You might also like
- Tlrhwesternpacific D 21 00438 ReviewerDocument19 pagesTlrhwesternpacific D 21 00438 ReviewerMinh Quang NguyenNo ratings yet
- Covid 19Document10 pagesCovid 19Adi Alphena100% (6)
- Evidence For Pre-Symptomatic Transmission of Coronavirus Disease 2019 (COVID-19) in ChinaDocument8 pagesEvidence For Pre-Symptomatic Transmission of Coronavirus Disease 2019 (COVID-19) in ChinaFatrina Maha DewiNo ratings yet
- The Effectiveness of The Quarantine of Wuhan City Against TheDocument25 pagesThe Effectiveness of The Quarantine of Wuhan City Against ThejameiNo ratings yet
- Estimating Unconfirmed COVID-19Document22 pagesEstimating Unconfirmed COVID-19mehdi lotfiNo ratings yet
- SSRN Id3525558Document20 pagesSSRN Id3525558Segundo PicoNo ratings yet
- Jiang2020 Article ReviewOfTheClinicalCharacteris PDFDocument5 pagesJiang2020 Article ReviewOfTheClinicalCharacteris PDFElena AlexandraNo ratings yet
- 1 s2.0 S1201971220301235 Main PDFDocument11 pages1 s2.0 S1201971220301235 Main PDFJoohhy DavïdNo ratings yet
- s41467-020-19802-w ReporteDocument7 pagess41467-020-19802-w ReporteJuan Carlos Martinez BorbonNo ratings yet
- Covid-19: A Perspective From ChinaDocument3 pagesCovid-19: A Perspective From ChinaEdgar Alfredo BERMEO VAN DEN BERGHENo ratings yet
- Review of The Clinical Characteristics of Coronavirus Disease 2019 (COVID-19)Document5 pagesReview of The Clinical Characteristics of Coronavirus Disease 2019 (COVID-19)Ahmed Abd El AzizNo ratings yet
- CoronaVirusOutbreak PDFDocument56 pagesCoronaVirusOutbreak PDFabcd100% (1)
- The Epidemiology and Pathogenesis of Coronavirus Disease Covid 19 Outbreak Hussin A Rothan Download 2024 Full ChapterDocument26 pagesThe Epidemiology and Pathogenesis of Coronavirus Disease Covid 19 Outbreak Hussin A Rothan Download 2024 Full Chapterbertha.harriman873100% (11)
- Mm6911e1 HDocument5 pagesMm6911e1 HShuvo H AhmedNo ratings yet
- Acop - Incubation Period of Covid-19Document7 pagesAcop - Incubation Period of Covid-19yorghiLNo ratings yet
- Aime202005050 m200504Document7 pagesAime202005050 m200504Ramsha RumaanNo ratings yet
- Dysregulation of Immune Response in Patients With Coronavirus 2019 (COVID-19) in Wuhan, ChinaDocument7 pagesDysregulation of Immune Response in Patients With Coronavirus 2019 (COVID-19) in Wuhan, Chinacika daraNo ratings yet
- Characteristics of COVID 19 Near China's EpidemicDocument5 pagesCharacteristics of COVID 19 Near China's EpidemicadaloraNo ratings yet
- Jiang Et Al-2020-Journal of General Internal Medicine1Document6 pagesJiang Et Al-2020-Journal of General Internal Medicine1Farida MurtianiNo ratings yet
- Articles: BackgroundDocument17 pagesArticles: BackgroundFereccella ZunettaNo ratings yet
- The Incubation Period of Coronavirus Disease 2019 (COVID-19) From Publicly Reported Confirmed Cases Estimation and ApplicationDocument7 pagesThe Incubation Period of Coronavirus Disease 2019 (COVID-19) From Publicly Reported Confirmed Cases Estimation and ApplicationIsrael Parra-OrtegaNo ratings yet
- A Comprehensive Literature Review On The Clinical Presentation, and Management of The Pandemic Coronavirus Disease 2019 (COVID-19)Document18 pagesA Comprehensive Literature Review On The Clinical Presentation, and Management of The Pandemic Coronavirus Disease 2019 (COVID-19)Zihan Zetira100% (1)
- Controlling The Transmission Dynamics of COVID-19Document13 pagesControlling The Transmission Dynamics of COVID-19Santos QuezadaNo ratings yet
- MainDocument7 pagesMainM ANo ratings yet
- Comment: The Lancet-And The Recently Documented Infections inDocument4 pagesComment: The Lancet-And The Recently Documented Infections inmbilotNo ratings yet
- Guidance for COVID-19: Prevention, Control, Diagnosis and ManagementFrom EverandGuidance for COVID-19: Prevention, Control, Diagnosis and ManagementNo ratings yet
- SARS To Novel Coronavirus - Old Lessons and New LessonsDocument4 pagesSARS To Novel Coronavirus - Old Lessons and New LessonsAlvaro SDNNo ratings yet
- 0 - 041 - Early PDFDocument7 pages0 - 041 - Early PDFsome buddyyNo ratings yet
- JMV 9999 NaDocument9 pagesJMV 9999 Nafk unswagatiNo ratings yet
- Controlling The Transmission Dynamics of COVID-19: March 2020Document14 pagesControlling The Transmission Dynamics of COVID-19: March 2020reqiqie reqeqeNo ratings yet
- Asia Covid EstrategiasDocument10 pagesAsia Covid EstrategiasJonell SanchezNo ratings yet
- Optimization Method For Forecasting Confirmed Cases of COVID-19 in ChinaDocument15 pagesOptimization Method For Forecasting Confirmed Cases of COVID-19 in Chinahectorfa1No ratings yet
- Nosocomial Infection of COVID 19: A New Challenge For Healthcare Professionals (Review)Document10 pagesNosocomial Infection of COVID 19: A New Challenge For Healthcare Professionals (Review)lagi magerNo ratings yet
- The Effect of Human Mobility and Control Measures On The COVID-19 Epidemic in ChinaDocument6 pagesThe Effect of Human Mobility and Control Measures On The COVID-19 Epidemic in ChinaJessica GomezNo ratings yet
- COVID-19 A Novel Zoonotic Disease Caused by A CoronavirusDocument6 pagesCOVID-19 A Novel Zoonotic Disease Caused by A CoronavirusAhmed Ismail SabriNo ratings yet
- The Rapid Assessment and Early Warning Models For COVID-19Document8 pagesThe Rapid Assessment and Early Warning Models For COVID-19Windu SyawalinaNo ratings yet
- Guide To Forensic Pathology Practice For Death Cases Related To Coronavirus Disease 2019 COVID 19 Trial DraftDocument8 pagesGuide To Forensic Pathology Practice For Death Cases Related To Coronavirus Disease 2019 COVID 19 Trial DraftDavid AlvarezNo ratings yet
- Guo-Li2021 Article ModelingAndDynamicAnalysisOfNoDocument26 pagesGuo-Li2021 Article ModelingAndDynamicAnalysisOfNoAmido MussaNo ratings yet
- A Mathematical Model For The Novel Coronavirus Epidemic in Wuhan, ChinaDocument17 pagesA Mathematical Model For The Novel Coronavirus Epidemic in Wuhan, ChinajrcubaNo ratings yet
- Jrnal COVID 123Document5 pagesJrnal COVID 123AzizaaNo ratings yet
- 3 PDFDocument9 pages3 PDFMORA CUEVAS NICOLE EDITHNo ratings yet
- Viral Infection and Transmission in A Large, Well-Traced Outbreak Caused by The Sars-Cov-2 Delta VariantDocument23 pagesViral Infection and Transmission in A Large, Well-Traced Outbreak Caused by The Sars-Cov-2 Delta VariantPatrick Leonard G. CoNo ratings yet
- Coronavirus Disease 2019 (COVID-19) A Perspective From ChinaDocument29 pagesCoronavirus Disease 2019 (COVID-19) A Perspective From ChinabackupNo ratings yet
- Piis0140673620301859 PDFDocument4 pagesPiis0140673620301859 PDFEnver Facundo Cruz GallegosNo ratings yet
- #126 - Zheng 2020Document13 pages#126 - Zheng 2020Adnan SaffiNo ratings yet
- 2020 Coronavirus Outbreak in Asia - Wikipedia PDFDocument25 pages2020 Coronavirus Outbreak in Asia - Wikipedia PDFChandrajeet ChavhanNo ratings yet
- Outbreak of A New Coronavirus What Anaesthetists Should KnowDocument5 pagesOutbreak of A New Coronavirus What Anaesthetists Should KnowSri NingsihNo ratings yet
- Microbes and Infection: Jin-Yan Li, Zhi You, Qiong Wang, Zhi-Jian Zhou, Ye Qiu, Rui Luo, Xing-Yi GeDocument6 pagesMicrobes and Infection: Jin-Yan Li, Zhi You, Qiong Wang, Zhi-Jian Zhou, Ye Qiu, Rui Luo, Xing-Yi GeLeah StroposNo ratings yet
- 2020 06 02 20120014v1 FullDocument15 pages2020 06 02 20120014v1 FullNATALIA BASTONo ratings yet
- Clinical Characteristics of Children With Coronavirus Disease 2019 in Hubei, ChinaDocument6 pagesClinical Characteristics of Children With Coronavirus Disease 2019 in Hubei, ChinaBobanBisercicNo ratings yet
- 1 s2.0 S0924857920301059 MainDocument13 pages1 s2.0 S0924857920301059 MainNini RinNo ratings yet
- Covid UpdateDocument29 pagesCovid UpdateAndreea PostolacheNo ratings yet
- The Novel Coronavirus Outbreak in Wuhan, China: Shortreport Open AccessDocument3 pagesThe Novel Coronavirus Outbreak in Wuhan, China: Shortreport Open AccessDelia AndreeaNo ratings yet
- Microbes and Infection: Xingchen Pan, David M. Ojcius, Tianyue Gao, Zhongsheng Li, Chunhua Pan, Chungen PanDocument6 pagesMicrobes and Infection: Xingchen Pan, David M. Ojcius, Tianyue Gao, Zhongsheng Li, Chunhua Pan, Chungen PanDavid Adolfo Paez MolinaNo ratings yet
- ARTIKELDocument6 pagesARTIKELandi susiloNo ratings yet
- 2020 Year End COVID UpdateDocument12 pages2020 Year End COVID UpdatehmounguiNo ratings yet
- Problem and Advice of Rural Poverty-Alleviation in China Amid The Epidemic of Covid-19Document11 pagesProblem and Advice of Rural Poverty-Alleviation in China Amid The Epidemic of Covid-19Mordecai NdlovuNo ratings yet
- Problem and Advice of Rural Poverty-Alleviation in China Amid The Epidemic of Covid-19 (Victor Mmbengwa and Xiaoshun Qin)Document11 pagesProblem and Advice of Rural Poverty-Alleviation in China Amid The Epidemic of Covid-19 (Victor Mmbengwa and Xiaoshun Qin)Mordecai NdlovuNo ratings yet
- Detailed Survey On Covid - 19: The VirusDocument19 pagesDetailed Survey On Covid - 19: The VirusAbbas KhanNo ratings yet
- Ciaa242 2 PDFDocument8 pagesCiaa242 2 PDFHesbon MomanyiNo ratings yet
- Construction of Compartmental Models For COVID-19 With Quarantine, Lockdown and Vaccine InterventionsDocument16 pagesConstruction of Compartmental Models For COVID-19 With Quarantine, Lockdown and Vaccine InterventionsMahmoudAboAlSamenNo ratings yet
- 6.2 More Times Than ReportedDocument12 pages6.2 More Times Than ReportedMahmoudAboAlSamenNo ratings yet
- Super Important - Seir and MobilityDocument19 pagesSuper Important - Seir and MobilityMahmoudAboAlSamenNo ratings yet
- Shinysir: Interactive Plotting For Infectious Disease ModelsDocument13 pagesShinysir: Interactive Plotting For Infectious Disease ModelsMahmoudAboAlSamenNo ratings yet
- Application of Deep Neural Networks As A PrescreenDocument10 pagesApplication of Deep Neural Networks As A PrescreenMahmoudAboAlSamenNo ratings yet
- Cameron Seir ModelDocument27 pagesCameron Seir ModelMahmoudAboAlSamenNo ratings yet
- Epidemic Modeling 102: All CoVID-19 Models Are Wrong, But Some Are Useful - by Bruno Gonçalves - Data For Science - MediumDocument24 pagesEpidemic Modeling 102: All CoVID-19 Models Are Wrong, But Some Are Useful - by Bruno Gonçalves - Data For Science - MediumMahmoudAboAlSamenNo ratings yet
- Substantial Undocumented Infection Facilitates The Rapid Dissemination of Novel Coronavirus (Sars-Cov-2)Document6 pagesSubstantial Undocumented Infection Facilitates The Rapid Dissemination of Novel Coronavirus (Sars-Cov-2)MahmoudAboAlSamenNo ratings yet
- EpiDynamics - SEIR Model DocumentationDocument41 pagesEpiDynamics - SEIR Model DocumentationMahmoudAboAlSamenNo ratings yet
- Measuring Excess MortalityDocument20 pagesMeasuring Excess MortalityMahmoudAboAlSamenNo ratings yet
- Estimating Number of TestsDocument8 pagesEstimating Number of TestsMahmoudAboAlSamenNo ratings yet
- The Politics of Return - Exploring The Future of Syrian Refugees in Jordan, Lebanon and TurkeyDocument20 pagesThe Politics of Return - Exploring The Future of Syrian Refugees in Jordan, Lebanon and TurkeyMahmoudAboAlSamenNo ratings yet
- Estimating Using Bayes RuleDocument9 pagesEstimating Using Bayes RuleMahmoudAboAlSamenNo ratings yet
- Livelihoods in ConflictDocument29 pagesLivelihoods in ConflictMahmoudAboAlSamenNo ratings yet
- Legal Status, Labelling, and Protection - The Case of Iraqi Refugees' in JordanDocument38 pagesLegal Status, Labelling, and Protection - The Case of Iraqi Refugees' in JordanMahmoudAboAlSamenNo ratings yet
- BrazilDocument6 pagesBrazilMahmoudAboAlSamenNo ratings yet
- 01 - Changrok Soh - Once Resolved Stay Resolved - The Refuge Policy of Jordan Toward Palestinian RefugeesDocument16 pages01 - Changrok Soh - Once Resolved Stay Resolved - The Refuge Policy of Jordan Toward Palestinian RefugeesMahmoudAboAlSamenNo ratings yet
- When Reciprocity FailsDocument9 pagesWhen Reciprocity FailsMahmoudAboAlSamenNo ratings yet
- Amman - City Migration ProfileDocument67 pagesAmman - City Migration ProfileMahmoudAboAlSamenNo ratings yet
- Stabilization of Amylase The Key Enzyme in Carbohydrates Properties Alterations at Low PHDocument16 pagesStabilization of Amylase The Key Enzyme in Carbohydrates Properties Alterations at Low PHMahmoudAboAlSamenNo ratings yet
- Effect of Refugee Integration On Migrant Labor in JordanDocument20 pagesEffect of Refugee Integration On Migrant Labor in JordanMahmoudAboAlSamenNo ratings yet
- ERI - PsychometricProperties PDFDocument28 pagesERI - PsychometricProperties PDFPaula CorreiaNo ratings yet
- Advantage of Teaching AidsDocument6 pagesAdvantage of Teaching AidsYousufNo ratings yet
- The Measurement of Effort-Reward Imbalance at Work: European ComparisonsDocument17 pagesThe Measurement of Effort-Reward Imbalance at Work: European ComparisonsMahmoudAboAlSamenNo ratings yet
- Diagnosis and Initial Management of Dysmenorrhea PDFDocument6 pagesDiagnosis and Initial Management of Dysmenorrhea PDFLam Sin WingNo ratings yet
- Research: Factors Predisposing Women To Chronic Pelvic Pain: Systematic ReviewDocument7 pagesResearch: Factors Predisposing Women To Chronic Pelvic Pain: Systematic ReviewMahmoudAboAlSamenNo ratings yet
- Informational Basis For Expert IntuitionDocument10 pagesInformational Basis For Expert IntuitionMahmoudAboAlSamenNo ratings yet
- Warning LabelsDocument18 pagesWarning LabelsMahmoudAboAlSamenNo ratings yet
- Developing Football Expertise A Football Specific Research ReviewDocument26 pagesDeveloping Football Expertise A Football Specific Research ReviewMahmoudAboAlSamenNo ratings yet
- Dialog 2 WWDocument4 pagesDialog 2 WWILHAM FERDIANSAHNo ratings yet
- QuestionsDocument47 pagesQuestionsCharizza Yvette100% (1)
- Tobacco Revelation ActDocument22 pagesTobacco Revelation ActSofie CatahanNo ratings yet
- The Indian History of Prenatal EducationDocument10 pagesThe Indian History of Prenatal Educationvaibhav gaikwadNo ratings yet
- k.4 B. Inggris Pak ArmanawiDocument8 pagesk.4 B. Inggris Pak ArmanawiUswatun HasanahNo ratings yet
- Donor Selections..Document17 pagesDonor Selections..OmamaNo ratings yet
- Medibuddy-EnrolPolicyConditions 22Document23 pagesMedibuddy-EnrolPolicyConditions 22Vadivelan BaskarNo ratings yet
- The Features and Benefits of Broiler Starter Feeds That Include Alphasoy™Document31 pagesThe Features and Benefits of Broiler Starter Feeds That Include Alphasoy™Matute SalmonNo ratings yet
- Test Metodu EN1276 PDFDocument13 pagesTest Metodu EN1276 PDFhcsoyleyiciNo ratings yet
- HIV Infection / AIDS (Z21, B20-B24)Document37 pagesHIV Infection / AIDS (Z21, B20-B24)Shreya ThackerNo ratings yet
- Vox Populix On Coronavirus PandemicDocument17 pagesVox Populix On Coronavirus PandemicayuNo ratings yet
- Powerpoint Presentation On Eating DisordersDocument52 pagesPowerpoint Presentation On Eating DisordersNirdesh MagarNo ratings yet
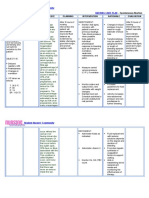
- Nursingcrib Com NURSING CARE PLAN Spontaneous AbortionDocument2 pagesNursingcrib Com NURSING CARE PLAN Spontaneous AbortionMina RacadioNo ratings yet
- JobDescriptionDocument17 pagesJobDescriptionAnonymous YqCxXQ6wF5No ratings yet
- Business Plan For Juan A Drink PDFDocument17 pagesBusiness Plan For Juan A Drink PDFMaria Jane MoyanoNo ratings yet
- Retirement Planning Mistakes Undermining The Post Retirement Adjustment and Well BeingDocument17 pagesRetirement Planning Mistakes Undermining The Post Retirement Adjustment and Well BeingMehedi HasanNo ratings yet
- Acp CBC 1Document52 pagesAcp CBC 1Danny R. SalvadorNo ratings yet
- Banking - Diksha Book On Effective Study Techniques PDFDocument66 pagesBanking - Diksha Book On Effective Study Techniques PDFHemrajSainiNo ratings yet
- Perioperative Nursing QuizDocument4 pagesPerioperative Nursing Quizgladz25100% (1)
- Employee Benefits Program by Etiqa Life Insurance BerhadDocument23 pagesEmployee Benefits Program by Etiqa Life Insurance BerhadNurain SarinaNo ratings yet
- Partograph EditedDocument54 pagesPartograph EditedNathaniel PulidoNo ratings yet
- Gorean Drugs & HerbsDocument3 pagesGorean Drugs & HerbsNishaNightFire100% (1)
- Lecture 1Document38 pagesLecture 1Yong Hao Jordan JinNo ratings yet
- Operator Edge 6 Wkphase 1 V2Document23 pagesOperator Edge 6 Wkphase 1 V2Luis Santamaría Álvarez-Gómez0% (1)
- DSEQ Manual 0 PDFDocument29 pagesDSEQ Manual 0 PDFRiki KikiNo ratings yet
- Form Pain DetectDocument2 pagesForm Pain Detectalvin100% (4)
- Moribund ICDSDocument114 pagesMoribund ICDSVikas SamvadNo ratings yet
- Confined Space RescueDocument490 pagesConfined Space RescueleeNo ratings yet
- Oxazepam (Serax)Document1 pageOxazepam (Serax)CassieNo ratings yet
- 11 ADHD Coping MechanismsDocument7 pages11 ADHD Coping Mechanismsamaandrei100% (11)