You might also like
- Neurological ExaminationDocument216 pagesNeurological Examinationkid_latigo100% (4)
- Riker ABSITE ReviewDocument36 pagesRiker ABSITE Reviewsgod34No ratings yet
- Damage Control SurgeryDocument31 pagesDamage Control SurgeryDyo Resna100% (1)
- Musculoskeletal SystemDocument93 pagesMusculoskeletal Systemromeo jr mostolesNo ratings yet
- Liver Abscesses and CystsDocument6 pagesLiver Abscesses and CystsbintangsebayangNo ratings yet
- Peripartum Hysterectomy - Incidence, Indications, Risk Factors and Outcomes at A Teritiary Care HospitalDocument4 pagesPeripartum Hysterectomy - Incidence, Indications, Risk Factors and Outcomes at A Teritiary Care HospitalIJAR JOURNALNo ratings yet
- Living with Metastatic Breast Cancer: Stories of Faith and HopeFrom EverandLiving with Metastatic Breast Cancer: Stories of Faith and HopeNo ratings yet
- Management of Anastomotic Complications of Colorectal SurgeryDocument13 pagesManagement of Anastomotic Complications of Colorectal Surgerydadupipa100% (1)
- Probiotics Improve Long Covid PDFDocument9 pagesProbiotics Improve Long Covid PDFSANTA HILDEGARDA DE BINGEN100% (1)
- Liposuccion Alta Definicion PDFDocument10 pagesLiposuccion Alta Definicion PDFDIOGENESNo ratings yet
- Ventilator Alarms and TroubleshootingDocument23 pagesVentilator Alarms and Troubleshootingjanubiomed0209100% (1)
- Cancer and Oncology Nursing NCLEX Practice Quiz-1Document30 pagesCancer and Oncology Nursing NCLEX Practice Quiz-1Susie Salmon100% (2)
- Fulminant Hepatic FailureDocument12 pagesFulminant Hepatic Failureafghansyah arfiantoNo ratings yet
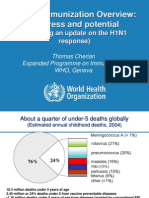
- Global Immunization Overview: Progress and PotentialDocument36 pagesGlobal Immunization Overview: Progress and PotentialPrabir Kumar ChatterjeeNo ratings yet
- Screening For Breast CancerDocument20 pagesScreening For Breast CancerqalbiNo ratings yet
- Gowri BongaigaonDocument32 pagesGowri BongaigaonGowri ShankarNo ratings yet
- Intravascular Ultrasound To Guide Left Main Stem Intervention A Sub Study of TheDocument19 pagesIntravascular Ultrasound To Guide Left Main Stem Intervention A Sub Study of Themayra osorioNo ratings yet
- Vismodegib in Neoadjuvant Treatment of Locally AdvDocument8 pagesVismodegib in Neoadjuvant Treatment of Locally Advcrazynoel411No ratings yet
- Apovian 2016Document10 pagesApovian 2016Sandy PranadaNo ratings yet
- Colorectal Cancer USTH Endoscopy Unit Are We Effective in Screening?Document27 pagesColorectal Cancer USTH Endoscopy Unit Are We Effective in Screening?Elton TiglaoNo ratings yet
- MRM ArticleDocument5 pagesMRM ArticleRekha Tulsi KhatriNo ratings yet
- Acne Vulgaris 1Document4 pagesAcne Vulgaris 1Ridho ForesNo ratings yet
- Breast Cancer Overview - Dr. Jamal Melhem 25 Sept. 2016Document69 pagesBreast Cancer Overview - Dr. Jamal Melhem 25 Sept. 2016Mohammad BanisalmanNo ratings yet
- Incidence and Treatment of Complications in PatientsDocument6 pagesIncidence and Treatment of Complications in Patientszfadhli.s.96No ratings yet
- CA A Cancer J Clinicians - July August 1995 - Hortobagyi - Current Status of Adjuvant Systemic Therapy For Primary BreastDocument28 pagesCA A Cancer J Clinicians - July August 1995 - Hortobagyi - Current Status of Adjuvant Systemic Therapy For Primary Breastryan aniceteNo ratings yet
- Quiz 3 MicroeconomicsDocument3 pagesQuiz 3 MicroeconomicsNguyễn Đức ThắngNo ratings yet
- Manuscript Vulvar CancerDocument5 pagesManuscript Vulvar CancerYudha GanesaNo ratings yet
- Pathology Case Presentation: Prepared by Roll No.s 1-9Document20 pagesPathology Case Presentation: Prepared by Roll No.s 1-9vishalzenia100% (1)
- JPM 12 01098 v2Document11 pagesJPM 12 01098 v2Rizki FebriyaniNo ratings yet
- Research FINAL-wordDocument23 pagesResearch FINAL-wordJahnenNo ratings yet
- Conservative Surgery For Ovarian TorsionDocument9 pagesConservative Surgery For Ovarian TorsionRizka AdiNo ratings yet
- Nipple DischargeDocument8 pagesNipple DischargeGabriela Zavaleta CamachoNo ratings yet
- The Surgeon's Guide To Fibroadenomas: Katherine Kopkash, Katharine YaoDocument8 pagesThe Surgeon's Guide To Fibroadenomas: Katherine Kopkash, Katharine YaoKarina WirajayaNo ratings yet
- Predictors of the risk of fibrosis at 10 years after breast conserving therapy for early breast cancer – A study based on the EORTC trial 22881–10882 ‘boost versus no boost’ / European Journal of Cancer Collette, 2008Document13 pagesPredictors of the risk of fibrosis at 10 years after breast conserving therapy for early breast cancer – A study based on the EORTC trial 22881–10882 ‘boost versus no boost’ / European Journal of Cancer Collette, 2008saipraveen03No ratings yet
- NMSC Excision Margins AuditDocument36 pagesNMSC Excision Margins AuditnuwanrajapakshaNo ratings yet
- Best-Practice Care Pathway For Improving Management of Mastitis and Breast AbscessDocument8 pagesBest-Practice Care Pathway For Improving Management of Mastitis and Breast AbscessEgy SeptiansyahNo ratings yet
- Folli Et Al 2012Document4 pagesFolli Et Al 2012Walid SasiNo ratings yet
- Radical Hysterectomy With Pelvic Lymphadenectomy - Indications TeDocument12 pagesRadical Hysterectomy With Pelvic Lymphadenectomy - Indications TexmatisaNo ratings yet
- Caprini Risk, 2022Document7 pagesCaprini Risk, 2022Tarek AbouzeidNo ratings yet
- Uterine Sarcima Tumor Board - Căutare GoogleDocument1 pageUterine Sarcima Tumor Board - Căutare GoogleCucu VeronicaNo ratings yet
- qt0b64c7mh NosplashDocument5 pagesqt0b64c7mh Nosplashdannafray.r1001No ratings yet
- Jurnal Bedah OnkologiDocument7 pagesJurnal Bedah OnkologiFieraNo ratings yet
- Birads Mammography: ExercisesDocument7 pagesBirads Mammography: ExercisesBetty Romero BarriosNo ratings yet
- Intraoperative Tests Rd100i Osna System and Metasin Test For Detecting Sentinel Lymph Node Metastases in Breast Cancer PDF 29279020741Document36 pagesIntraoperative Tests Rd100i Osna System and Metasin Test For Detecting Sentinel Lymph Node Metastases in Breast Cancer PDF 29279020741MariajanNo ratings yet
- Leiomioma - Miomectomia AbdominalDocument32 pagesLeiomioma - Miomectomia AbdominalNella SolanoNo ratings yet
- Perioperative Management For A Patient With Severe Congenital Factor V Deficiency Undergoing Cochlear ImplantationDocument3 pagesPerioperative Management For A Patient With Severe Congenital Factor V Deficiency Undergoing Cochlear ImplantationInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Benak Thesis For PublicationDocument24 pagesBenak Thesis For Publicationbenak shivalingappaNo ratings yet
- International Ovarian Tumour Analysis (IOTA) Phase 5Document22 pagesInternational Ovarian Tumour Analysis (IOTA) Phase 5RachnaNo ratings yet
- Global Cancer Facts and Figures 4th EditionDocument76 pagesGlobal Cancer Facts and Figures 4th EditionAfra AmiraNo ratings yet
- NATURE - Determinants of Obesity in Latin America (Ferreira Et Al., 2024)Document24 pagesNATURE - Determinants of Obesity in Latin America (Ferreira Et Al., 2024)LeonorNo ratings yet
- Research ArticleDocument9 pagesResearch ArticleJuliánPitalúaNo ratings yet
- 6th Refeerence FPDDocument12 pages6th Refeerence FPDSkAliHassanNo ratings yet
- Official Reprint From Uptodate ©2018 Uptodate, Inc. And/Or Its Affiliates. All Rights ReservedDocument53 pagesOfficial Reprint From Uptodate ©2018 Uptodate, Inc. And/Or Its Affiliates. All Rights ReservedKevin AdrianNo ratings yet
- 60 MustaphaDocument6 pages60 MustaphaMelody CyyNo ratings yet
- TrialsDocument7 pagesTrialsthweesha tanejaNo ratings yet
- Module 5&6 Statistics AnswerDocument10 pagesModule 5&6 Statistics AnswerElaine Canasta75% (4)
- Mammary Pathology: 1 Histology ReminderDocument17 pagesMammary Pathology: 1 Histology ReminderMonty IshikawaNo ratings yet
- Duker ClassificationDocument9 pagesDuker ClassificationfenestretoNo ratings yet
- Jurnal Deskriptif VICDocument14 pagesJurnal Deskriptif VICDarmayasa BagusNo ratings yet
- Manuskrip Jurnal Wina ISJNMSDocument11 pagesManuskrip Jurnal Wina ISJNMSWina OctavianaNo ratings yet
- Does Ovarian Cystectomy Pose A Risk To Ovarian Reserve and Fertility?Document10 pagesDoes Ovarian Cystectomy Pose A Risk To Ovarian Reserve and Fertility?Mohmd AboelkheirNo ratings yet
- Non-Melanoma Skin Cancer (NMSC) Is An Umbrella Term Which In1Document5 pagesNon-Melanoma Skin Cancer (NMSC) Is An Umbrella Term Which In1nuwanrajapakshaNo ratings yet
- 3D Printing Breast Tissue Models: A Review of Past Work and Directions For Future WorkDocument18 pages3D Printing Breast Tissue Models: A Review of Past Work and Directions For Future WorkRita DiabNo ratings yet
- IasjDocument7 pagesIasjismuNo ratings yet
- Treatment of Vitiligo by Narrow Band UVB Radiation Alone in Comparison To Combination of NB-UVB Plus Topical Vitiskin (Case, Therapeutic, Controlled Study)Document6 pagesTreatment of Vitiligo by Narrow Band UVB Radiation Alone in Comparison To Combination of NB-UVB Plus Topical Vitiskin (Case, Therapeutic, Controlled Study)IOSRjournalNo ratings yet
- Cholesteatoma SurgeryDocument4 pagesCholesteatoma SurgeryJad KafrouniNo ratings yet
- Myomectomy Without Myoma Extraction - 2021Document6 pagesMyomectomy Without Myoma Extraction - 2021sarafrota2016No ratings yet
- 10 Intraoperative RadiotherapyDocument11 pages10 Intraoperative RadiotherapyDgek LondonNo ratings yet
- Managing Common and Uncommon Complications of Aesthetic Breast SurgeryFrom EverandManaging Common and Uncommon Complications of Aesthetic Breast SurgeryJohn Y.S. KimNo ratings yet
- Pronostico en MamasDocument13 pagesPronostico en MamasDIOGENESNo ratings yet
- Celulas MesenquimalesDocument6 pagesCelulas MesenquimalesDIOGENESNo ratings yet
- Mama 4Document20 pagesMama 4DIOGENESNo ratings yet
- Injertos Viaje en La HistoriaDocument14 pagesInjertos Viaje en La HistoriaDIOGENESNo ratings yet
- The Impact of COVID-19 On Burn Care at A Major Regional Burn CenterDocument2 pagesThe Impact of COVID-19 On Burn Care at A Major Regional Burn CenterDIOGENESNo ratings yet
- Cancer de Lengua 2Document8 pagesCancer de Lengua 2DIOGENESNo ratings yet
- Five Methods of Breast Volume Measurement: A Comparative Study of Measurements of Specimen Volume in 30 Mastectomy CasesDocument10 pagesFive Methods of Breast Volume Measurement: A Comparative Study of Measurements of Specimen Volume in 30 Mastectomy CasesDIOGENESNo ratings yet
- The Submental Fat Compartment of The NeckDocument5 pagesThe Submental Fat Compartment of The NeckDIOGENESNo ratings yet
- Breast: Prediction of Resection Weight in Reduction Mammaplasty Based On Anthropometric MeasurementsDocument5 pagesBreast: Prediction of Resection Weight in Reduction Mammaplasty Based On Anthropometric MeasurementsDIOGENESNo ratings yet
- ''Flip-Over Flap'' in Two-Stage Cleft Palate RepairDocument6 pages''Flip-Over Flap'' in Two-Stage Cleft Palate RepairDIOGENESNo ratings yet
- Nanomedicina y Tecnologías Avanzadas para Quemaduras - Prevenir Infecciones y Facilitar La Curación de Heridas - ScienceDirectDocument103 pagesNanomedicina y Tecnologías Avanzadas para Quemaduras - Prevenir Infecciones y Facilitar La Curación de Heridas - ScienceDirectDIOGENESNo ratings yet
- Scar Management in Burn Injuries Using Drug Delivery and 2018 Advanced DrugDocument20 pagesScar Management in Burn Injuries Using Drug Delivery and 2018 Advanced DrugDIOGENESNo ratings yet
- Celulas MadresDocument10 pagesCelulas MadresDIOGENESNo ratings yet
- Bacterial and Viral ConjunctivitisDocument31 pagesBacterial and Viral ConjunctivitisSiddhant GautamNo ratings yet
- Cec Post Fall Assess and Man June 2013Document3 pagesCec Post Fall Assess and Man June 2013Vicente TurasNo ratings yet
- Jama Zhou 2023 It 230012 1694198870.80806Document2 pagesJama Zhou 2023 It 230012 1694198870.80806William TapiaNo ratings yet
- AdrenalinDocument8 pagesAdrenalinMisha Angela Isabel PerolNo ratings yet
- ArmeoPower HocomaDocument4 pagesArmeoPower HocomaralphholingsheadNo ratings yet
- CIcloyd Psychosis Peralta CuestaDocument10 pagesCIcloyd Psychosis Peralta CuestaJuan IgnacioNo ratings yet
- End of LifeDocument79 pagesEnd of LifeAbcd TolibasNo ratings yet
- 2surgical Nursing-Chronic Illness and Older AdultsDocument6 pages2surgical Nursing-Chronic Illness and Older AdultsGedie RocamoraNo ratings yet
- Anemia Testing Algorithm PDFDocument1 pageAnemia Testing Algorithm PDFkatNo ratings yet
- Neurological History TakingDocument3 pagesNeurological History TakingLANCE GILL TolentinoNo ratings yet
- Ccmanejoventilador y TerapiaadjuntaDocument11 pagesCcmanejoventilador y TerapiaadjuntaARELHI ROSARIO GARCIA MONROYNo ratings yet
- Case Presentation On Ruptured AppendicitisDocument83 pagesCase Presentation On Ruptured AppendicitisJoshuaNo ratings yet
- Dry Socket (Alveolar Osteitis) : Incidence, Pathogenesis, Prevention and ManagementDocument4 pagesDry Socket (Alveolar Osteitis) : Incidence, Pathogenesis, Prevention and ManagementPipin HeryantoNo ratings yet
- ctg نهائيDocument37 pagesctg نهائيdr.nahlla hellesNo ratings yet
- Case 1Document7 pagesCase 1secretNo ratings yet
- CLINICAL PLACEMENT PERMIT CHECKLIST Brock UniversityDocument2 pagesCLINICAL PLACEMENT PERMIT CHECKLIST Brock UniversityroldinpgNo ratings yet
- Animal BitesDocument48 pagesAnimal BitesJalouis GabalfinNo ratings yet
- Pros Tho Don Tic Considerations in Diabetes MellitusDocument16 pagesPros Tho Don Tic Considerations in Diabetes MellitusDrPrachi AgrawalNo ratings yet
- HTP Heat Related IllnessDocument7 pagesHTP Heat Related IllnessNhadzmae Asmadul IsnainNo ratings yet
- Kidney F Post TestDocument4 pagesKidney F Post TestMardie ArcesNo ratings yet
- Proposal of Rabies ProjectDocument3 pagesProposal of Rabies ProjectAngel Dario Morón FelizNo ratings yet
- Differential Diagnosis of The Scalp Hair FolliculitisDocument8 pagesDifferential Diagnosis of The Scalp Hair FolliculitisandreinaviconNo ratings yet