratings yet
- Fluid and Electrolyte ImbalanceDocument29 pagesFluid and Electrolyte ImbalancePrincewill SeiyefaNo ratings yet
- Diabetes Insipidus: Nitha K 2 Year MSC NursingDocument47 pagesDiabetes Insipidus: Nitha K 2 Year MSC NursingNITHA K100% (1)
- Fluid and Elctrolyte Balance.... Power PointDocument40 pagesFluid and Elctrolyte Balance.... Power PointMarwan M.100% (1)
- Case Study: Hyponatremia: Bicol University College of NursingDocument34 pagesCase Study: Hyponatremia: Bicol University College of NursingDaniel Angelo ArangoNo ratings yet
- ANNEDocument5 pagesANNEapi-3759646No ratings yet
- Electrolyte Imbalances and Their Management.: by Nabawanda Saluwa Facilitator: DR - Ssebuliba MosesDocument44 pagesElectrolyte Imbalances and Their Management.: by Nabawanda Saluwa Facilitator: DR - Ssebuliba MosesNinaNo ratings yet
- ElectddrolyDocument5 pagesElectddrolyapi-3759646No ratings yet
- Brain Dump NUR 213 FINALDocument37 pagesBrain Dump NUR 213 FINALkelsey jackson100% (1)
- Fluid and Electrolyte - 2022Document147 pagesFluid and Electrolyte - 2022Lacangan, Thea YvonneNo ratings yet
- Guideline, Management of HypernatremiaDocument9 pagesGuideline, Management of HypernatremiaLia Safitri Leloly100% (1)
- Fluid & Electrolyte ImbalanceDocument37 pagesFluid & Electrolyte ImbalanceoutkastedNo ratings yet
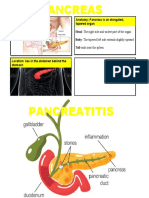
- Anatomy: Pancreas Is An Elongated, Tapered OrganDocument2 pagesAnatomy: Pancreas Is An Elongated, Tapered OrganErica P. ManlunasNo ratings yet
- Abdominal Aortic Aneurysmn FINAL WORDDocument16 pagesAbdominal Aortic Aneurysmn FINAL WORDErica P. ManlunasNo ratings yet
- Abdominal Aortic Aneurysm and Atherosclerosis FINALDocument23 pagesAbdominal Aortic Aneurysm and Atherosclerosis FINALErica P. ManlunasNo ratings yet
- Presentation 1Document2 pagesPresentation 1Erica P. ManlunasNo ratings yet
- New Case TitleDocument2 pagesNew Case TitleErica P. ManlunasNo ratings yet
- Introduction For ElectrolytesDocument1 pageIntroduction For ElectrolytesErica P. ManlunasNo ratings yet
- Chapter 20: Opthalmic Surgeon in Hong Kong (1891-92)Document4 pagesChapter 20: Opthalmic Surgeon in Hong Kong (1891-92)Erica P. ManlunasNo ratings yet
- Erica P. Manlunas - Tools Used in Community Diagnosis UpdateDocument2 pagesErica P. Manlunas - Tools Used in Community Diagnosis UpdateErica P. ManlunasNo ratings yet
- IntroductionDocument1 pageIntroductionErica P. ManlunasNo ratings yet
- Week 5 NCPDocument1 pageWeek 5 NCPErica P. ManlunasNo ratings yet
- C1-Attitude and Awareness of Vaccination Program in Municipality of Antipas Among Millennial Generation 2Document5 pagesC1-Attitude and Awareness of Vaccination Program in Municipality of Antipas Among Millennial Generation 2Erica P. ManlunasNo ratings yet
- Erica P. Manlunas - Tools Used in Community Diagnosis UpdateDocument2 pagesErica P. Manlunas - Tools Used in Community Diagnosis UpdateErica P. ManlunasNo ratings yet
- Chapter 20: Opthalmic Surgeon in Hong Kong (1891-92)Document4 pagesChapter 20: Opthalmic Surgeon in Hong Kong (1891-92)Erica P. ManlunasNo ratings yet
- OrdersDocument1 pageOrdersErica P. ManlunasNo ratings yet
- Erica P. Manlunas - Tools Used in Community Diagnosis UpdateDocument2 pagesErica P. Manlunas - Tools Used in Community Diagnosis UpdateErica P. ManlunasNo ratings yet
- C1-Attitude and Awareness of Vaccination Program in Municipality of Antipas Among Millennial Generation 2Document5 pagesC1-Attitude and Awareness of Vaccination Program in Municipality of Antipas Among Millennial Generation 2Erica P. ManlunasNo ratings yet
- Week 5 NCPDocument1 pageWeek 5 NCPErica P. ManlunasNo ratings yet
- Erica P. Manlunas - Tools Used in Community Diagnosis UpdateDocument2 pagesErica P. Manlunas - Tools Used in Community Diagnosis UpdateErica P. ManlunasNo ratings yet
- WEEK 5 Management of Patients With Fluids and ElectrolytesDocument89 pagesWEEK 5 Management of Patients With Fluids and ElectrolytesErica P. ManlunasNo ratings yet
- Abdominal Aortic Aneurysmn FINAL WORDDocument16 pagesAbdominal Aortic Aneurysmn FINAL WORDErica P. ManlunasNo ratings yet
- Abdominal Aortic Aneurysmn FINAL WORDDocument16 pagesAbdominal Aortic Aneurysmn FINAL WORDErica P. ManlunasNo ratings yet
- Chapter 20: Opthalmic Surgeon in Hong Kong (1891-92)Document4 pagesChapter 20: Opthalmic Surgeon in Hong Kong (1891-92)Erica P. ManlunasNo ratings yet
- Erica P. Manlunas - Tools Used in Community Diagnosis UpdateDocument2 pagesErica P. Manlunas - Tools Used in Community Diagnosis UpdateErica P. ManlunasNo ratings yet
- Introduction For ElectrolytesDocument1 pageIntroduction For ElectrolytesErica P. ManlunasNo ratings yet
- After Writing Chapter 2, Remind Ma'am How To Make TitleDocument1 pageAfter Writing Chapter 2, Remind Ma'am How To Make TitleErica P. ManlunasNo ratings yet
- Introduction For ElectrolytesDocument1 pageIntroduction For ElectrolytesErica P. ManlunasNo ratings yet
- Abdominal Aortic Aneurysmn FINAL WORDDocument16 pagesAbdominal Aortic Aneurysmn FINAL WORDErica P. ManlunasNo ratings yet
- After Writing Chapter 2, Remind Ma'am How To Make TitleDocument1 pageAfter Writing Chapter 2, Remind Ma'am How To Make TitleErica P. ManlunasNo ratings yet
- 7 35Document29 pages7 35nandagamersNo ratings yet
- FMDC Past Paper PakLearningSpotDocument17 pagesFMDC Past Paper PakLearningSpotMuneeb UlHasaanNo ratings yet
- Snell 1931Document5 pagesSnell 1931MANDALIKA AYUSTI NAWANGSARI -No ratings yet
- NomenclatureDocument14 pagesNomenclatureAzeem KahlonNo ratings yet
- Patent for Preparing Ergot Alkaloids from Saprophytic CultureDocument4 pagesPatent for Preparing Ergot Alkaloids from Saprophytic CultureSmokeNo ratings yet
- Chjv01i04p0209 PDFDocument11 pagesChjv01i04p0209 PDFchemistryjournalNo ratings yet
- ၂၀၁၄ တကၠသိုလ္ဝင္စာေမးပြဲ မေကြး ဓာတုေဗဒေမးခြန္းDocument4 pages၂၀၁၄ တကၠသိုလ္ဝင္စာေမးပြဲ မေကြး ဓာတုေဗဒေမးခြန္းKyi Htin PawNo ratings yet
- Hydrochemical Assessment of SW and GW Quality Along Uyyakondan ChannelDocument13 pagesHydrochemical Assessment of SW and GW Quality Along Uyyakondan ChannelbrindhaNo ratings yet
- 2 The Alkali and Alkaline Earth Metals PDFDocument9 pages2 The Alkali and Alkaline Earth Metals PDFAdnan DeparNo ratings yet
- Column Manual: Metrosep A Supp 4 (6.1006.XX0 / 6.01021.XX0)Document50 pagesColumn Manual: Metrosep A Supp 4 (6.1006.XX0 / 6.01021.XX0)LollipopNo ratings yet
- 9572 BiochemistryDocument414 pages9572 Biochemistrymaryam100% (9)
- CQ BleachDocument7 pagesCQ Bleachapi-3826629No ratings yet
- Ingredients to avoid or look for in natural hair careDocument4 pagesIngredients to avoid or look for in natural hair careEllenOliveiraNo ratings yet
- One Bath One Stage Dyeing of Polyester/Cellulosic Blends Using Disperse and Reactive DyesDocument31 pagesOne Bath One Stage Dyeing of Polyester/Cellulosic Blends Using Disperse and Reactive Dyessanjay shettiNo ratings yet
- Aquaculture Probiotics Manufacturers in India - Finar ChemicalsDocument44 pagesAquaculture Probiotics Manufacturers in India - Finar Chemicalsfinar chemicalsNo ratings yet
- Sodium Methylate-Msds Green CatalystsDocument3 pagesSodium Methylate-Msds Green CatalystsBen Yudha SatriaNo ratings yet
- 32 20 01Document2 pages32 20 01acetonafloresNo ratings yet
- CH 3 Chemical Reaction Worksheet 1Document19 pagesCH 3 Chemical Reaction Worksheet 1Alia ShabbirNo ratings yet
- Keshe Foundation Micro Plasma Energy Reactor, European Patent Filing, Patent Application Number 05447236.0Document17 pagesKeshe Foundation Micro Plasma Energy Reactor, European Patent Filing, Patent Application Number 05447236.0American Kabuki100% (4)
- BS 812-118 1988 Sulphate Content硫酸盐含量Document15 pagesBS 812-118 1988 Sulphate Content硫酸盐含量yangNo ratings yet
- Identifying Contaminants in SoilDocument7 pagesIdentifying Contaminants in SoilJivitesh SharmaNo ratings yet
- Samplenote 0620 Chemistry Paper 6 Kit 1564557209 5d413f990a27b 1596Document4 pagesSamplenote 0620 Chemistry Paper 6 Kit 1564557209 5d413f990a27b 1596da_reaper_dasNo ratings yet
- PharmaceuticsDocument52 pagesPharmaceuticsl3948380No ratings yet
- Complete Chem (6) 44-61 - 20200428 - 0001Document18 pagesComplete Chem (6) 44-61 - 20200428 - 0001Wisdom PhanganNo ratings yet
- Importance of Sequestering Agent in Textile ProcessingDocument2 pagesImportance of Sequestering Agent in Textile ProcessingKushagradhi DebnathNo ratings yet
- PERIOD 3 OXIDE PROPERTIESDocument6 pagesPERIOD 3 OXIDE PROPERTIESCHEE HONG CHANNo ratings yet
- RthyyDocument19 pagesRthyyXazerco LaxNo ratings yet