You might also like
- Primary CareDocument184 pagesPrimary Carehaneefmdf100% (1)
- Dermatology Class NotesDocument48 pagesDermatology Class Notesapi-26938624100% (6)
- Guava Soap For Investigatory ProjectDocument2 pagesGuava Soap For Investigatory ProjectfebyNo ratings yet
- Performing Facial TreatmentDocument48 pagesPerforming Facial TreatmentAngela Mae Gratija100% (1)
- PixleV User ManualDocument24 pagesPixleV User ManualVanja BossiNo ratings yet
- CAOP Exam Sample May 2020Document34 pagesCAOP Exam Sample May 2020BP155 -123 M. Taha KhanNo ratings yet
- European Ivd Market Report 2022Document9 pagesEuropean Ivd Market Report 2022Andreea G.100% (1)
- FINAL - Honey-Lemon-Based Facial Cleanser (FOR HARDBOUND)Document65 pagesFINAL - Honey-Lemon-Based Facial Cleanser (FOR HARDBOUND)JB TuganoNo ratings yet
- Tinywow Esa 2022 - Extension Slides 41022543-CompressedDocument36 pagesTinywow Esa 2022 - Extension Slides 41022543-Compressedapi-491110160No ratings yet
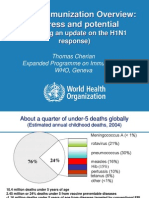
- Global Immunization Overview: Progress and PotentialDocument36 pagesGlobal Immunization Overview: Progress and PotentialPrabir Kumar ChatterjeeNo ratings yet
- Slid CH04Document48 pagesSlid CH04muneera aljaberiNo ratings yet
- Partner Abuse in England Wales Scotland Jan 10Document5 pagesPartner Abuse in England Wales Scotland Jan 10pete_RFFJNo ratings yet
- Services Brochure2015 eDocument8 pagesServices Brochure2015 eRumanaNo ratings yet
- Incidence and Treatment of Complications in PatientsDocument6 pagesIncidence and Treatment of Complications in Patientszfadhli.s.96No ratings yet
- Servicequalityof Canara BankDocument55 pagesServicequalityof Canara BankYuvraj LuhaniaNo ratings yet
- Servicequalityof Canara BankDocument55 pagesServicequalityof Canara BankGRAMY TRADERS SALEMNo ratings yet
- Data 13 QuestionsDocument17 pagesData 13 QuestionsEiksha SunejaNo ratings yet
- COVID-19 - Inmobi-Consumer Insights - India Part 2Document30 pagesCOVID-19 - Inmobi-Consumer Insights - India Part 2Avnish TripathiNo ratings yet
- Mamas 2Document6 pagesMamas 2DIOGENESNo ratings yet
- Teen Pregnancy 2Document1 pageTeen Pregnancy 2api-534751209No ratings yet
- Adjusted Dynamics of COVID-19 Pandemic Due To Herd Immunity in BangladeshDocument16 pagesAdjusted Dynamics of COVID-19 Pandemic Due To Herd Immunity in BangladeshNazmul IslamNo ratings yet
- Compilation of Past Years' MUETDocument38 pagesCompilation of Past Years' MUETnorasyrina90No ratings yet
- 11311-1087032 CavalloDocument43 pages11311-1087032 CavalloThanekaivel SNo ratings yet
- Trends in Telehealth: Alex Gerwer Principal Partner AKNDocument60 pagesTrends in Telehealth: Alex Gerwer Principal Partner AKNasg_akn8335No ratings yet
- xxx-ILC 4.2-024 Poster-Shahed Hossain Bangladesh-2 PDFDocument22 pagesxxx-ILC 4.2-024 Poster-Shahed Hossain Bangladesh-2 PDFRahen Rangan100% (1)
- Wagr 2020 RegistryDocument6 pagesWagr 2020 RegistryLuiziane SilvaNo ratings yet
- Goal: Clean AirDocument9 pagesGoal: Clean AirM-NCPPCNo ratings yet
- A Study On Customers Perception Towards House Loan: AbstractDocument6 pagesA Study On Customers Perception Towards House Loan: Abstractsenthilkumar SNo ratings yet
- Oral Final DefenseDocument44 pagesOral Final Defenserazel c. SorianoNo ratings yet
- FR Annex II Attractiveness Questionnaire Analysis PDFDocument80 pagesFR Annex II Attractiveness Questionnaire Analysis PDFKhin Nandar ThawNo ratings yet
- IJEDR2204013Document4 pagesIJEDR2204013pappuzbby2003No ratings yet
- Project Part 4Document4 pagesProject Part 4api-536264210No ratings yet
- Gig Report SummaryDocument8 pagesGig Report SummaryparidhiNo ratings yet
- Nursing Student's Anxiety About Career During The Pandemic Covid-19Document5 pagesNursing Student's Anxiety About Career During The Pandemic Covid-19Popi SopiahNo ratings yet
- Islp 4Document5 pagesIslp 4amithx100No ratings yet
- DAta Analysis and InterpretationDocument13 pagesDAta Analysis and Interpretationdeepikasaluja13No ratings yet
- Jefferis Et Al 2020 Final PaperDocument40 pagesJefferis Et Al 2020 Final PaperJose Antonio ChicurraneNo ratings yet
- Spain Demographics 2023 (Population, Age, Sex, Trends) - WorldometerDocument1 pageSpain Demographics 2023 (Population, Age, Sex, Trends) - WorldometerŞuc MihneaNo ratings yet
- BRM PDFDocument19 pagesBRM PDFShahebazNo ratings yet
- Live Project MarketingDocument17 pagesLive Project MarketingShambhunath PaulNo ratings yet
- Graphs Book For PrintingDocument112 pagesGraphs Book For PrintingHarshVavadiya67% (3)
- Goal: Smart Communities: Suggested RevisionDocument6 pagesGoal: Smart Communities: Suggested RevisionM-NCPPCNo ratings yet
- Assignment: Course Code: STA101 Section: 05 Instructor: Mohammad Mastak Al Amin (MMA)Document10 pagesAssignment: Course Code: STA101 Section: 05 Instructor: Mohammad Mastak Al Amin (MMA)i CrYNo ratings yet
- Deinstitutionalization Emilia SDocument27 pagesDeinstitutionalization Emilia SEmsNo ratings yet
- Formal Final ResutlDocument11 pagesFormal Final ResutlEngr Sardar Umer KhalidNo ratings yet
- Data Analysis and Interpretation: CH Apter IvDocument35 pagesData Analysis and Interpretation: CH Apter IvDeepak KumarNo ratings yet
- A Study On Customers' Satisfaction Towards: Lakmé Cosmetics at Ambegaon, PuneDocument25 pagesA Study On Customers' Satisfaction Towards: Lakmé Cosmetics at Ambegaon, PuneMome SinhaNo ratings yet
- Security of Ride SharingDocument22 pagesSecurity of Ride Sharingmd.jewel ranaNo ratings yet
- Exit Strategy of COVID-19 Epidemic in Sri LankaDocument17 pagesExit Strategy of COVID-19 Epidemic in Sri LankagazNo ratings yet
- Pandemic Flu Report, 2010Document22 pagesPandemic Flu Report, 2010haquera06No ratings yet
- 2011 HCMC Hotel Market Past Present and Future1Document28 pages2011 HCMC Hotel Market Past Present and Future1Tran BachNo ratings yet
- Assignment No 1: of Services MarketingDocument10 pagesAssignment No 1: of Services MarketingRohit SinghNo ratings yet
- Data VisualizationDocument39 pagesData Visualizationravi guptaNo ratings yet
- Work Force Planning For Public Power Utilities:: Ensuring Resources To Meet Projected NeedsDocument27 pagesWork Force Planning For Public Power Utilities:: Ensuring Resources To Meet Projected NeedsmtttusharNo ratings yet
- WHO English Summary GSRRS2018Document20 pagesWHO English Summary GSRRS2018sofiabloemNo ratings yet
- Arvind Eye Care Case StudyDocument48 pagesArvind Eye Care Case StudyNader NazihNo ratings yet
- The Economist Intelligence Unit - Online Retailing 2021Document11 pagesThe Economist Intelligence Unit - Online Retailing 2021Su ZhiNo ratings yet
- 2efim20034 2101425Document9 pages2efim20034 2101425jamietreasureNo ratings yet
- Screening For Breast CancerDocument20 pagesScreening For Breast CancerqalbiNo ratings yet
- Fair and Lovely AFFUDocument36 pagesFair and Lovely AFFUTheju ThejasreeNo ratings yet
- A Guideline To Belarusian Repressive Methods. Dealing With Structural Roots of Dissent - New Eastern EuropeDocument7 pagesA Guideline To Belarusian Repressive Methods. Dealing With Structural Roots of Dissent - New Eastern EuropeNunung KhairunnisahNo ratings yet
- PUBH151 Lab Exercises W3 Student'sDocument8 pagesPUBH151 Lab Exercises W3 Student'sAbdulqader DawoudNo ratings yet
- Main PaperDocument20 pagesMain PaperAnuPamGhOshNo ratings yet
- CHAPTER 4 First Page 14Document1 pageCHAPTER 4 First Page 14mhynaNo ratings yet
- ADB Client Perceptions Survey 2020: Multinational Survey of StakeholdersFrom EverandADB Client Perceptions Survey 2020: Multinational Survey of StakeholdersNo ratings yet
- Viet Nam Secondary Education Sector Assessment, Strategy, and Road MapFrom EverandViet Nam Secondary Education Sector Assessment, Strategy, and Road MapNo ratings yet
- Skabies Dermoskopi PedriatricDocument6 pagesSkabies Dermoskopi PedriatricRidho ForesNo ratings yet
- Acne Vulgaris 5Document3 pagesAcne Vulgaris 5Ridho ForesNo ratings yet
- Guideline KulitDocument38 pagesGuideline KulitRidho ForesNo ratings yet
- PruritusDocument11 pagesPruritusRidho ForesNo ratings yet
- Acne Urticata Associated With Chronic Myelogenous Leukemia: of Be of ofDocument4 pagesAcne Urticata Associated With Chronic Myelogenous Leukemia: of Be of ofGo McFlyNo ratings yet
- Medical Student Guide For Dermatology489Document89 pagesMedical Student Guide For Dermatology489Mojtaba Andalib AzarNo ratings yet
- Acne VulgarisDocument10 pagesAcne Vulgarisbrilian jelitaNo ratings yet
- New 4Document38 pagesNew 4rishi guptaNo ratings yet
- Pub 4Document4 pagesPub 4Faran MalikNo ratings yet
- Case Report Extended - Paradigm - of - Spectra - Dr-GlenDocument12 pagesCase Report Extended - Paradigm - of - Spectra - Dr-GlensristakNo ratings yet
- Using A Nonablative Monopolar Radiofrequency Laser in The Treatment of Acne VulgarisDocument5 pagesUsing A Nonablative Monopolar Radiofrequency Laser in The Treatment of Acne VulgarisGusraniNo ratings yet
- Quimical Peel and AcneDocument11 pagesQuimical Peel and AcneigorfragaNo ratings yet
- Soal Bahasa InggrisDocument9 pagesSoal Bahasa InggrisViona CansNo ratings yet
- MN552 UNIT 10 LAB 3 Childhood ObesityDocument3 pagesMN552 UNIT 10 LAB 3 Childhood ObesityHugsNo ratings yet
- Perioral Dermatitis: Acta Dermatovenerologica Croatica: ADC / Hrvatsko Dermatolosko Drustvo February 2008Document6 pagesPerioral Dermatitis: Acta Dermatovenerologica Croatica: ADC / Hrvatsko Dermatolosko Drustvo February 2008Firdani MutiaraNo ratings yet
- SMK 01Document12 pagesSMK 01FathiyaNo ratings yet
- Pricelist SKINTIFIC Jakarta X Beauty II 14 - 17 Dec 2023Document1 pagePricelist SKINTIFIC Jakarta X Beauty II 14 - 17 Dec 2023ZakiyahNo ratings yet
- Vitabrid Company Intro ENG 180119Document41 pagesVitabrid Company Intro ENG 180119Kate NguyenNo ratings yet
- Treatment of Acne With A Combination of Propolis, Tea Tree Oil, and Aloe Vera Compared To Erythromycin Cream: Two Double-Blind InvestigationsDocument7 pagesTreatment of Acne With A Combination of Propolis, Tea Tree Oil, and Aloe Vera Compared To Erythromycin Cream: Two Double-Blind InvestigationsFajar RamadhanNo ratings yet
- Acne Vulgaris New Evidence in Pathogenesis and Future Modalities of TreatmentDocument11 pagesAcne Vulgaris New Evidence in Pathogenesis and Future Modalities of TreatmentyelsiNo ratings yet
- A New Dimension in Ensuring Safety of Laser and Light Based Devices in Dermatological Practice Materiovigilance ProgrammeDocument5 pagesA New Dimension in Ensuring Safety of Laser and Light Based Devices in Dermatological Practice Materiovigilance ProgrammeAthenaeum Scientific PublishersNo ratings yet
- Acne Treatment - Benzoyl PeroxideDocument2 pagesAcne Treatment - Benzoyl PeroxideudinNo ratings yet
- Cosmetics 10 00014 v2Document15 pagesCosmetics 10 00014 v2waode hasryaniNo ratings yet
- For Research PapersDocument2 pagesFor Research PapersLuna Lux CastielloNo ratings yet
- Microbiological Perspective of Common Skin Rashes: A Seminar Presentation BY Oluwamuyiwa Boluwatife Yinka (HSLT-20-0109)Document12 pagesMicrobiological Perspective of Common Skin Rashes: A Seminar Presentation BY Oluwamuyiwa Boluwatife Yinka (HSLT-20-0109)Olayimika OluwanifemiNo ratings yet
- Sub Micron Cosmeceuticals in Drug DeliveryDocument24 pagesSub Micron Cosmeceuticals in Drug DeliverySuraj Vasista67% (6)
- Skin, Hair & Nails Supplement Guide - Examine - 2020 - Examine - Anna's ArchiveDocument75 pagesSkin, Hair & Nails Supplement Guide - Examine - 2020 - Examine - Anna's Archivesimondon11No ratings yet