You might also like
- Growth FactorsFrom EverandGrowth FactorsChoh Hao LiNo ratings yet
- Hair Loss PDFDocument64 pagesHair Loss PDFWilliam WongNo ratings yet
- Anti-Anginal DrugsDocument39 pagesAnti-Anginal Drugspoonam rana100% (1)
- Zero Sum Fun LiteDocument8 pagesZero Sum Fun LiteNguyễn Xuân YênNo ratings yet
- Triage Made EasyDocument7 pagesTriage Made EasyCamille Lou Cariaga AbellaNo ratings yet
- Plan 415Document20 pagesPlan 415Eduardo Dutra100% (1)
- Trend Continuation PatternDocument11 pagesTrend Continuation PatternIFCMarketsNo ratings yet
- Bikash Kumar Sah 2 Semester PucmasDocument22 pagesBikash Kumar Sah 2 Semester PucmasBikash SahNo ratings yet
- Inhaler DosingjjDocument2 pagesInhaler Dosingjjkhangsiean89No ratings yet
- Kuliah HyperthyroidDocument18 pagesKuliah HyperthyroidFreddyNo ratings yet
- Lecture 15-Autoimmune Disease of The Skin-Hardyanto Soebono (2017)Document58 pagesLecture 15-Autoimmune Disease of The Skin-Hardyanto Soebono (2017)Alfina MeidinaNo ratings yet
- Ant. Pituitary Hormones: 1. Growth HormoneDocument21 pagesAnt. Pituitary Hormones: 1. Growth HormoneGriffinNo ratings yet
- Glimepiride Vs Gliclazide in Dm2 - PHC - Medicine Review - January2014Document5 pagesGlimepiride Vs Gliclazide in Dm2 - PHC - Medicine Review - January2014Manik ANo ratings yet
- HYPOTHYROIDISMDocument30 pagesHYPOTHYROIDISMTopeNo ratings yet
- Pathways of Invasion in Laryngeal CancerDocument5 pagesPathways of Invasion in Laryngeal CancerJaspreet SinghNo ratings yet
- Vanadium Pentoxide MsdsDocument6 pagesVanadium Pentoxide Msdschiang95No ratings yet
- Emsella TreatmentDocument1 pageEmsella TreatmentLiana ZainalNo ratings yet
- Chapter 4 Sent DRMDocument41 pagesChapter 4 Sent DRMSarvar PathanNo ratings yet
- How To Make Momey SummeryDocument11 pagesHow To Make Momey SummeryPriyanka BhattacharjeeNo ratings yet
- Terms and Jargons For Trading by EmperorBTCDocument9 pagesTerms and Jargons For Trading by EmperorBTCsaptovicnemanjaNo ratings yet
- Iraqi Guidelines For CCHF ManagementDocument23 pagesIraqi Guidelines For CCHF ManagementMasod Haji100% (1)
- Hypertension GuidelinesDocument33 pagesHypertension GuidelinesErlinda NRANo ratings yet
- The Break and Retest Setup by SCALPSNIPERDocument2 pagesThe Break and Retest Setup by SCALPSNIPERsanou Sidibe100% (1)
- Sepsis 3 PDFDocument10 pagesSepsis 3 PDFFayeListancoNo ratings yet
- Top 10 Technical Indicators For Agri Commodity Market Part 1Document40 pagesTop 10 Technical Indicators For Agri Commodity Market Part 1sharathNo ratings yet
- CBG Coverage CBG Coverage: Actrapid Sliding ScaleDocument10 pagesCBG Coverage CBG Coverage: Actrapid Sliding ScaleSerious LeoNo ratings yet
- 6-10 Telecentre Entrepreneur Course Answer Key 2020 - Any Time TipsDocument12 pages6-10 Telecentre Entrepreneur Course Answer Key 2020 - Any Time Tipsvikash kumar100% (1)
- AntiretroviralDocument14 pagesAntiretroviralSeffia riandiniNo ratings yet
- Surviving Sepsis Campaign3Document43 pagesSurviving Sepsis Campaign3Dr.Talal Aljuhani100% (1)
- Davit Pivot Zone Introduction Worksheet Trade EvaluationDocument1 pageDavit Pivot Zone Introduction Worksheet Trade EvaluationIsabelo AbaoNo ratings yet
- MLC Protocols and Its Awareness Among Dental Professionals - A ReviewDocument4 pagesMLC Protocols and Its Awareness Among Dental Professionals - A ReviewInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Falls Risk and Medication: Selina Khanom: Dementia Team PharmacistDocument29 pagesFalls Risk and Medication: Selina Khanom: Dementia Team PharmacistSyahrial100% (1)
- Acute Coronary Syndrome (Acs) : DR M. Arman Nasution SPPDDocument162 pagesAcute Coronary Syndrome (Acs) : DR M. Arman Nasution SPPDfifahNo ratings yet
- Guppy PDFDocument7 pagesGuppy PDFEdouard YaoNo ratings yet
- Phase III Clinical Trials - 2014-15Document23 pagesPhase III Clinical Trials - 2014-15Ali TasleemNo ratings yet
- The Endocrine Functions of The Pancreas4923 160122104950Document26 pagesThe Endocrine Functions of The Pancreas4923 160122104950Nancy Akunna100% (1)
- Burkitt LymphomaDocument51 pagesBurkitt LymphomaDee100% (2)
- BuySell2.0 Installation GuideDocument2 pagesBuySell2.0 Installation Guiderodrigo250No ratings yet
- FXT50 - System ManualDocument14 pagesFXT50 - System ManualZakaria Yusof100% (2)
- Selecting Dynamic Moving Average Trading Rules in The Crude Oil Futures Market Using A Genetic ApproachDocument11 pagesSelecting Dynamic Moving Average Trading Rules in The Crude Oil Futures Market Using A Genetic ApproachMicael GomesNo ratings yet
- Maternity Benefit Act, 1961Document22 pagesMaternity Benefit Act, 1961bijuanithaNo ratings yet
- 1.4A Lipid ChemistryDocument12 pages1.4A Lipid ChemistryBea SamonteNo ratings yet
- Prostaglandin E2Document7 pagesProstaglandin E2Tanasescu MariusNo ratings yet
- Sepsis - 3Document36 pagesSepsis - 3Mohd Ekhwan DarusNo ratings yet
- Anemia OutlineDocument3 pagesAnemia Outlinekaylakmills_10135868No ratings yet
- Scalp PDFDocument7 pagesScalp PDFduranduran11No ratings yet
- 04 - 05 - Option Strategies & Payoff'sDocument66 pages04 - 05 - Option Strategies & Payoff'sMohammedAveshNagoriNo ratings yet
- NR 446 Week 6 ATI Weekly Tips Mental HealthDocument16 pagesNR 446 Week 6 ATI Weekly Tips Mental HealthChristine LansdownNo ratings yet
- High Dose Intravenous Vitamin C Treatment For Zika FeverDocument4 pagesHigh Dose Intravenous Vitamin C Treatment For Zika FeverEliza LlenzaNo ratings yet
- Clinical Management of DiabetesDocument122 pagesClinical Management of DiabetesViju K GNo ratings yet
- Examining TD Lines - Conditions of Use of TD Demand Line PDFDocument11 pagesExamining TD Lines - Conditions of Use of TD Demand Line PDFWalter KovacsNo ratings yet
- FX Cog MasterDocument19 pagesFX Cog MasterNarashimma Kumar100% (1)
- Emeset MedicalDocument16 pagesEmeset MedicalSwapnil PatilNo ratings yet
- Lipid Movement BiochemDocument9 pagesLipid Movement BiochemCrowNo ratings yet
- FibonnacciDocument13 pagesFibonnacciCaitlin WenkeNo ratings yet
- 5 Pro Strategies To WealthDocument7 pages5 Pro Strategies To WealthΣπύρος ΚασιμάτηςNo ratings yet
- National Guideline On Diabetes Mellitus, First Edition 2023Document116 pagesNational Guideline On Diabetes Mellitus, First Edition 2023Zohra AfrozNo ratings yet
- Adrenocortical HyperfunctionDocument132 pagesAdrenocortical Hyperfunctionshobharamkrishna100% (2)
- Nail DisorderDocument37 pagesNail Disorderetti sappeNo ratings yet
- OnychomycosisDocument19 pagesOnychomycosisRahul SrivastavaNo ratings yet
- February 2024 NewsletterDocument1 pageFebruary 2024 NewsletterJolaine ValloNo ratings yet
- (ANES) Fri Asynchronous Discussion - Basic Principles of Palliative Care and End of Life Care (Group 3) 10-23-2020Document12 pages(ANES) Fri Asynchronous Discussion - Basic Principles of Palliative Care and End of Life Care (Group 3) 10-23-2020Jolaine ValloNo ratings yet
- Effects of Music As An Adjunctive Therapy On Severity of Symptoms in Patients With Obsessive-Compulsive Disorder: Randomized Controlled TrialDocument15 pagesEffects of Music As An Adjunctive Therapy On Severity of Symptoms in Patients With Obsessive-Compulsive Disorder: Randomized Controlled TrialJolaine ValloNo ratings yet
- Preoperative Evaluation and PreparationDocument7 pagesPreoperative Evaluation and PreparationJolaine ValloNo ratings yet
- Effect of Internet-Based Vs Face-to-Face Cognitive Behavioral Therapy For Adults With Obsessive-Compulsive Disorder A Randomized Clinical TrialDocument15 pagesEffect of Internet-Based Vs Face-to-Face Cognitive Behavioral Therapy For Adults With Obsessive-Compulsive Disorder A Randomized Clinical TrialJolaine ValloNo ratings yet
- Structure-Function Correlation of Juxtapapillary Choroidal Thickness With Visual Field Analysis of Patients Suspected With GlaucomaDocument9 pagesStructure-Function Correlation of Juxtapapillary Choroidal Thickness With Visual Field Analysis of Patients Suspected With GlaucomaJolaine ValloNo ratings yet
- (ANES) Fri Asynchronous - Discussion - Principles of Palliative Care and End of Life CareDocument8 pages(ANES) Fri Asynchronous - Discussion - Principles of Palliative Care and End of Life CareJolaine ValloNo ratings yet
- CL Psychiatry Case Vignettes, 2022: July 1Document2 pagesCL Psychiatry Case Vignettes, 2022: July 1Jolaine ValloNo ratings yet
- (GYN) 05 Pelvic PainDocument5 pages(GYN) 05 Pelvic PainJolaine ValloNo ratings yet
- Student Guide Clerkship Revised AY2021-2022 Sept - OctDocument12 pagesStudent Guide Clerkship Revised AY2021-2022 Sept - OctJolaine ValloNo ratings yet
- (DERMA) 01 Introduction To Dermatology (History and PE)Document8 pages(DERMA) 01 Introduction To Dermatology (History and PE)Jolaine ValloNo ratings yet
- Med-Rheuma-Patient Write Up - Valeriano and ValloDocument10 pagesMed-Rheuma-Patient Write Up - Valeriano and ValloJolaine ValloNo ratings yet
- (DERMA) 03 TineasDocument9 pages(DERMA) 03 TineasJolaine ValloNo ratings yet
- Pgi To Do List: As of October 22, 2020 - Please Do Steps 1-3:)Document2 pagesPgi To Do List: As of October 22, 2020 - Please Do Steps 1-3:)Jolaine ValloNo ratings yet
- Advocacy Proposal - Group 3-3Document6 pagesAdvocacy Proposal - Group 3-3Jolaine ValloNo ratings yet
- Rheuma Prestests CompiledDocument13 pagesRheuma Prestests CompiledJolaine ValloNo ratings yet
- Data Management 'Birth Certificate'Document22 pagesData Management 'Birth Certificate'Jolaine Vallo100% (1)
- Data Management MCCODDocument48 pagesData Management MCCODJolaine ValloNo ratings yet
- (CLINPATH) Lipids and DyslipoproteinemiaDocument5 pages(CLINPATH) Lipids and DyslipoproteinemiaJolaine ValloNo ratings yet
- Treatments For COVID-19 - Harvard HealthDocument13 pagesTreatments For COVID-19 - Harvard HealthJolaine ValloNo ratings yet
- 12 Clin Path Exocrine and Endocrine Functions of The PancreasDocument13 pages12 Clin Path Exocrine and Endocrine Functions of The PancreasJolaine ValloNo ratings yet
- Gastroenterology Case Discussion: JANUARY 07, 2021 Dr. Stephen Wong Indigo and VioletDocument19 pagesGastroenterology Case Discussion: JANUARY 07, 2021 Dr. Stephen Wong Indigo and VioletJolaine ValloNo ratings yet
- (DERMA) Therapeutic Conference - Antifungal 07-07-20Document89 pages(DERMA) Therapeutic Conference - Antifungal 07-07-20Jolaine ValloNo ratings yet
- MPPRC Gi 2Document95 pagesMPPRC Gi 2Jolaine ValloNo ratings yet
- Derma Quiz 3 NotesDocument11 pagesDerma Quiz 3 NotesJolaine ValloNo ratings yet
- Derma Review HandoutDocument15 pagesDerma Review HandoutJolaine ValloNo ratings yet
- Course Orientation - Preventive Medicine 4 - AY 2021-2022 - SignedDocument24 pagesCourse Orientation - Preventive Medicine 4 - AY 2021-2022 - SignedJolaine ValloNo ratings yet
- Derma Quiz 2 NotesDocument9 pagesDerma Quiz 2 NotesJolaine ValloNo ratings yet
- UB HSPED Differential Diagnosis of Lower Back PainDocument62 pagesUB HSPED Differential Diagnosis of Lower Back PainJolaine ValloNo ratings yet
- Risk Factors of Urinary Tract Infection Caused by Extended SpectrumDocument5 pagesRisk Factors of Urinary Tract Infection Caused by Extended SpectrumPrimasari DiahNo ratings yet
- ICABST 2022 Conf - Program and Abstract BookDocument16 pagesICABST 2022 Conf - Program and Abstract BookDr.Vijayan Gurumurthy IyerNo ratings yet
- Pharmacotherapy: A Pathophysiologic Approach The Mcgraw-Hill CompaniesDocument83 pagesPharmacotherapy: A Pathophysiologic Approach The Mcgraw-Hill CompaniesLohith BasavarajuNo ratings yet
- NDDSDocument17 pagesNDDSsomesh chandraNo ratings yet
- 30 Nov 2016 131813263P8EW648MPreFeasibilityReportAVROrganics PDFDocument63 pages30 Nov 2016 131813263P8EW648MPreFeasibilityReportAVROrganics PDFgowthamNo ratings yet
- Atosiban-5ml InfusionDocument5 pagesAtosiban-5ml InfusionMd. Abdur RahmanNo ratings yet
- Pharmaceutical Latin. Abbreviations.: LibraryDocument12 pagesPharmaceutical Latin. Abbreviations.: LibraryTricia Antonette MillanesNo ratings yet
- An Update On Treatment Options For MethicillinResistant Staphylococcus Aureus (MRSA)Document9 pagesAn Update On Treatment Options For MethicillinResistant Staphylococcus Aureus (MRSA)Alex HernandezNo ratings yet
- MeclizineDocument2 pagesMeclizineGwyn Rosales100% (1)
- Pharmacotherapy of Anxiety Disorders: Current and Emerging Treatment OptionsDocument21 pagesPharmacotherapy of Anxiety Disorders: Current and Emerging Treatment OptionsGabriel Vargas CuadrosNo ratings yet
- Corticosteroids: Eva Dania Kosasih, M. Si., AptDocument17 pagesCorticosteroids: Eva Dania Kosasih, M. Si., AptTaufiq AnwariNo ratings yet
- Mercury Drug CorporationDocument11 pagesMercury Drug CorporationAj Lechugas50% (2)
- Drug Design and IsomarismDocument25 pagesDrug Design and IsomarismModern Institutes IndoreNo ratings yet
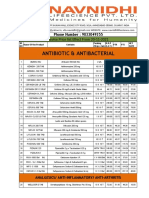
- Antibiotic & Antibacterial: Revise Price List Effect From 20-11-2021Document8 pagesAntibiotic & Antibacterial: Revise Price List Effect From 20-11-2021star internetNo ratings yet
- Novel Topical, Regional & Transdermal Dosage Forms Using Nanotechnology: A ReviewDocument9 pagesNovel Topical, Regional & Transdermal Dosage Forms Using Nanotechnology: A ReviewIJAR JOURNALNo ratings yet
- Anti-NMDA-receptor Encephalitis in An Adolescent With HIV Infection and Review of The LiteratureDocument3 pagesAnti-NMDA-receptor Encephalitis in An Adolescent With HIV Infection and Review of The LiteratureJeremy Eckhart S ParhusipNo ratings yet
- Critical Care MCQsDocument514 pagesCritical Care MCQsbgman83% (18)
- Lange Smart Charts: Pharmacology, 2e Pharmacologic SuffixesDocument2 pagesLange Smart Charts: Pharmacology, 2e Pharmacologic SuffixesSolNo ratings yet
- The Fundamentals of CTD & ECTDDocument45 pagesThe Fundamentals of CTD & ECTDRenuNo ratings yet
- Unit 9 - Drugs and Forensic ToxicologyDocument53 pagesUnit 9 - Drugs and Forensic ToxicologyNarciso Ana Jenecel100% (1)
- CBG Force Cannabinoids and Terpens v2Document1 pageCBG Force Cannabinoids and Terpens v2alejo ortiz szakielNo ratings yet
- Alkaloids 1Document4 pagesAlkaloids 1Mr nobodyNo ratings yet
- Antipsychotic Drugs: Referance Book .Essential of Pharmacology by Shah NawazDocument47 pagesAntipsychotic Drugs: Referance Book .Essential of Pharmacology by Shah NawazLaiba ShahNo ratings yet
- Contoh LASADocument1 pageContoh LASAninananaNo ratings yet
- Hyg 062Document5 pagesHyg 062verneck silvaNo ratings yet
- Protein Drug Binding: By: Kishan Arudra M.PharmDocument21 pagesProtein Drug Binding: By: Kishan Arudra M.PharmGianniNo ratings yet
- Wac 246-945Document90 pagesWac 246-945Christopher VũNo ratings yet
- Algorithm D: Pharmacological Treatment of Chronic Asthma in Children Under 5Document1 pageAlgorithm D: Pharmacological Treatment of Chronic Asthma in Children Under 5samNo ratings yet
- Disease of Pituitary GlandDocument25 pagesDisease of Pituitary GlandgibreilNo ratings yet
- Medication Card ClonazepamDocument2 pagesMedication Card ClonazepamTSPANNo ratings yet