You might also like
- EKG/ECG Study GuideDocument13 pagesEKG/ECG Study GuideSherree HayesNo ratings yet
- Internal Medicine TNDocument3 pagesInternal Medicine TNZeeshan Ahmed100% (2)
- Pediatric NotesDocument45 pagesPediatric NoteskkkssbbNo ratings yet
- Anesthesia PocketDocument10 pagesAnesthesia Pocketnebrasothman977No ratings yet
- Transurethral Resection of The Prostate Anesthetic Considerations Dr. Frank TitzeDocument25 pagesTransurethral Resection of The Prostate Anesthetic Considerations Dr. Frank TitzeFityan Aulia RahmanNo ratings yet
- Acute Renal FailureDocument5 pagesAcute Renal FailureSalman KhanNo ratings yet
- Oxford Learner's Pocket Phrasal Verbs and Idioms (Scanned File, Deskewed Pages)Document287 pagesOxford Learner's Pocket Phrasal Verbs and Idioms (Scanned File, Deskewed Pages)Rob P100% (14)
- Ravi Kannaiyan: QC Inspection EngineerDocument5 pagesRavi Kannaiyan: QC Inspection EngineerVinoth BalaNo ratings yet
- Experience Human Development 13th Edition Papalia Test Bank 1Document150 pagesExperience Human Development 13th Edition Papalia Test Bank 1matthew100% (39)
- Renal Emergency RevisiDocument103 pagesRenal Emergency Revisidesy f sarahNo ratings yet
- Diabetic Ketoacidosis PathwayDocument22 pagesDiabetic Ketoacidosis PathwaySri Nath100% (1)
- Endocrine Emergencies CompiledDocument102 pagesEndocrine Emergencies CompiledSubhkanish RavindraNo ratings yet
- Use Hygienic Practices For Food SafetyDocument60 pagesUse Hygienic Practices For Food Safetyapi-505030460No ratings yet
- Exchange TransfusionDocument35 pagesExchange Transfusionsobinjohnpkl100% (2)
- Hyperkalaemia: See Also BackgroundDocument6 pagesHyperkalaemia: See Also BackgroundamaliaNo ratings yet
- Turp 160328193838Document36 pagesTurp 160328193838Right VentricleNo ratings yet
- Hipertensi Portal Donny SandraDocument67 pagesHipertensi Portal Donny SandrabobyNo ratings yet
- Case Report Uterine InversionDocument64 pagesCase Report Uterine InversionFelicia Yumita Winata100% (1)
- Potassium DisturbancesDocument23 pagesPotassium DisturbancesThien Nhan MaiNo ratings yet
- Acute Kidney Injury and Chronic Kidney DiseaseDocument44 pagesAcute Kidney Injury and Chronic Kidney DiseaseIda Bagus Putu Swabawa100% (1)
- Mojahid Sheet Complete PDFDocument176 pagesMojahid Sheet Complete PDFOsman SomiNo ratings yet
- Body FluidDocument37 pagesBody FluidBir Mohammad SonetNo ratings yet
- Fever: DengueDocument95 pagesFever: DengueAnonymous RNMJmeu8tNo ratings yet
- Chronic Liver Disease Decompensated N PDFDocument6 pagesChronic Liver Disease Decompensated N PDFmzhao230No ratings yet
- Mojahid Sheet CompleteDocument176 pagesMojahid Sheet CompleteAdams AdamNo ratings yet
- مجاهد PDFDocument176 pagesمجاهد PDFHalema Al OkshNo ratings yet
- Post Partum Haemorrhage (PPH)Document33 pagesPost Partum Haemorrhage (PPH)Khan WasimNo ratings yet
- Hyperkalaemia FormularyDocument3 pagesHyperkalaemia FormularyMiguel SanJuanNo ratings yet
- Comer Emergency Department (ED) Clinical Guidelines: Diabetic Ketoacidosis (DKA) - Moderately Severe To SevereDocument6 pagesComer Emergency Department (ED) Clinical Guidelines: Diabetic Ketoacidosis (DKA) - Moderately Severe To SevereChristelle Malaluan CalumpitNo ratings yet
- Jurnal Laporan 3Document6 pagesJurnal Laporan 3Rutnita NainggolanNo ratings yet
- Angela Heithaus, MD, PS Internal Medicine Seattle Healing Arts CenterDocument32 pagesAngela Heithaus, MD, PS Internal Medicine Seattle Healing Arts CenterMarwan M.No ratings yet
- Acute Metabolic Complications of Diabetes MellitusDocument54 pagesAcute Metabolic Complications of Diabetes MellitusPrincewill SeiyefaNo ratings yet
- Based On Your Possible Final Diagnosis, What Are The Treatment Plans For Our Patient?Document63 pagesBased On Your Possible Final Diagnosis, What Are The Treatment Plans For Our Patient?Kita kitaNo ratings yet
- Surgery Class Biliary System SurgeryDocument69 pagesSurgery Class Biliary System SurgeryKashif BurkiNo ratings yet
- Peritonitis in PD PatientsDocument64 pagesPeritonitis in PD PatientsDaniel SitungkirNo ratings yet
- Revised DKA 2015 PDFDocument6 pagesRevised DKA 2015 PDFDr AhmedNo ratings yet
- Akd & CKDDocument44 pagesAkd & CKDﻣﻠﻚ عيسىNo ratings yet
- Cross Cover Survival Guide: Electrolyte ReplacementDocument5 pagesCross Cover Survival Guide: Electrolyte Replacementjrbull88No ratings yet
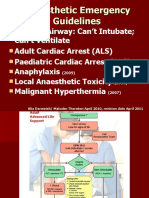
- Emergency GuidelinesDocument11 pagesEmergency GuidelineswinstonappsNo ratings yet
- Fluid Student 2012Document43 pagesFluid Student 2012Sara Ilyas KhanNo ratings yet
- Diabetic Ketoacidosis (DKA) : Myocardial InfarctionDocument5 pagesDiabetic Ketoacidosis (DKA) : Myocardial InfarctionManju PillaiNo ratings yet
- Slemani Pediatric Teaching Hospital GuidelinesDocument93 pagesSlemani Pediatric Teaching Hospital GuidelinesHeersh RaofNo ratings yet
- Diabetes KetoacidosisDocument23 pagesDiabetes KetoacidosisSalman MajidNo ratings yet
- Anaesthesia For Urologic Surgery: (Peer Reviewed) (1987), 15,203-211Document12 pagesAnaesthesia For Urologic Surgery: (Peer Reviewed) (1987), 15,203-211ramzi MohamedNo ratings yet
- AscitesDocument71 pagesAscitessohilaw210No ratings yet
- Skin Nylon 6/0 Nylon 3/0 Nylon 5/0 Face Back, Scalp Elsewhere Deeper Tissue (Dead Space) Catgut 4/0 Dexon/Vicryl 3/0 or 4/0 Face ElsewhereDocument8 pagesSkin Nylon 6/0 Nylon 3/0 Nylon 5/0 Face Back, Scalp Elsewhere Deeper Tissue (Dead Space) Catgut 4/0 Dexon/Vicryl 3/0 or 4/0 Face Elsewheredr.gauravsuneja7125No ratings yet
- B4Y5G1 O - G - With AnswersDocument4 pagesB4Y5G1 O - G - With AnswersZeke EdgeNo ratings yet
- Case Report: Non St-Elevated Myocardial Infarction (Nstemi)Document40 pagesCase Report: Non St-Elevated Myocardial Infarction (Nstemi)NissaIsfadinaSNo ratings yet
- Git BleedingDocument28 pagesGit Bleedingsembakarani thevagumaranNo ratings yet
- MGT of D KetoacidosisDocument5 pagesMGT of D Ketoacidosisshabatat2002No ratings yet
- Ascitic TapDocument20 pagesAscitic TapLaraib KanwalNo ratings yet
- سموم عملي٣Document16 pagesسموم عملي٣مصطفى ابراهيم سعيد100% (1)
- Gastrointestinal HaemorrhageDocument58 pagesGastrointestinal HaemorrhageAhmed ElwassiefNo ratings yet
- Diabetic Ketoacidosis (DKA) : BackgroundDocument7 pagesDiabetic Ketoacidosis (DKA) : BackgroundLeoNo ratings yet
- Management of Potassium Disorders 17706 ArticleDocument4 pagesManagement of Potassium Disorders 17706 ArticlealeNo ratings yet
- 23 Anaesthesia For Emergency SurgeryDocument7 pages23 Anaesthesia For Emergency SurgeryAtuy NapsterNo ratings yet
- Diabetic Ketoacidosis: Medical EmergencyDocument18 pagesDiabetic Ketoacidosis: Medical EmergencyKirsten Padilla ChuaNo ratings yet
- ATOTW 136 Major Haemorrhage Part 1 2009Document6 pagesATOTW 136 Major Haemorrhage Part 1 2009viaereaNo ratings yet
- Management of PPHDocument24 pagesManagement of PPHMutabazi SharifNo ratings yet
- DKAPPTxDocument34 pagesDKAPPTxMuhammad FurqanNo ratings yet
- Clinical Pathophys NitesDocument28 pagesClinical Pathophys NitesDemianaNo ratings yet
- Paediatric Clinical GuidelinesDocument7 pagesPaediatric Clinical GuidelinesAndriNo ratings yet
- Presentation 5 - DR Rao BondugulapatiDocument44 pagesPresentation 5 - DR Rao Bondugulapatiশরীফ উল কবীরNo ratings yet
- Management of Post Partum Haemorrhage 2017Document30 pagesManagement of Post Partum Haemorrhage 2017Muhamad IrsyadNo ratings yet
- Terms Definitions and Routes of IV TherapyDocument13 pagesTerms Definitions and Routes of IV TherapyRob PNo ratings yet
- J Vet Emergen Crit Care - 2002 - Mazzaferro - The Role of Albumin Replacement in The Critically Ill Veterinary PatientDocument12 pagesJ Vet Emergen Crit Care - 2002 - Mazzaferro - The Role of Albumin Replacement in The Critically Ill Veterinary PatientRob PNo ratings yet
- Brown C (2013) Patient Care Report For Feline Patient With Urethral ObstructionDocument5 pagesBrown C (2013) Patient Care Report For Feline Patient With Urethral ObstructionRob PNo ratings yet
- Transforming Cancer CareDocument33 pagesTransforming Cancer CareAKASH SHRIVASTAVANo ratings yet
- Basic Training: Elementary First Aid: Written AssessmentDocument2 pagesBasic Training: Elementary First Aid: Written AssessmentClark LlameraNo ratings yet
- Hospital Managment Unit 3Document62 pagesHospital Managment Unit 3seemantham123No ratings yet
- Normal Value For Urine TestDocument2 pagesNormal Value For Urine TestMarcellino NernereNo ratings yet
- Harga KhususDocument16 pagesHarga KhususNoperitaNo ratings yet
- Operating RoomDocument13 pagesOperating RoomrichardNo ratings yet
- ACG Clinical Guideline Diagnosis Treatment and Prevention of Acute Diarrheal Infections in AdultsDocument14 pagesACG Clinical Guideline Diagnosis Treatment and Prevention of Acute Diarrheal Infections in AdultsMara Medina - BorleoNo ratings yet
- Cardiopulmonary Resuscitation (CPR) : Akper BookDocument4 pagesCardiopulmonary Resuscitation (CPR) : Akper BookFitriana Noor SabrinaNo ratings yet
- Tatalaksana Oftalmia Neonatorum Ec Infeksi Gonokokal Dengan Ikterik Neonatorum - Viora Rianda PiscalokaDocument12 pagesTatalaksana Oftalmia Neonatorum Ec Infeksi Gonokokal Dengan Ikterik Neonatorum - Viora Rianda Piscalokasupaidi97No ratings yet
- D HC OperatorsDocument5,396 pagesD HC OperatorsCoupon VampireNo ratings yet
- NICU PPT Hypo and HyperthermiaDocument23 pagesNICU PPT Hypo and HyperthermiaelsawzgoodNo ratings yet
- CMR 00062-17Document78 pagesCMR 00062-17pokhara144No ratings yet
- PicoPlus Sell Sheet FINAL SMDocument2 pagesPicoPlus Sell Sheet FINAL SMJLNo ratings yet
- Cephalosporin UnitDocument11 pagesCephalosporin Unitviper1402No ratings yet
- Pub - Principles and Practice of NeuropathologyDocument608 pagesPub - Principles and Practice of NeuropathologyArkham AsylumNo ratings yet
- Ca1 PrelimDocument60 pagesCa1 PrelimAira EspleguiraNo ratings yet
- Administering Intradermal InjectionDocument17 pagesAdministering Intradermal InjectionPattNo ratings yet
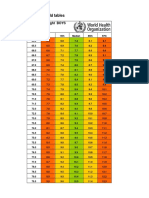
- Girls Simplified Field Tables Weight For Length Birth To 2 Years (Percentiles)Document5 pagesGirls Simplified Field Tables Weight For Length Birth To 2 Years (Percentiles)Gabrielly LopesNo ratings yet
- From One Prick To AnotherDocument528 pagesFrom One Prick To AnotherSkyla ReadNo ratings yet
- Unknown 79 Mycology University of Adelaide PDFDocument1 pageUnknown 79 Mycology University of Adelaide PDFLinda Gonzalez (Maddy)No ratings yet
- 02 - Establishing Background Levels - EPA - 1995Document7 pages02 - Establishing Background Levels - EPA - 1995JessikaNo ratings yet
- 2023 NGN Ati RN Fundamentals Proctored Exam (Version 1, 2, 3, 4, 5,) With NGN Questions and Verified Answers & RationalesDocument4 pages2023 NGN Ati RN Fundamentals Proctored Exam (Version 1, 2, 3, 4, 5,) With NGN Questions and Verified Answers & Rationalesmarcuskenyatta275No ratings yet
- Planned Parenthood Maryland 2020Document12 pagesPlanned Parenthood Maryland 2020Kate AndersonNo ratings yet
- D2 0905 Paediatric Reference Intervals - An Update - Tina YenDocument25 pagesD2 0905 Paediatric Reference Intervals - An Update - Tina YenkamalNo ratings yet
- JUSHI Safety Data SheetDocument11 pagesJUSHI Safety Data SheetSofya AndarinaNo ratings yet
- Boys Simplified Field Tables Weight For Length 2 To 5 Years (Percentiles)Document4 pagesBoys Simplified Field Tables Weight For Length 2 To 5 Years (Percentiles)Gabrielly LopesNo ratings yet