You might also like
- 1 s2.0 S2173511517301550 MainDocument6 pages1 s2.0 S2173511517301550 MainHermenegildo chitumbaNo ratings yet
- Out-of-Pocket Costs For Patients Diagnosed With Tuberculosis in Different Healthcare Settings in Bandung, IndonesiaDocument8 pagesOut-of-Pocket Costs For Patients Diagnosed With Tuberculosis in Different Healthcare Settings in Bandung, Indonesiagshalimar shalNo ratings yet
- Adiutarini 6Document12 pagesAdiutarini 6Eva Tirtabayu HasriNo ratings yet
- Private Practitioners and Tuberculosis Case Detection in Jogjakarta, Indonesia: Actual Role and PotentialDocument7 pagesPrivate Practitioners and Tuberculosis Case Detection in Jogjakarta, Indonesia: Actual Role and PotentialEva Tirtabayu HasriNo ratings yet
- Arentz Et AlDocument8 pagesArentz Et Alkang.asep008No ratings yet
- 2209-4526-1-SM (1)Document1 page2209-4526-1-SM (1)baloziandersonNo ratings yet
- Chen 2017Document7 pagesChen 2017Miranti Dea DoraNo ratings yet
- Evaluation Factors Contributing To The Treatment Default by Tuberculosis Patients at ART Clinic in Ishaka Adventist Hospital, Bushenyi District, Uganda.Document15 pagesEvaluation Factors Contributing To The Treatment Default by Tuberculosis Patients at ART Clinic in Ishaka Adventist Hospital, Bushenyi District, Uganda.KIU PUBLICATION AND EXTENSIONNo ratings yet
- A Kap Study of Hepatitis Among Hepatitis Positive Patients Presenting To A Tertiary Care Hospital in Southern Punjab, PakistanDocument4 pagesA Kap Study of Hepatitis Among Hepatitis Positive Patients Presenting To A Tertiary Care Hospital in Southern Punjab, Pakistanارسلان علیNo ratings yet
- Adherence To Medication Behavior Among TuberculosiDocument7 pagesAdherence To Medication Behavior Among TuberculosiPPI RSUI MBNo ratings yet
- A Prospective Interventional Study of Knowledge, Attitude and Practice (Kap) Towards Tuberculosis Among Patients With Koch'S DiseaseDocument4 pagesA Prospective Interventional Study of Knowledge, Attitude and Practice (Kap) Towards Tuberculosis Among Patients With Koch'S DiseaseButton WoodcraftNo ratings yet
- Knowledge, Attitudes, and Practices Among Physicians On HIV/AIDS in Quang Ninh, VietnamDocument13 pagesKnowledge, Attitudes, and Practices Among Physicians On HIV/AIDS in Quang Ninh, VietnamAli143MarymNo ratings yet
- Le Couturier 1999Document9 pagesLe Couturier 1999NYONGKERNo ratings yet
- Zimbabwe's Hospital Referral System: Does It Work? Zimbabwe's Hospital Referral System: Does It Work?Document12 pagesZimbabwe's Hospital Referral System: Does It Work? Zimbabwe's Hospital Referral System: Does It Work?Hiten DabhiNo ratings yet
- PD Reference Article 1Document4 pagesPD Reference Article 1Azmul HussainNo ratings yet
- Treatment Seeking Behavior and Factors Associated With Its Delay Among Newly Diagnosed Pulmonary Tuberculosis Patients in Bhopal, Madhya PradeshDocument6 pagesTreatment Seeking Behavior and Factors Associated With Its Delay Among Newly Diagnosed Pulmonary Tuberculosis Patients in Bhopal, Madhya PradeshAdvanced Research PublicationsNo ratings yet
- Karapet DavtyanDocument8 pagesKarapet Davtyanyenni elfiraNo ratings yet
- Analisis+Konkordansi+Perilaku+Pengobatan Arlinda Fkusu 12007Document9 pagesAnalisis+Konkordansi+Perilaku+Pengobatan Arlinda Fkusu 12007Muhammad Mahadi HasibuanNo ratings yet
- Factors Impacting Tuberculosis Treatment Adherence in Rural TurkeyDocument7 pagesFactors Impacting Tuberculosis Treatment Adherence in Rural TurkeyAnonymous QPXAgjBwNo ratings yet
- (Pro) Ing 1, Ada Kuesioner Juga12Document8 pages(Pro) Ing 1, Ada Kuesioner Juga12ilhamNo ratings yet
- SSMJ 7 2 TB Kap StudyDocument5 pagesSSMJ 7 2 TB Kap StudyUmer FarooqNo ratings yet
- Jurnal TBC Inter 1Document5 pagesJurnal TBC Inter 1sekti lindaNo ratings yet
- Occupational Exposure and Tuberculosis Among Medical Residents in A High-Burden Setting: An Open-Cohort StudyDocument14 pagesOccupational Exposure and Tuberculosis Among Medical Residents in A High-Burden Setting: An Open-Cohort StudyWisnu Syahputra SuryanullahNo ratings yet
- Factors Affecting Adherence To Antiretroviral Therapy Among HIV Positive Adults Living in Bison Slums in Tororo Municipality, Tororo District, Eastern UgandaDocument11 pagesFactors Affecting Adherence To Antiretroviral Therapy Among HIV Positive Adults Living in Bison Slums in Tororo Municipality, Tororo District, Eastern UgandaKIU PUBLICATION AND EXTENSIONNo ratings yet
- World of Pediatric Surgery 1Document8 pagesWorld of Pediatric Surgery 1VanessaGGSNo ratings yet
- Early Detection of Tuberculosis Through Community-Based Active Case Finding in CambodiaDocument11 pagesEarly Detection of Tuberculosis Through Community-Based Active Case Finding in CambodiaPatriciann13No ratings yet
- Abstract 59Document3 pagesAbstract 59Jarvis WheelerNo ratings yet
- Hemodialysis and Peritoneal Dialysis - Patients' Assessment of Their Satisfaction With Therapy and The Impact of The Therapy On Their LivesDocument6 pagesHemodialysis and Peritoneal Dialysis - Patients' Assessment of Their Satisfaction With Therapy and The Impact of The Therapy On Their Livesmaria teresa pertuz rondonNo ratings yet
- Articulo 1Document5 pagesArticulo 1lucia acasieteNo ratings yet
- Haber 2017Document8 pagesHaber 2017Gisela M SilvaNo ratings yet
- InIntegrating Traditional Healers in The Treatment of Tbtegrating Traditional Healers in The Treatment of TBDocument2 pagesInIntegrating Traditional Healers in The Treatment of Tbtegrating Traditional Healers in The Treatment of TBGerald SackNo ratings yet
- Awareness of Medical Orders For Life Sustaining Treatmen - 2016 - Journal of PaiDocument1 pageAwareness of Medical Orders For Life Sustaining Treatmen - 2016 - Journal of PaiDipendra PratapNo ratings yet
- Wales 2004Document6 pagesWales 2004Subha ManivannanNo ratings yet
- Diagnostic Delay Amongst Tuberculosis Patients in Jogjakarta Province, Indonesia Is Related To The Quality of Services in DOTS FacilitiesDocument13 pagesDiagnostic Delay Amongst Tuberculosis Patients in Jogjakarta Province, Indonesia Is Related To The Quality of Services in DOTS FacilitiesSeptina Esthy AyuNo ratings yet
- 1 35Document8 pages1 35Saiful HudaNo ratings yet
- CRA 2010-Poster-PresentationsDocument236 pagesCRA 2010-Poster-PresentationsJoe GassNo ratings yet
- HIV and TuberculosisDocument9 pagesHIV and TuberculosisDian NinaNo ratings yet
- Document PDFDocument7 pagesDocument PDFnur fadlilahNo ratings yet
- Ppa 10 1063Document8 pagesPpa 10 1063MyaSopNo ratings yet
- Wabah TBC Di VietnamDocument8 pagesWabah TBC Di VietnamSatya WangsaNo ratings yet
- Stories From Frequent Attenders: A Qualitative Study in Primary CareDocument7 pagesStories From Frequent Attenders: A Qualitative Study in Primary CareAlmudena Alameda CuestaNo ratings yet
- Economic and Survival Burden of Dysphagia Among Inpatients in The United StatesDocument7 pagesEconomic and Survival Burden of Dysphagia Among Inpatients in The United StatesClaudia Lorena MedinaNo ratings yet
- Efficiency of Web Application and Spaced Repetition Algorithms As An Aid in Preparing To Practical Examination of HistologyDocument2 pagesEfficiency of Web Application and Spaced Repetition Algorithms As An Aid in Preparing To Practical Examination of HistologyduffuchimpsNo ratings yet
- Chahine 2008Document8 pagesChahine 2008jumabarrientosNo ratings yet
- Huang 2019Document10 pagesHuang 2019blume diaNo ratings yet
- 1 PBDocument9 pages1 PBkpbugisNo ratings yet
- Ghana study finds over half of TB patients malnourished at start of treatmentDocument7 pagesGhana study finds over half of TB patients malnourished at start of treatmentSyahrul Hamidi NasutionNo ratings yet
- Jurnal 1Document6 pagesJurnal 1Pratiwi AyuningtyasNo ratings yet
- Journal of Clinical Tuberculosis and Other Mycobacterial DiseasesDocument16 pagesJournal of Clinical Tuberculosis and Other Mycobacterial DiseasesIlna RamadhaniNo ratings yet
- 2006 Article BF02351499Document10 pages2006 Article BF02351499litzyouk8381No ratings yet
- Fredrick Alleni Mfinanga and Tafuteni Nicholaus Chusi and Agnes B. ChaweneDocument6 pagesFredrick Alleni Mfinanga and Tafuteni Nicholaus Chusi and Agnes B. ChaweneinventionjournalsNo ratings yet
- Understanding The Gaps in DR TB Care Casc - 2020 - Journal of Clinical TuberculoDocument16 pagesUnderstanding The Gaps in DR TB Care Casc - 2020 - Journal of Clinical TuberculoKarina ChristantoNo ratings yet
- Pharmaceutical Sciences: Factors Contributing To Poor Compliance With Anti-Tb Treatment Among Tuberculosis PatientsDocument6 pagesPharmaceutical Sciences: Factors Contributing To Poor Compliance With Anti-Tb Treatment Among Tuberculosis PatientsMehreen KhanNo ratings yet
- Kenia Afirca ResilienciaDocument7 pagesKenia Afirca ResilienciaBlanca PacsiNo ratings yet
- Blood PressureDocument13 pagesBlood PressuremerlinNo ratings yet
- BullyingDocument2 pagesBullyingsherrybrarNo ratings yet
- JTLD 27 03 10 - 1..8Document9 pagesJTLD 27 03 10 - 1..8Reixel Raquel MugruzaNo ratings yet
- JurnalDocument7 pagesJurnalyenni elfiraNo ratings yet
- Hiv Fix 2Document7 pagesHiv Fix 2Wulan CerankNo ratings yet
- Evaluation and Management of Dysphagia: An Evidence-Based ApproachFrom EverandEvaluation and Management of Dysphagia: An Evidence-Based ApproachDhyanesh A. PatelNo ratings yet
- Tuberculosis Report 2019Document8 pagesTuberculosis Report 2019Rossita PrastiwiNo ratings yet
- SR Drop Out BrazilDocument10 pagesSR Drop Out Brazilsuci K SariNo ratings yet
- Mix Metod1Document13 pagesMix Metod1suci K SariNo ratings yet
- Kruk Et Al-2008-Tropical Medicine & International HealthDocument10 pagesKruk Et Al-2008-Tropical Medicine & International Healthsuci K SariNo ratings yet
- Free Printable 2018 Muslim Planner PDFDocument125 pagesFree Printable 2018 Muslim Planner PDFPujja Sari Purnama100% (1)
- Cost of Fellowship Program CourseDocument3 pagesCost of Fellowship Program CourseainihanifiahNo ratings yet
- Initial Nurse Patient InteractionDocument1 pageInitial Nurse Patient InteractionBryan Jay Carlo PañaNo ratings yet
- Peripartum Cardiomyopathy MedscapeDocument18 pagesPeripartum Cardiomyopathy MedscapeAji Isra SaputraNo ratings yet
- SCREENING FOR DISEASEDocument15 pagesSCREENING FOR DISEASEDr. Radhay ShyamNo ratings yet
- Basic Principle On Shad Kriya KalaDocument15 pagesBasic Principle On Shad Kriya KalaSiddhendu Bhattacharjee100% (1)
- Gestational Diabetus MellitusDocument28 pagesGestational Diabetus MellitusSanthosh.S.UNo ratings yet
- HIV and AIDS in Malawi Groups Most Affected by HIV in Malawi HIV Disproportionately Affects Women in Malawi PDFDocument14 pagesHIV and AIDS in Malawi Groups Most Affected by HIV in Malawi HIV Disproportionately Affects Women in Malawi PDFJames ChinamasaNo ratings yet
- Bureau of Fire Protection First AidDocument7 pagesBureau of Fire Protection First AidRexelle RamosNo ratings yet
- Concept MapDocument9 pagesConcept Mapapi-608044542No ratings yet
- Artesunato MefloquinaDocument11 pagesArtesunato MefloquinaDavid CerrónNo ratings yet
- COVID-19 poverty Philippines lockdowns job lossesDocument1 pageCOVID-19 poverty Philippines lockdowns job lossesRyza ParreñoNo ratings yet
- Jufex Forte LiteratureDocument5 pagesJufex Forte Literaturedan singh choudharyNo ratings yet
- Legislator Email on Safe Patient HandlingDocument5 pagesLegislator Email on Safe Patient HandlingAnonymous dcpGmD60% (5)
- Toward Nanotechnology-Enabled Approaches Against The COVID-19 PandemicDocument24 pagesToward Nanotechnology-Enabled Approaches Against The COVID-19 Pandemicmadcraft9832No ratings yet
- Hvac WorksDocument4 pagesHvac WorksSaleem BashaNo ratings yet
- Manage Severe Asthma EmergencyDocument17 pagesManage Severe Asthma EmergencyGanjar RaharjaNo ratings yet
- Clinical Presentation On AppendicectomyDocument30 pagesClinical Presentation On AppendicectomyValarmathiNo ratings yet
- Drug Study - MetronidazoleDocument1 pageDrug Study - MetronidazoleDeeRicachoMembela75% (16)
- Q3 Health 8 Module 1 PDFDocument15 pagesQ3 Health 8 Module 1 PDFkateNo ratings yet
- Fluids and Electrolytes in ElderlyDocument7 pagesFluids and Electrolytes in ElderlyDithaNo ratings yet
- Asuncion, Rachel Mae (Infectious Dse)Document3 pagesAsuncion, Rachel Mae (Infectious Dse)Rachel AsuncionNo ratings yet
- Korean Hand Acupuncture: A Unique and Highly Efficacious Branch of OMDocument4 pagesKorean Hand Acupuncture: A Unique and Highly Efficacious Branch of OMElanghovan ArumugamNo ratings yet
- CBT Blissful MaterialDocument223 pagesCBT Blissful MaterialDanial Hassan80% (5)
- Soal Ujian Sekolah Kls XIDocument6 pagesSoal Ujian Sekolah Kls XINUR FATWA PUTRI HUSAINNo ratings yet
- Contingency PLAN COVID 19 FIN Sept 29 2022Document35 pagesContingency PLAN COVID 19 FIN Sept 29 2022Fabro F. MhiseyNo ratings yet
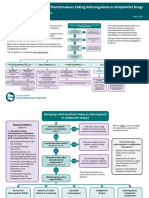
- Sdcep Anticoagulants Quick Reference Guide 2nd EditionDocument5 pagesSdcep Anticoagulants Quick Reference Guide 2nd EditionMeryem LahlouNo ratings yet
- Yamamoto Acupuncture PDFDocument17 pagesYamamoto Acupuncture PDFcarlos100% (1)
- IGC 2 - Element 7 - Chemical HazardsDocument67 pagesIGC 2 - Element 7 - Chemical HazardsHim SiwakotiNo ratings yet
- Community Health Nursing Diagnosis GGGDocument24 pagesCommunity Health Nursing Diagnosis GGGeen78% (9)
- Fixed Prosthodontics: Drg. Bertha E. Setio, SpprosDocument16 pagesFixed Prosthodontics: Drg. Bertha E. Setio, Spprosiin revient29No ratings yet