You might also like
- Icelandic Spells and SigilsDocument16 pagesIcelandic Spells and SigilsSimonida Mona Vulić83% (6)
- Serv7107 V05N01 TXT7Document32 pagesServ7107 V05N01 TXT7azry_alqadry100% (6)
- Banu Maaruf of The LevantDocument6 pagesBanu Maaruf of The LevantMotiwala AbbasNo ratings yet
- SHORT STORY Manhood by John Wain - Lindsay RossouwDocument17 pagesSHORT STORY Manhood by John Wain - Lindsay RossouwPrincess67% (3)
- PBS-P100 Facilities Standards GuideDocument327 pagesPBS-P100 Facilities Standards Guidecessna5538cNo ratings yet
- Flexible Ductwork Report - November 2011v2Document69 pagesFlexible Ductwork Report - November 2011v2bommobNo ratings yet
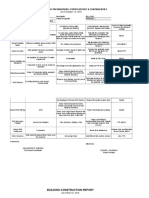
- Class Opening Preparations Status ReportDocument3 pagesClass Opening Preparations Status ReportMaria Theresa Buscato86% (7)
- Building and Enhancing New Literacies Across The CurriculumDocument119 pagesBuilding and Enhancing New Literacies Across The CurriculumLowela Kasandra100% (3)
- (PDF) Biochemistry and Molecular Biology of Plants: Book DetailsDocument1 page(PDF) Biochemistry and Molecular Biology of Plants: Book DetailsArchana PatraNo ratings yet
- Nutrition StudDocument7 pagesNutrition StudfeelanNo ratings yet
- 184-Article Text - 797-1-10-20151013Document5 pages184-Article Text - 797-1-10-20151013Bushra KainaatNo ratings yet
- Assessment of Pregnant Women's Knowledge, Attitude, and Practice Regarding Pregnancy Nutrition at A Tertiary Care HospitalDocument6 pagesAssessment of Pregnant Women's Knowledge, Attitude, and Practice Regarding Pregnancy Nutrition at A Tertiary Care HospitalInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- 1 PBDocument10 pages1 PBLabiba AkyasNo ratings yet
- Relationship Between Calcium Supplementation Dose and Vegetable Intake With PreeclampsiaDocument7 pagesRelationship Between Calcium Supplementation Dose and Vegetable Intake With PreeclampsiaBrevi Istu PambudiNo ratings yet
- Knowledge and attitude of primigravida mothers regarding antenatal dietDocument6 pagesKnowledge and attitude of primigravida mothers regarding antenatal dietNeha RanaNo ratings yet
- Parenteral Nutrition Patients: ObstetricDocument14 pagesParenteral Nutrition Patients: ObstetricAripinSyarifudinNo ratings yet
- Jurnal Terbaru GiziDocument11 pagesJurnal Terbaru GiziTasarane AngelNo ratings yet
- Naskah PublikasiDocument12 pagesNaskah PublikasiRatihWulandariNo ratings yet
- Maternal and Early-Life Nutrition and HealthDocument4 pagesMaternal and Early-Life Nutrition and HealthTiffani_Vanessa01No ratings yet
- OK - EJMED KakfitDocument5 pagesOK - EJMED Kakfitl_bajakanNo ratings yet
- Nutrients 09 00221 v2Document11 pagesNutrients 09 00221 v2Firman FajriNo ratings yet
- UEU Undergraduate 12789 MANUSKRIP - Image.MarkedDocument12 pagesUEU Undergraduate 12789 MANUSKRIP - Image.MarkedRian PNo ratings yet
- Assessment of Nutrition Profile of Pregnant Women in Rural Area (Mymensingh District) of BangladeshDocument6 pagesAssessment of Nutrition Profile of Pregnant Women in Rural Area (Mymensingh District) of BangladeshKanhiya MahourNo ratings yet
- nutritional-risk-in-hospitalized-pregnant-wome_english_translatedDocument6 pagesnutritional-risk-in-hospitalized-pregnant-wome_english_translatedTrang KiềuNo ratings yet
- 60f19c6083673.chang Tan ADocument12 pages60f19c6083673.chang Tan AS. M.No ratings yet
- International Journal of Health Sciences and Research: Maternal Nutritional Status and Its Relation With Birth WeightDocument12 pagesInternational Journal of Health Sciences and Research: Maternal Nutritional Status and Its Relation With Birth WeightimeldafitriNo ratings yet
- Sefita@unpad - Ac.id: AbstrakDocument4 pagesSefita@unpad - Ac.id: AbstrakSaskia 17No ratings yet
- 1 PBDocument4 pages1 PBNeny OraNo ratings yet
- Pengetahuan, Sikap, Perilaku, Dan Asupan Gizi Berdasarkan Status Hidrasi Ibu HamilDocument9 pagesPengetahuan, Sikap, Perilaku, Dan Asupan Gizi Berdasarkan Status Hidrasi Ibu HamilSyntia AsunaNo ratings yet
- The Dietary Intake of Two Groups of Lactating Women in Shanghai During The PuerperiumDocument10 pagesThe Dietary Intake of Two Groups of Lactating Women in Shanghai During The PuerperiumtraphuongNo ratings yet
- Hapzah, Veni Hadju, Saifuddin Sirajuddin: Artikel PenelitianDocument7 pagesHapzah, Veni Hadju, Saifuddin Sirajuddin: Artikel PenelitianDewiNo ratings yet
- Jurnal Gizi Indonesia (The Indonesian Journal of Nutrition)Document10 pagesJurnal Gizi Indonesia (The Indonesian Journal of Nutrition)Maria NeleNo ratings yet
- Nutrient Intake of Pregnant Women in Indonesia: A Review: Malaysian Journal of Nutrition April 2012Document13 pagesNutrient Intake of Pregnant Women in Indonesia: A Review: Malaysian Journal of Nutrition April 2012BamwinataNo ratings yet
- 172-Article Text-698-1-10-20191111Document8 pages172-Article Text-698-1-10-20191111ENdank SyurianiiNo ratings yet
- Intl J Gynecology Obste - 2020 - Killeen - Examining The Use of The FIGO Nutrition Checklist in Routine AntenatalDocument6 pagesIntl J Gynecology Obste - 2020 - Killeen - Examining The Use of The FIGO Nutrition Checklist in Routine AntenatalBenk Setsuna F. SeieiNo ratings yet
- 1 PBDocument6 pages1 PBShelamita ImanisaNo ratings yet
- Assessment of Dietary Intake Among PregnDocument9 pagesAssessment of Dietary Intake Among PregnBushra KainaatNo ratings yet
- Effect of Counseling On Nutritional StatusDocument6 pagesEffect of Counseling On Nutritional StatuseunisflammeNo ratings yet
- Suplementasi Vitamin A Dan Asupan Zat Gizi Dengan Serum Retinol Dan Morbiditas Anak 1-3 TahunDocument9 pagesSuplementasi Vitamin A Dan Asupan Zat Gizi Dengan Serum Retinol Dan Morbiditas Anak 1-3 TahundhannylagarenseNo ratings yet
- Malnutrition During Pregnancy Among Child BearingDocument6 pagesMalnutrition During Pregnancy Among Child BearingR&T FamilyNo ratings yet
- Women Beliefs & Practices Regarding Food During Pregnancy - A Hospital Based Study"Document7 pagesWomen Beliefs & Practices Regarding Food During Pregnancy - A Hospital Based Study"ayrahma29No ratings yet
- 1 PB PDFDocument12 pages1 PB PDFMegayana Yessy MarettaNo ratings yet
- Regular Egg Consumption at Breakfast by Japanese Woman University Students Improves Daily Nutrient Intakes: Open-Labeled ObservationsDocument7 pagesRegular Egg Consumption at Breakfast by Japanese Woman University Students Improves Daily Nutrient Intakes: Open-Labeled ObservationsLeena MuniandyNo ratings yet
- The Relationship Between Dietary Patterns and Nutritional Knowledge With The Nutritional Status of Bajo Tribe Pregnant Women in Duruka District, Muna RegencyDocument5 pagesThe Relationship Between Dietary Patterns and Nutritional Knowledge With The Nutritional Status of Bajo Tribe Pregnant Women in Duruka District, Muna RegencytreesNo ratings yet
- 2018-KnE Life Sciences (Publisher)Document7 pages2018-KnE Life Sciences (Publisher)Muhamad Jauhar S.Kep., Ners, M.KepNo ratings yet
- AASP Chandradewi 1391 1402 PDFDocument12 pagesAASP Chandradewi 1391 1402 PDFDede KusmawanNo ratings yet
- Konsumsi Makronutrien Pada Ibu Hamil Kekurangan Energi Kronik (Kek) Di Masa Pandemi Covid-19Document6 pagesKonsumsi Makronutrien Pada Ibu Hamil Kekurangan Energi Kronik (Kek) Di Masa Pandemi Covid-19Leni MarlinaNo ratings yet
- Pregnant Women's Nutritional Status Identified Based on Arm Circumference, BMI, and Weight GainDocument8 pagesPregnant Women's Nutritional Status Identified Based on Arm Circumference, BMI, and Weight GainRisma Ripfandiana SariNo ratings yet
- Asemi and Esmaillzadeh, 2015Document7 pagesAsemi and Esmaillzadeh, 2015Anindita BatabyalNo ratings yet
- Hamil Wilayah: Antara Konsumsi Energi Protein Dengan Gizi IBU Kerja SukoharjoDocument10 pagesHamil Wilayah: Antara Konsumsi Energi Protein Dengan Gizi IBU Kerja Sukoharjojulfandi kuncoroNo ratings yet
- Food Suggestions, Meal Frequency and Dietary Diversity Among Pregnant Women A Quantitative StudyDocument12 pagesFood Suggestions, Meal Frequency and Dietary Diversity Among Pregnant Women A Quantitative Studyrian dianaNo ratings yet
- Research Article: Do Maternal Vitamin D Levels Influence Vitamin D Levels in Preterm Neonates?Document8 pagesResearch Article: Do Maternal Vitamin D Levels Influence Vitamin D Levels in Preterm Neonates?bellaNo ratings yet
- 77-Article Text-726-1-10-20210128Document20 pages77-Article Text-726-1-10-20210128ShafaNo ratings yet
- Daniels, 2019 - Micronutrient Intakes of Lactating Mothers and Their Association With Breast Milk Concentrations and Micronutrient Adequacy of Exclusively Breastfed Indonesian InfantsDocument10 pagesDaniels, 2019 - Micronutrient Intakes of Lactating Mothers and Their Association With Breast Milk Concentrations and Micronutrient Adequacy of Exclusively Breastfed Indonesian Infantsdiana.alyNo ratings yet
- Nutritional Status of Prepregnant and Pregnant Women Residing in Bogor District Indonesia A Crosssectional Dietary and Nutrient Intake StudyDocument10 pagesNutritional Status of Prepregnant and Pregnant Women Residing in Bogor District Indonesia A Crosssectional Dietary and Nutrient Intake Studyston777No ratings yet
- Nutrisi Ibu HmilDocument8 pagesNutrisi Ibu HmilChila RegitaNo ratings yet
- BSC Project FinalDocument56 pagesBSC Project FinalNgenyi Chiaritta100% (1)
- Pengaruh Pemberian Makanan Tambahan Terhadap Peningkatan Berat Badan Ibu Hamil Kek (Kurang Energi Kronis) Di Wilayah Kerja Puskesmas Labuan LombokDocument12 pagesPengaruh Pemberian Makanan Tambahan Terhadap Peningkatan Berat Badan Ibu Hamil Kek (Kurang Energi Kronis) Di Wilayah Kerja Puskesmas Labuan LombokRia DestrianiNo ratings yet
- Malnutrition During Pregnancy Among Child Bearing Mothers in Mbaitolu of South-Eastern NigeriaDocument5 pagesMalnutrition During Pregnancy Among Child Bearing Mothers in Mbaitolu of South-Eastern NigeriaEka Rosiana DewiNo ratings yet
- Anaemia in Pregnancy: WelcomeDocument25 pagesAnaemia in Pregnancy: WelcomeDelphy VargheseNo ratings yet
- Effectiveness of Nutritional Supplementation During The - 2022 - The Lancet RegDocument11 pagesEffectiveness of Nutritional Supplementation During The - 2022 - The Lancet RegCawee CawNo ratings yet
- Effect of Nutrition Education On Hemoglobin Level in Pregnant Women: A Quasi-Experimental StudyDocument12 pagesEffect of Nutrition Education On Hemoglobin Level in Pregnant Women: A Quasi-Experimental StudyRidwan SyalwacesarioNo ratings yet
- ajcn-2Fnqz047Document10 pagesajcn-2Fnqz047agung krisNo ratings yet
- 2022 - The Importance of Nutrition in Pregnancy and Lactation - Lifelong ConsequencesDocument26 pages2022 - The Importance of Nutrition in Pregnancy and Lactation - Lifelong ConsequencesjacquelineNo ratings yet
- Beliefs and Practices Regarding Nutrition During Pregnancy and Lactation in A Rural Area in Karnataka, India: A Qualitative StudyDocument5 pagesBeliefs and Practices Regarding Nutrition During Pregnancy and Lactation in A Rural Area in Karnataka, India: A Qualitative StudyNishaNo ratings yet
- Nutritional Requirements OverviewDocument6 pagesNutritional Requirements OverviewKoriaNo ratings yet
- Bahasa Indonesia1Document9 pagesBahasa Indonesia1lucia listaNo ratings yet
- Nutrients 04 01958Document19 pagesNutrients 04 01958Wahyu Arief MahatmaNo ratings yet
- Membandingkan Recall 24 Jam Nutri Survey Dengan TkpiDocument7 pagesMembandingkan Recall 24 Jam Nutri Survey Dengan TkpiFransisca SihotangNo ratings yet
- 1571-1635319494618-Unit 04 Leadership and ManagementDocument48 pages1571-1635319494618-Unit 04 Leadership and ManagementdevindiNo ratings yet
- IPO Fact Sheet - Accordia Golf Trust 140723Document4 pagesIPO Fact Sheet - Accordia Golf Trust 140723Invest StockNo ratings yet
- Hisar CFC - Approved DPRDocument126 pagesHisar CFC - Approved DPRSATYAM KUMARNo ratings yet
- BOQ - Hearts & Arrows Office 04sep2023Document15 pagesBOQ - Hearts & Arrows Office 04sep2023ChristianNo ratings yet
- PropensityModels PDFDocument4 pagesPropensityModels PDFSarbarup BanerjeeNo ratings yet
- Bhakti Trader Ram Pal JiDocument232 pagesBhakti Trader Ram Pal JiplancosterNo ratings yet
- 02 MortarsDocument2 pages02 MortarsTarun kumar DigarseNo ratings yet
- Useful Relations in Quantum Field TheoryDocument30 pagesUseful Relations in Quantum Field TheoryDanielGutierrez100% (1)
- United Airlines Case Study: Using Marketing to Address External ChallengesDocument4 pagesUnited Airlines Case Study: Using Marketing to Address External ChallengesSakshiGuptaNo ratings yet
- Hydrocarbon: Understanding HydrocarbonsDocument9 pagesHydrocarbon: Understanding HydrocarbonsBari ArouaNo ratings yet
- Inventory Storage and Retrieval System PatentDocument15 pagesInventory Storage and Retrieval System PatentdevanasokaNo ratings yet
- Polygenic InheritanceDocument13 pagesPolygenic InheritanceSandeep Kumar RaghuvanshiNo ratings yet
- Presentation 1Document20 pagesPresentation 1nikitakhanduja1304No ratings yet
- Oas Community College: Republic of The Philippines Commission On Higher Education Oas, AlbayDocument22 pagesOas Community College: Republic of The Philippines Commission On Higher Education Oas, AlbayJaycel NepalNo ratings yet
- Biamp Vocia Catalog Apr2020Document24 pagesBiamp Vocia Catalog Apr2020Mahavir Shantilal DhokaNo ratings yet
- Ahu, Chiller, Fcu Technical Bid TabulationDocument15 pagesAhu, Chiller, Fcu Technical Bid TabulationJohn Henry AsuncionNo ratings yet
- How Do I Prepare For Public Administration For IAS by Myself Without Any Coaching? Which Books Should I Follow?Document3 pagesHow Do I Prepare For Public Administration For IAS by Myself Without Any Coaching? Which Books Should I Follow?saiviswanath0990100% (1)
- Oral Medication PharmacologyDocument4 pagesOral Medication PharmacologyElaisa Mae Delos SantosNo ratings yet
- Smoktech Vmax User ManualDocument9 pagesSmoktech Vmax User ManualStella PapaNo ratings yet
- Translation of Japanese Onomatopoeia Into Swedish (With Focus On Lexicalization)Document20 pagesTranslation of Japanese Onomatopoeia Into Swedish (With Focus On Lexicalization)Aldandy OckadeyaNo ratings yet