You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- TMR Facilitators 24.01.2018Document15 pagesTMR Facilitators 24.01.2018job.cndNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
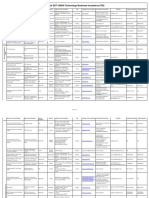
- List of DST-NIDHI Technology Business Incubators (TBI)Document11 pagesList of DST-NIDHI Technology Business Incubators (TBI)job.cndNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- United States O1 Visa Approval 1 728 AhmedDocument1 pageUnited States O1 Visa Approval 1 728 Ahmedjob.cndNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Sta Application UsDocument2 pagesSta Application Usjob.cndNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
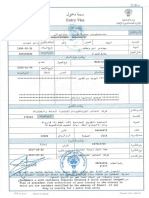
- Saudi VisaDocument1 pageSaudi Visajob.cndNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Personal Health Insurance Application FormDocument9 pagesPersonal Health Insurance Application Formjob.cndNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Ivermectin-The Global Scam1Document8 pagesIvermectin-The Global Scam1job.cndNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Application For United Kingdom Entry ClearanceDocument3 pagesApplication For United Kingdom Entry Clearancejob.cnd0% (1)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- List Insolvency ProfessionalDocument45 pagesList Insolvency ProfessionalSatyakam MishraNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Annual Report 2016-17 EnglishDocument76 pagesAnnual Report 2016-17 Englishjob.cndNo ratings yet
- Hard Hat, Safety Glasses, Gloves: Yemen DrillingDocument2 pagesHard Hat, Safety Glasses, Gloves: Yemen DrillingkhurramNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Opening Movement 1 - Holding Barrels - Proofread LN 2021-07-12Document3 pagesOpening Movement 1 - Holding Barrels - Proofread LN 2021-07-12api-268467409No ratings yet
- Quiz 1Document2 pagesQuiz 1tasfin mahmudNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- PANAMA CANAL AUTHORITY ACP Maritime OperDocument70 pagesPANAMA CANAL AUTHORITY ACP Maritime Operagus nurcahyoNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shell Helix HX5 15W 40 TDS PDFDocument2 pagesShell Helix HX5 15W 40 TDS PDFhoussem houssemNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
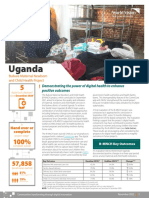
- 2021 Digital Health Factsheet - B-MNCH - UgandaDocument2 pages2021 Digital Health Factsheet - B-MNCH - UgandaMd UmerNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Reviewer in P.E. 11Document25 pagesReviewer in P.E. 11Joel BrionesNo ratings yet
- CH 1812Document58 pagesCH 1812mjaved986142No ratings yet
- Moon Dialoguing With Dreams in Existential Art TherapyDocument6 pagesMoon Dialoguing With Dreams in Existential Art TherapyAnonymous oAGumZoNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Durability of Porcelain VeneersDocument6 pagesDurability of Porcelain VeneersGeorge GeoNo ratings yet
- Makassar 1: Total Target OptimisDocument2 pagesMakassar 1: Total Target OptimisAchaElmanNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- 1-Janparticle 2 PDFDocument13 pages1-Janparticle 2 PDFMusunuri Ratna TejaNo ratings yet
- How To Do Dhanurasana (Bow Pose)Document2 pagesHow To Do Dhanurasana (Bow Pose)MIBNo ratings yet
- Meta Analysis Offers Research On Research For MR ArticlesDocument9 pagesMeta Analysis Offers Research On Research For MR ArticlesSahil Vyas100% (1)
- Contoh Judul Jurnal Kesehatan InternasionalDocument3 pagesContoh Judul Jurnal Kesehatan Internasionalnadya100% (1)
- Muscles Developing Properties of Gamma Oryzanol - ResearchDocument1 pageMuscles Developing Properties of Gamma Oryzanol - ResearchRAJESH ANNAMALAI ALNo ratings yet
- Surrogate Parenting AgreementDocument10 pagesSurrogate Parenting Agreementsujith suryaNo ratings yet
- Contoh Review GarciniaDocument8 pagesContoh Review GarciniamarwahNo ratings yet
- Scandinavian Med Sci Sports - 2023 - Nuzzo - Overview of Muscle Fatigue Differences Between Maximal Eccentric andDocument15 pagesScandinavian Med Sci Sports - 2023 - Nuzzo - Overview of Muscle Fatigue Differences Between Maximal Eccentric andcsrpirataNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Life Science Health System T C FryDocument2,295 pagesThe Life Science Health System T C FryAna Debeljuh100% (1)
- Application Form - FMU (New Form BUPA)Document16 pagesApplication Form - FMU (New Form BUPA)gabinicolescu9999No ratings yet
- ASD Atrial Septal Defect PDFDocument9 pagesASD Atrial Septal Defect PDFAco AjjahNo ratings yet
- Mil PRF 680CDocument12 pagesMil PRF 680CfltpNo ratings yet
- Jade Stem Exercises - Gift PDFDocument16 pagesJade Stem Exercises - Gift PDFHéctorMartínezSalazarNo ratings yet
- Crew Size Simulation Cardiac Arrest TapiaiDocument12 pagesCrew Size Simulation Cardiac Arrest TapiaiJamison ParfittNo ratings yet
- Haug1992 PDFDocument4 pagesHaug1992 PDFpalliNo ratings yet
- Department of Education Schools Division of Toledo City Malubog Elementary SchoolDocument6 pagesDepartment of Education Schools Division of Toledo City Malubog Elementary SchoolTintin Cadorna FielNo ratings yet
- Inventaris Alkes BaruDocument49 pagesInventaris Alkes Barulyna timothyNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Daftar Produk Sisipan 2 Formularium Edisi XiiDocument4 pagesDaftar Produk Sisipan 2 Formularium Edisi XiikobusNo ratings yet
- Ayurpharm 393Document6 pagesAyurpharm 393Rahul KirkNo ratings yet