You might also like
- Archer USMLE Step 3 Question BankDocument116 pagesArcher USMLE Step 3 Question Bankrolpf garri33% (3)
- The Myth of Autism: How a Misunderstood Epidemic Is Destroying Our Children, Expanded and Revised EditionFrom EverandThe Myth of Autism: How a Misunderstood Epidemic Is Destroying Our Children, Expanded and Revised EditionRating: 2.5 out of 5 stars2.5/5 (3)
- 2020-Biochem-Activity-16 - BIOCHEMISTRY OF HORMONESDocument32 pages2020-Biochem-Activity-16 - BIOCHEMISTRY OF HORMONESGabrielle John HernaezNo ratings yet
- Empty Sella Syndrome: Continuing Education ActivityDocument8 pagesEmpty Sella Syndrome: Continuing Education Activityn2763288No ratings yet
- Cerebral Palsy Practice Essentials: Signs and SymptomsDocument11 pagesCerebral Palsy Practice Essentials: Signs and SymptomsTahsinur RahmanNo ratings yet
- Syncope 3Document19 pagesSyncope 3Pratyush PrateekNo ratings yet
- Clinical Autonomic and Mitochondrial Disorders: Diagnosis, Prevention, and Treatment for Mind-Body WellnessFrom EverandClinical Autonomic and Mitochondrial Disorders: Diagnosis, Prevention, and Treatment for Mind-Body WellnessNo ratings yet
- Primary Empty Sella Syndrome and The Prevalence of Hormonal DysregulationDocument9 pagesPrimary Empty Sella Syndrome and The Prevalence of Hormonal DysregulationHantiukNo ratings yet
- The Stress System in The Human Brain in Depression and NeurodegenerationDocument54 pagesThe Stress System in The Human Brain in Depression and NeurodegenerationRomeo IsaíasNo ratings yet
- 2021 - Apnea Central Del Sueño @ishikawaDocument13 pages2021 - Apnea Central Del Sueño @ishikawaJorge Toshio Yazawa ChaconNo ratings yet
- Posterior Reversible Encephalopathy Syndrome (Pres) in A Patient With Late Postpartum Eclampsia: Case ReportDocument4 pagesPosterior Reversible Encephalopathy Syndrome (Pres) in A Patient With Late Postpartum Eclampsia: Case ReportIJAR JOURNALNo ratings yet
- Avoiding Common Errors in The Emergency Department-801-1002Document200 pagesAvoiding Common Errors in The Emergency Department-801-1002Hernando CastrillónNo ratings yet
- The Myth of Autism: How a Misunderstood Epidemic Is Destroying Our ChildrenFrom EverandThe Myth of Autism: How a Misunderstood Epidemic Is Destroying Our ChildrenRating: 2.5 out of 5 stars2.5/5 (8)
- Cerebellar DisordersDocument12 pagesCerebellar DisordersAnn SamNo ratings yet
- Childhood-Onset Schizophrenia with Complete Corpus Callosum AgenesisDocument4 pagesChildhood-Onset Schizophrenia with Complete Corpus Callosum AgenesisBhagyaraj JeevangiNo ratings yet
- Hypoxic-Ischemic Encephalopathy: Practice EssentialsDocument38 pagesHypoxic-Ischemic Encephalopathy: Practice EssentialsPasien ICU RSUINo ratings yet
- Amenorrhea WorkupDocument10 pagesAmenorrhea WorkupHaoKeat HoeNo ratings yet
- NPH BookletDocument41 pagesNPH BookletDini NanamiNo ratings yet
- Practical Neurology (Cerebellar Ataxia)Document11 pagesPractical Neurology (Cerebellar Ataxia)idno1008No ratings yet
- Now You See It, Case ReportDocument6 pagesNow You See It, Case ReportPhilip McNelsonNo ratings yet
- Endo Part IVDocument40 pagesEndo Part IVChippy RabeNo ratings yet
- Progress AsfiksiaDocument8 pagesProgress AsfiksiaNi Wayan Ana PsNo ratings yet
- Neonatal Asphyxia Management and Therapeutic HypothermiaDocument68 pagesNeonatal Asphyxia Management and Therapeutic HypothermiaAprilliaNo ratings yet
- Sleep Consult TemplateDocument5 pagesSleep Consult Templatesbonvallet3912100% (1)
- Catamenial Epilepsy: Definition, Prevalence Pathophysiology and TreatmentDocument9 pagesCatamenial Epilepsy: Definition, Prevalence Pathophysiology and TreatmentastriNo ratings yet
- Epilepticus: Morbidity and MortalityDocument5 pagesEpilepticus: Morbidity and MortalityIndah Maharani NasutionNo ratings yet
- Dr. Waqas Ayubian Notes For Step 3Document772 pagesDr. Waqas Ayubian Notes For Step 3Muhammad HammadNo ratings yet
- Pulmonary hypertension causes and symptomsDocument10 pagesPulmonary hypertension causes and symptomscharmieangelNo ratings yet
- Neonatal Asphyxia Causes & EffectsDocument15 pagesNeonatal Asphyxia Causes & Effectsmin09hihiNo ratings yet
- Herrera 2016Document16 pagesHerrera 2016Farin MauliaNo ratings yet
- Hanhan 2001Document12 pagesHanhan 2001ATIKAH NUR HAFIZHAHNo ratings yet
- Spontaneous Intracranial Hypotension - Diagnosis and ManagementDocument3 pagesSpontaneous Intracranial Hypotension - Diagnosis and ManagementMazin Al-TahirNo ratings yet
- In This Issue: Mitochondrial Disease and Dysautonomia: Exploring The LiteratureDocument17 pagesIn This Issue: Mitochondrial Disease and Dysautonomia: Exploring The LiteraturedoctornulNo ratings yet
- Cerebral Perfusion Pressure and Autoregulation inDocument9 pagesCerebral Perfusion Pressure and Autoregulation inayu permata dewiNo ratings yet
- Q 2005 Society of The European Journal of Endocrinology DOI: 10.1530/eje.1.01911Document7 pagesQ 2005 Society of The European Journal of Endocrinology DOI: 10.1530/eje.1.01911Hasnae HassaniNo ratings yet
- ESSDocument41 pagesESSSushma MalladiNo ratings yet
- On Fetal MeasureDocument40 pagesOn Fetal MeasureHarish Labana100% (2)
- Obstructive Sleep Apnoea Syndrome A Systematic Literature ReviewDocument4 pagesObstructive Sleep Apnoea Syndrome A Systematic Literature Reviewc5nah867No ratings yet
- Block 2 Assignment Edited Catherine Ruguru SamsonDocument12 pagesBlock 2 Assignment Edited Catherine Ruguru Samsonmoses karituNo ratings yet
- Likely Cause of Lady's Atrial FibrillationDocument5 pagesLikely Cause of Lady's Atrial FibrillationZhao Xuan TanNo ratings yet
- Neonate With AcrocyanosisDocument4 pagesNeonate With Acrocyanosisnurul noviarisaNo ratings yet
- 121 Anaesthesia For VP Shunt InsertionDocument8 pages121 Anaesthesia For VP Shunt InsertionMohammed ElSayedNo ratings yet
- Cerebellar DisordersDocument16 pagesCerebellar DisordersNur Ajiyanti 'anthi' SabirinaNo ratings yet
- Abses Serebri2 PDFDocument22 pagesAbses Serebri2 PDFRagillia Irena FebriNo ratings yet
- Cerebral SLE Case Report and Diagnostic Test EvaluationDocument9 pagesCerebral SLE Case Report and Diagnostic Test EvaluationrandyardinalNo ratings yet
- 1b. EclampsiaDocument14 pages1b. EclampsiaJuan P. RuedaNo ratings yet
- Neurology: Left Homonymous HemianopiaDocument4 pagesNeurology: Left Homonymous HemianopiaAmmad JavedNo ratings yet
- Cerebral Palsy The ABC's: of CPDocument43 pagesCerebral Palsy The ABC's: of CPravannofanizzaNo ratings yet
- Management of Fetal Distress: StephanieDocument16 pagesManagement of Fetal Distress: Stephanieyenni anggrainiNo ratings yet
- Perinatal Asphyxia GuideDocument37 pagesPerinatal Asphyxia GuideHomeground entertainmentNo ratings yet
- Eclampsia - UpToDateDocument42 pagesEclampsia - UpToDateGinaNo ratings yet
- Carotid SinusDocument20 pagesCarotid SinusPratyush PrateekNo ratings yet
- Cerebrovascular AccidentDocument30 pagesCerebrovascular AccidentRichard Charles UmlasNo ratings yet
- Antiphospholipid Syndrome and Pregnancy (Dengan Foto Punya DR RositaDocument9 pagesAntiphospholipid Syndrome and Pregnancy (Dengan Foto Punya DR RositadidongNo ratings yet
- Penatalaksanaan Anestesia Pada Preeklampsia Dan Eklampsia U. Kaswiyan ADocument19 pagesPenatalaksanaan Anestesia Pada Preeklampsia Dan Eklampsia U. Kaswiyan AReyhan CalabroNo ratings yet
- Fetal Biophysical Profile. A Critical Appraisal PDFDocument11 pagesFetal Biophysical Profile. A Critical Appraisal PDFchronos6534No ratings yet
- ENLS Sub-Arachnoid Hemorrhage ProtocolDocument22 pagesENLS Sub-Arachnoid Hemorrhage ProtocolFransiskus MikaelNo ratings yet
- Cardiac Evaluation of ThenewbornDocument19 pagesCardiac Evaluation of ThenewbornChristian MartínezNo ratings yet
- Care of Unconscious PatientDocument6 pagesCare of Unconscious PatientSuparna SinghaNo ratings yet
- Art 1Document4 pagesArt 1Claudia IrimieNo ratings yet
- Increased Intracranial PressureDocument2 pagesIncreased Intracranial PressureCheryl Lim SorianoNo ratings yet
- (PED) T.10.2 - Pediatric Endocrinology (Part II) PDFDocument7 pages(PED) T.10.2 - Pediatric Endocrinology (Part II) PDFLiberty AgcaoiliNo ratings yet
- Drugs Effecting On Thyroid Gland: Abdullaev Dzhumadil, PharmdDocument22 pagesDrugs Effecting On Thyroid Gland: Abdullaev Dzhumadil, PharmdRtxGaming Zone 73No ratings yet
- Lect.10 Acromegaly, Gigantism and OthersDocument10 pagesLect.10 Acromegaly, Gigantism and OthersShubhamNo ratings yet
- Adrenal CrisisDocument25 pagesAdrenal CrisisKusum RoyNo ratings yet
- SAS #16 NUR 151: Your Email Will Be Recorded When You Submit This FormDocument7 pagesSAS #16 NUR 151: Your Email Will Be Recorded When You Submit This FormA.No ratings yet
- Adrenal Cortex DR - GomezDocument13 pagesAdrenal Cortex DR - Gomezvicbart11No ratings yet
- With DR WajeihDocument62 pagesWith DR WajeihZeeshan AhmedNo ratings yet
- Science 10 ReviewerDocument14 pagesScience 10 ReviewerMonique FranciscoNo ratings yet
- Coordination and Control in Science Class XDocument11 pagesCoordination and Control in Science Class Xbhargavthegreat123No ratings yet
- Human Reproduction - DPP 10 (Of Lecture 14) - Lakshya NEET 2024Document3 pagesHuman Reproduction - DPP 10 (Of Lecture 14) - Lakshya NEET 2024Ankit BhartiNo ratings yet
- Anatomy and Physiology of ThyroidDocument23 pagesAnatomy and Physiology of ThyroidPonnan DasaiyanNo ratings yet
- First Summative Test Science 5Document3 pagesFirst Summative Test Science 5Gil Arriola100% (2)
- Posterior Pituitary: DR Axelle Saverettiar Mbbs Physiology Department SSR Medical CollegeDocument60 pagesPosterior Pituitary: DR Axelle Saverettiar Mbbs Physiology Department SSR Medical CollegeÑäd ÉèmNo ratings yet
- HS140 Unit 8 Quiz Study Guide-Oct2011Document3 pagesHS140 Unit 8 Quiz Study Guide-Oct2011Crystal MendiolaNo ratings yet
- Las 1Document5 pagesLas 1rosemarie lingonNo ratings yet
- Hiper Dan Hipotiroid (Revisi)Document76 pagesHiper Dan Hipotiroid (Revisi)AgusNo ratings yet
- Intro To EthologyDocument3 pagesIntro To EthologyRowzFerlTanutanNo ratings yet
- The Renin Angiotensin Aldosterone System - RAASDocument3 pagesThe Renin Angiotensin Aldosterone System - RAASrienz nicnic peraltaNo ratings yet
- Basic Word Structure Roots Suffixes PrefixesDocument3 pagesBasic Word Structure Roots Suffixes PrefixesFrancisco Martinez GarciaNo ratings yet
- Macario Biology W1Document6 pagesMacario Biology W1Roberto MendozaNo ratings yet
- Thyroid Function TestDocument21 pagesThyroid Function TestPat JacintoNo ratings yet
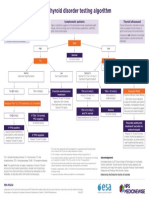
- NPS MedicineWise Thyroid Testing Algorithm v3Document1 pageNPS MedicineWise Thyroid Testing Algorithm v3Mikhael JHNo ratings yet
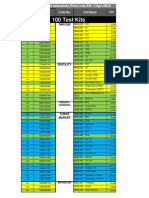
- 100 Test Kits: Golden Harvest Industries Price List Eff: 1-Apr-2019Document3 pages100 Test Kits: Golden Harvest Industries Price List Eff: 1-Apr-2019Naveed AbrarNo ratings yet
- Coordination of Body Functions by Chemical MessengerDocument6 pagesCoordination of Body Functions by Chemical MessengerHorain FatimaNo ratings yet
- ELISA Test For The Quantitative Determination of Total Thyroxine (T4) in Human SerumDocument2 pagesELISA Test For The Quantitative Determination of Total Thyroxine (T4) in Human SerumMaherNo ratings yet
- MRCP EndocrineDocument94 pagesMRCP EndocrineMarwan M.100% (3)
- Nejmoa 2111953Document10 pagesNejmoa 2111953Andreea VlădanNo ratings yet
- Obstetrics and Gynecology Sixth Edition Obstetrics and Gynecology Beckman Chapter 36Document8 pagesObstetrics and Gynecology Sixth Edition Obstetrics and Gynecology Beckman Chapter 363hondoNo ratings yet
- 702 FullDocument54 pages702 FullAndrew Hukom100% (1)