You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- BPC-157 A Collection of StudiesDocument28 pagesBPC-157 A Collection of StudiesscribdNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- PSYCH 1.1A Schizophrenia Spectrum and Other Psychotic DisorderDocument28 pagesPSYCH 1.1A Schizophrenia Spectrum and Other Psychotic DisorderZaza100% (1)
- Z Score Girls PDFDocument15 pagesZ Score Girls PDFDio Pratama0% (1)
- HEALTH 7 EXAM (2nd Quarter) QuestionsDocument4 pagesHEALTH 7 EXAM (2nd Quarter) QuestionsKert Cyrel RomeroNo ratings yet
- Guide to Salivary Gland NeoplasmsDocument28 pagesGuide to Salivary Gland Neoplasmsrameshparajuli14100% (1)
- CopdDocument60 pagesCopdRizqy Shofianingrum100% (1)
- Test 1 Science Form 3Document7 pagesTest 1 Science Form 3Zunaizah Yahaya100% (1)
- Pediatric DehydrationDocument4 pagesPediatric DehydrationFortune De AmorNo ratings yet
- Medical Health Care PowerPoint TemplatesDocument48 pagesMedical Health Care PowerPoint TemplatesAl-UmamNo ratings yet
- DehydrationDocument1 pageDehydrationFortune De AmorNo ratings yet
- Pemicu 1 GI AmorDocument93 pagesPemicu 1 GI AmorFortune De AmorNo ratings yet
- Pemicu 1 GI AmorDocument93 pagesPemicu 1 GI AmorFortune De AmorNo ratings yet
- Blok Kegawatdaruratan 4Document66 pagesBlok Kegawatdaruratan 4Fortune De AmorNo ratings yet
- Pemicu 5 GIDocument98 pagesPemicu 5 GIFortune De AmorNo ratings yet
- Pemicu 4 GIDocument121 pagesPemicu 4 GIFortune De AmorNo ratings yet
- Kegawatdaruratan 3Document49 pagesKegawatdaruratan 3Fortune De AmorNo ratings yet
- Blok Kegawatdaruratan 1Document71 pagesBlok Kegawatdaruratan 1Fortune De AmorNo ratings yet
- Blok Kegawatdaruratan 2Document42 pagesBlok Kegawatdaruratan 2Fortune De AmorNo ratings yet
- Examining The PrecordiumDocument83 pagesExamining The PrecordiumnicolNo ratings yet
- Liu036 Brain Disorders PDFDocument2 pagesLiu036 Brain Disorders PDFAyeshaNo ratings yet
- Calawag National High School MAPEH AssessmentDocument2 pagesCalawag National High School MAPEH AssessmentMarbert GarganzaNo ratings yet
- ECG Rhythm InterpretationDocument21 pagesECG Rhythm Interpretationvanstar7100% (1)
- Clinical - Liver: Simple Noninvasive Systems Predict Long-Term Outcomes of Patients With Nonalcoholic Fatty Liver DiseaseDocument12 pagesClinical - Liver: Simple Noninvasive Systems Predict Long-Term Outcomes of Patients With Nonalcoholic Fatty Liver Disease走过一些路No ratings yet
- Eye - Blur Vision Part IIDocument56 pagesEye - Blur Vision Part IIStaporn Kasemsripitak100% (2)
- Pill CameraDocument21 pagesPill CameraAnil DsouzaNo ratings yet
- Opening: (EN-ES-EI-AI-DI) (EN-ES-EI-AI-DI)Document4 pagesOpening: (EN-ES-EI-AI-DI) (EN-ES-EI-AI-DI)Trisna meyanaNo ratings yet
- Liposomal Doxorubicin ExtravasationDocument2 pagesLiposomal Doxorubicin ExtravasationjathieNo ratings yet
- Dr. Niroopama Pushpagiri: RSR Sarada Maternity Hospital, Pogathota, NelloreDocument51 pagesDr. Niroopama Pushpagiri: RSR Sarada Maternity Hospital, Pogathota, Nelloresushmanth reddy katamreddyNo ratings yet
- Urology Case Reports: Aideen Madden, Asadullah Aslam, Nadeem B. NusratDocument3 pagesUrology Case Reports: Aideen Madden, Asadullah Aslam, Nadeem B. NusratsoufiearyaniNo ratings yet
- Diagnosis: ChildrenDocument2 pagesDiagnosis: ChildrencsomimagesNo ratings yet
- Chart of Eye SymptomsDocument1 pageChart of Eye SymptomsRaghunandan RamanathanNo ratings yet
- A Diagnostic Dilemma in A Child With Macroscopic Hematuria, Nephrotic Syndrome and Hypocomplementemia: AnswersDocument4 pagesA Diagnostic Dilemma in A Child With Macroscopic Hematuria, Nephrotic Syndrome and Hypocomplementemia: AnswersRiszki_03No ratings yet
- Drug index for Risperdal, Diumide, Amlodipine, Linagliptin and other medicationsDocument103 pagesDrug index for Risperdal, Diumide, Amlodipine, Linagliptin and other medicationsvalencia222No ratings yet
- Top 5 Acupressure Points To Treat Cold, Flu and FeverDocument16 pagesTop 5 Acupressure Points To Treat Cold, Flu and Feverdlpurpos0% (1)
- Investigation of Outbreak 2Document54 pagesInvestigation of Outbreak 2Evan Permana PutraNo ratings yet
- Rodaks Chapter Quizzes Chapter 35 43Document8 pagesRodaks Chapter Quizzes Chapter 35 43Maria MikaelaNo ratings yet
- Congenital Scoliosis Case Study: Ashley (6-7 YearsDocument20 pagesCongenital Scoliosis Case Study: Ashley (6-7 YearsIulia Dulgheru100% (1)
- MicroorganismsDocument12 pagesMicroorganismsMiggy GNo ratings yet
- DNB Radio Diagnosis Paper1Document4 pagesDNB Radio Diagnosis Paper1Taha IsmailNo ratings yet
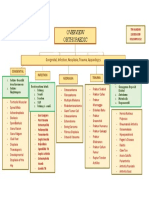
- Orthopaedic: Congenital, Infection, Neoplasia, Trauma, AppandegesDocument1 pageOrthopaedic: Congenital, Infection, Neoplasia, Trauma, AppandegesdinsNo ratings yet
- Case 1: Group 4Document26 pagesCase 1: Group 4John Joshua Lacson MedicineNo ratings yet