You might also like
- Free Version of Growthinks Vending Machine Business Plan TemplateDocument16 pagesFree Version of Growthinks Vending Machine Business Plan TemplateswdNo ratings yet
- Mirko Workout PDFDocument10 pagesMirko Workout PDFSirine Boussama100% (3)
- Communication in Marriage Reed 105Document28 pagesCommunication in Marriage Reed 105Erwin Y. CabaronNo ratings yet
- (START HERE) 7 Day Feminine Transformation WorkbookDocument37 pages(START HERE) 7 Day Feminine Transformation Workbookt6w5g27n4qNo ratings yet
- Stage 1 Overcoming Imposter Syndrome: What You Will LearnDocument4 pagesStage 1 Overcoming Imposter Syndrome: What You Will LearnPaul Ioan PopescuNo ratings yet
- Lateralviolenceamongnurses Areviewoftheliterature 1Document13 pagesLateralviolenceamongnurses Areviewoftheliterature 1api-519721866No ratings yet
- Date & Time Focus Data Action Response D: Into OR, A - Year Old - PerDocument2 pagesDate & Time Focus Data Action Response D: Into OR, A - Year Old - PerMichelle Gliselle Guinto MallareNo ratings yet
- Early Detection of Tuberculosis Through Community-Based Active Case Finding in CambodiaDocument11 pagesEarly Detection of Tuberculosis Through Community-Based Active Case Finding in CambodiaPatriciann13No ratings yet
- Efficiency of Web Application and Spaced Repetition Algorithms As An Aid in Preparing To Practical Examination of HistologyDocument2 pagesEfficiency of Web Application and Spaced Repetition Algorithms As An Aid in Preparing To Practical Examination of HistologyduffuchimpsNo ratings yet
- Outcomes of HIV-infected Children With Tuberculosis Who Are Started On Antiretroviral Therapy in MalawiDocument5 pagesOutcomes of HIV-infected Children With Tuberculosis Who Are Started On Antiretroviral Therapy in MalawiIrfan Dzakir NugrohoNo ratings yet
- 1 PBDocument9 pages1 PBkpbugisNo ratings yet
- Treatment Seeking Behavior and Factors Associated With Its Delay Among Newly Diagnosed Pulmonary Tuberculosis Patients in Bhopal, Madhya PradeshDocument6 pagesTreatment Seeking Behavior and Factors Associated With Its Delay Among Newly Diagnosed Pulmonary Tuberculosis Patients in Bhopal, Madhya PradeshAdvanced Research PublicationsNo ratings yet
- Risk of Tuberculosis Infection Among Community Health AgentsDocument6 pagesRisk of Tuberculosis Infection Among Community Health AgentsLuciana SaundersNo ratings yet
- Raghavendra Yarlagadda Temesgen Mulugeta Fanta Gashe Ramanjireddy Tatiparthi.Document18 pagesRaghavendra Yarlagadda Temesgen Mulugeta Fanta Gashe Ramanjireddy Tatiparthi.yraghavendraNo ratings yet
- Jurnal TBC ParuDocument8 pagesJurnal TBC ParuMaria FulgensiaNo ratings yet
- Medi 99 E23649Document6 pagesMedi 99 E23649kornelis aribowoNo ratings yet
- JTLD 27 03 10 - 1..8Document9 pagesJTLD 27 03 10 - 1..8Reixel Raquel MugruzaNo ratings yet
- 7a Fee ARTDocument12 pages7a Fee ARTVinod GaurNo ratings yet
- Nihms 1587191Document13 pagesNihms 1587191Vnime MusicNo ratings yet
- (Pro) Ing 1, Ada Kuesioner Juga12Document8 pages(Pro) Ing 1, Ada Kuesioner Juga12ilhamNo ratings yet
- 718-1519-1-SM 2Document6 pages718-1519-1-SM 2NicoleNo ratings yet
- Childhood Intussusceptions at A Tertiary Care Hospital in Northwestern Tanzania: A Diagnostic and Therapeutic Challenge in Resource-Limited SettingDocument8 pagesChildhood Intussusceptions at A Tertiary Care Hospital in Northwestern Tanzania: A Diagnostic and Therapeutic Challenge in Resource-Limited Settingegi lewisNo ratings yet
- Servikal TBDocument15 pagesServikal TBnur wahidaNo ratings yet
- Sample PresentationDocument36 pagesSample Presentationmuhammed essaNo ratings yet
- Pone 0142607 PDFDocument9 pagesPone 0142607 PDFNurul Muqarribah Pratiwi IshaqNo ratings yet
- Abstracts COMAPI 2014 IJMSDocument20 pagesAbstracts COMAPI 2014 IJMSfelipetheNo ratings yet
- Prevalence and Determinants of Human Immunodeficiency Virus and Tuberculosis Co-Infection at Kampala International University Teaching HospitalDocument6 pagesPrevalence and Determinants of Human Immunodeficiency Virus and Tuberculosis Co-Infection at Kampala International University Teaching HospitalKIU PUBLICATION AND EXTENSIONNo ratings yet
- Adiutarini 6Document12 pagesAdiutarini 6Eva Tirtabayu HasriNo ratings yet
- Research Article: Characteristics and Treatment Outcomes of Retreatment Tuberculosis Patients in BeninDocument7 pagesResearch Article: Characteristics and Treatment Outcomes of Retreatment Tuberculosis Patients in BeninfaustinaNo ratings yet
- As Preventive TherapyDocument6 pagesAs Preventive TherapymutimutimutiNo ratings yet
- Oup Accepted Manuscript 2020Document10 pagesOup Accepted Manuscript 2020Najla rayNo ratings yet
- Factors Affecting Patient Compliance With Anti-Tuberculosis Chemotherapy Using The Directly Observed Treatment, Short-Course Strategy (DOTS)Document6 pagesFactors Affecting Patient Compliance With Anti-Tuberculosis Chemotherapy Using The Directly Observed Treatment, Short-Course Strategy (DOTS)suci K SariNo ratings yet
- 1 - Incidence of Tuberculosis Meningitis in A High HIV Prevalence Serie de Caso 2018 (Modelo para o Trabalho)Document9 pages1 - Incidence of Tuberculosis Meningitis in A High HIV Prevalence Serie de Caso 2018 (Modelo para o Trabalho)SERGIO LOBATO FRANÇANo ratings yet
- Novitasari - Is Premigration Health Screening For Tuberculosis WorthwileDocument12 pagesNovitasari - Is Premigration Health Screening For Tuberculosis Worthwileontet28No ratings yet
- Mortality Among Tuberculosis Patients in The Democratic Republic of CongoDocument7 pagesMortality Among Tuberculosis Patients in The Democratic Republic of CongoGary Rios DionicioNo ratings yet
- Plasma Biomarkers To Detect Prevalent, or Predict Progressive, HIV-1-associated TuberculosisDocument21 pagesPlasma Biomarkers To Detect Prevalent, or Predict Progressive, HIV-1-associated TuberculosisPaulo MattosNo ratings yet
- Assessment of Knowledge, Attitudes and Perceptions Regarding Ebola Disease in Healthcare Workers From A Tertiary Care Hospital in RomaniaDocument9 pagesAssessment of Knowledge, Attitudes and Perceptions Regarding Ebola Disease in Healthcare Workers From A Tertiary Care Hospital in RomaniaAli GhanemNo ratings yet
- Implementasi Penemuan Suspek Tuberkulosis Di Puskesmas Kabupaten Pesisir SelatanDocument14 pagesImplementasi Penemuan Suspek Tuberkulosis Di Puskesmas Kabupaten Pesisir Selatantiara_kusumaningtyasNo ratings yet
- Clinical Science Session-IsTCDocument17 pagesClinical Science Session-IsTCSari HarahapNo ratings yet
- 197828-Article Text-498080-1-10-20200722Document8 pages197828-Article Text-498080-1-10-20200722ሀይደር ዶ.ርNo ratings yet
- Long Term Outcomes of A Pediatric HIV Treatment Program in Maputo Mozambique A Cohort StudyDocument10 pagesLong Term Outcomes of A Pediatric HIV Treatment Program in Maputo Mozambique A Cohort StudyKevin RadittyaNo ratings yet
- Tuberculosis Treatment Delay and Nosocomial Exposure Remain Important Risks For Patients Undergoing Regular HemodialysisDocument9 pagesTuberculosis Treatment Delay and Nosocomial Exposure Remain Important Risks For Patients Undergoing Regular HemodialysisRayCassidyNo ratings yet
- Review Afb Neg CultureDocument7 pagesReview Afb Neg Cultureธิรดา สายสตรอง สายจำปาNo ratings yet
- Socio-Demographic Factors Affecting Knowledge Level of Tuberculosis Patients in Rajshahi City, BangladeshDocument6 pagesSocio-Demographic Factors Affecting Knowledge Level of Tuberculosis Patients in Rajshahi City, BangladeshGusti Oey Part IINo ratings yet
- Nihpp rs3758745v1Document20 pagesNihpp rs3758745v1Yulia Niswatul FauziyahNo ratings yet
- Out-of-Pocket Costs For Patients Diagnosed With Tuberculosis in Different Healthcare Settings in Bandung, IndonesiaDocument8 pagesOut-of-Pocket Costs For Patients Diagnosed With Tuberculosis in Different Healthcare Settings in Bandung, Indonesiagshalimar shalNo ratings yet
- Abstract 59Document3 pagesAbstract 59Jarvis WheelerNo ratings yet
- Contemporary Clinical Trials: SciencedirectDocument10 pagesContemporary Clinical Trials: SciencedirectFristune NewNo ratings yet
- Research On Prevalence of TB FinalDocument9 pagesResearch On Prevalence of TB FinalBontuNo ratings yet
- Pone 0198080Document15 pagesPone 0198080kornelis aribowoNo ratings yet
- Fetch ObjectDocument7 pagesFetch ObjectBilly UntuNo ratings yet
- Screening Program For Lung Tuberculosis in Adult A-3Document42 pagesScreening Program For Lung Tuberculosis in Adult A-3bramNo ratings yet
- Undiagnosed Tuberculosis in Patients With HIV Infection Who Present With Severe Anaemia at A District HospitalDocument6 pagesUndiagnosed Tuberculosis in Patients With HIV Infection Who Present With Severe Anaemia at A District HospitalDian EsthyNo ratings yet
- Knowledge On HIV/AIDS Among Students of The Faculty of Health Sciences, Brazzaville, Republic of CongoDocument14 pagesKnowledge On HIV/AIDS Among Students of The Faculty of Health Sciences, Brazzaville, Republic of CongoNovita HerlitadewiNo ratings yet
- PDFDocument9 pagesPDFsatriobudi_wicaksonoNo ratings yet
- Tuberculosis Thesis TitleDocument5 pagesTuberculosis Thesis Titletjgyhvjef100% (2)
- Leprosy and contact surveillance: active screening detects cases earlierDocument6 pagesLeprosy and contact surveillance: active screening detects cases earlierAjie WitamaNo ratings yet
- IJTLDeditorial Protecting HCworkers Form TBDocument2 pagesIJTLDeditorial Protecting HCworkers Form TBRoma ParyaniNo ratings yet
- DK 1Document5 pagesDK 1Isnila F. KelilauwNo ratings yet
- 1201 Sanchez Padilla High Prevalence of Multidrug Resistant Tuberculosis Swaziland 2009 2010 Emerging Infectious Diseases 18 1Document9 pages1201 Sanchez Padilla High Prevalence of Multidrug Resistant Tuberculosis Swaziland 2009 2010 Emerging Infectious Diseases 18 1dewi ayu wulandariNo ratings yet
- Rapid Drug Susceptibility Testing and Treatment Outcomes For Multidrug-Resistant Tuberculosis in PeruDocument9 pagesRapid Drug Susceptibility Testing and Treatment Outcomes For Multidrug-Resistant Tuberculosis in Perucarlos castañon reyesNo ratings yet
- Ajol File Journals - 494 - Articles - 112516 - Submission - Proof - 112516 5833 312396 1 10 20150204Document6 pagesAjol File Journals - 494 - Articles - 112516 - Submission - Proof - 112516 5833 312396 1 10 20150204ASK De OliveiraNo ratings yet
- Placement Report: Good Shepherd Hospital, SwazilandDocument22 pagesPlacement Report: Good Shepherd Hospital, SwazilandNaftal ShetunyengaNo ratings yet
- Postoperative Nausea and Vomiting at A Tertiary Care Hospital in North-Western TanzaniaDocument9 pagesPostoperative Nausea and Vomiting at A Tertiary Care Hospital in North-Western TanzaniaAsfaw NurhussenNo ratings yet
- 2017 Article 2662Document11 pages2017 Article 2662Dhani KurniawanNo ratings yet
- Diagnostic Imaging of Novel Coronavirus PneumoniaFrom EverandDiagnostic Imaging of Novel Coronavirus PneumoniaMinming ZhangNo ratings yet
- Living on the Frontline of COVID-19 in MCO And CMCO: Clinical Updates in COVID-19From EverandLiving on the Frontline of COVID-19 in MCO And CMCO: Clinical Updates in COVID-19No ratings yet
- Global Healthcare Sample Abstract NOV1Document2 pagesGlobal Healthcare Sample Abstract NOV1Hermenegildo chitumbaNo ratings yet
- Ojs Checklist-Fin2 PDFDocument11 pagesOjs Checklist-Fin2 PDFHermenegildo chitumbaNo ratings yet
- Ojs Checklist-Fin2 PDFDocument11 pagesOjs Checklist-Fin2 PDFHermenegildo chitumbaNo ratings yet
- Files Without This Message by Purchasing Novapdf PrinterDocument1 pageFiles Without This Message by Purchasing Novapdf PrinterHermenegildo chitumbaNo ratings yet
- ToryDocument3 pagesToryHermenegildo chitumbaNo ratings yet
- ACUTE KIDNEY INJURY SIGNS, SYMPTOMS, AND CAUSESDocument10 pagesACUTE KIDNEY INJURY SIGNS, SYMPTOMS, AND CAUSESYanti TandjungNo ratings yet
- List of Approved INGOsDocument4 pagesList of Approved INGOsZain JavedNo ratings yet
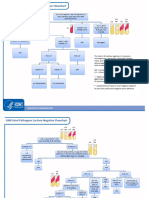
- GNR Stool Pathogens Lactose Negative FlowchartDocument2 pagesGNR Stool Pathogens Lactose Negative FlowchartKeithNo ratings yet
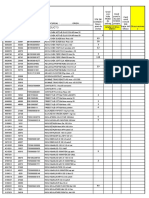
- AL CIERRE DE Julio Del 2021: Barra COD AlfabetaDocument2 pagesAL CIERRE DE Julio Del 2021: Barra COD AlfabetaBrian Javier GomezNo ratings yet
- HEALTH-CARE SYSTEMS: CULTURAL, SOCIAL AND PROFESSIONAL ASPECTSDocument16 pagesHEALTH-CARE SYSTEMS: CULTURAL, SOCIAL AND PROFESSIONAL ASPECTSWasima TabassumNo ratings yet
- Introduction To Basic Food PreparationDocument18 pagesIntroduction To Basic Food PreparationJiety PlarisanNo ratings yet
- Paternal Love EssayDocument2 pagesPaternal Love Essayfhlorievy langomezNo ratings yet
- Act Cart InterventionDocument21 pagesAct Cart Interventionapi-645942287No ratings yet
- Impact of Fast Food Consumption On Health: IjrtbtDocument5 pagesImpact of Fast Food Consumption On Health: IjrtbtAnisha AmmuNo ratings yet
- 9 ErDocument13 pages9 Ermartin Ignacio Zapata LaguadoNo ratings yet
- Locate Indian Oil Petrol Pump in Belgaum District of Karnataka StateDocument20 pagesLocate Indian Oil Petrol Pump in Belgaum District of Karnataka StateDeva Chandra SekharNo ratings yet
- Board and Reviewer Assignments for Convened IRB ReviewDocument5 pagesBoard and Reviewer Assignments for Convened IRB ReviewMuhammad Zaryab KhanNo ratings yet
- Hospital Business ModelsDocument8 pagesHospital Business ModelsPOLOKO MHUSIWANo ratings yet
- Middle East CaravanDocument20 pagesMiddle East CaravanB2B AFRICANo ratings yet
- Lesson 1:: Introduction To Science, Technology and SocietyDocument17 pagesLesson 1:: Introduction To Science, Technology and SocietyAlexis A. AguilarNo ratings yet
- Curriculam Vitae: ObjectiveDocument5 pagesCurriculam Vitae: ObjectiveGokul RajNo ratings yet
- Module 2Document43 pagesModule 2jbg060595No ratings yet
- Reviewing Literature Learning Disability Fiction and The Social Work PerspectiveDocument13 pagesReviewing Literature Learning Disability Fiction and The Social Work Perspectiveauthor.avengingangelNo ratings yet
- CrossFit®-Injury Prevalence and Main Risk Factors (Curiosidade)Document5 pagesCrossFit®-Injury Prevalence and Main Risk Factors (Curiosidade)TUTOR PAULO EDUARDO REDKVANo ratings yet
- RX Kianbradleyjowett 20240319 080316 0000Document1 pageRX Kianbradleyjowett 20240319 080316 0000cleofeleighclarkNo ratings yet
- Ey Work SampleDocument10 pagesEy Work SampleKris ANo ratings yet
- Bionic Final PDFDocument4 pagesBionic Final PDFJasmine RaoNo ratings yet
- Tutorial 1A - Public HealthDocument22 pagesTutorial 1A - Public Healthmuhammad saufi sulaimanNo ratings yet