You might also like
- Article 8 Mohamed Yousef 2 PDFDocument6 pagesArticle 8 Mohamed Yousef 2 PDFfikih mahgfirohNo ratings yet
- Patient Doses in General Radiography Examinations: Peer Reviewed ORIGINAL ARTICLEDocument5 pagesPatient Doses in General Radiography Examinations: Peer Reviewed ORIGINAL ARTICLEModestus OgbukaNo ratings yet
- Applsci 11 09749 v2Document10 pagesApplsci 11 09749 v2Angelina ProtikNo ratings yet
- Digital Radiography RejectDocument8 pagesDigital Radiography RejectRama EdelianoorNo ratings yet
- Quality Control of Diagnostic RadiologyDocument7 pagesQuality Control of Diagnostic RadiologySehad KadiriNo ratings yet
- Analysis of Repeat Radiography and Corrective Measures in Teaching Hospital in Tertiary Health Care CentreDocument4 pagesAnalysis of Repeat Radiography and Corrective Measures in Teaching Hospital in Tertiary Health Care CentreIJAR JOURNALNo ratings yet
- RPT 29Document79 pagesRPT 29Vidya NaikNo ratings yet
- Oral and Maxillofacial Radiology: Oral Surgery Oral Medicine Oral PathologyDocument6 pagesOral and Maxillofacial Radiology: Oral Surgery Oral Medicine Oral PathologynisaNo ratings yet
- Paper 24 RPD Ubeda 2015Document4 pagesPaper 24 RPD Ubeda 2015CARLOS ARTURO UBEDA DE LA CERDANo ratings yet
- Qa AssuranceDocument6 pagesQa AssuranceSari BustillosNo ratings yet
- Implementation of a Remote and Automated Quality Control Programme for Radiography and Mammography EquipmentFrom EverandImplementation of a Remote and Automated Quality Control Programme for Radiography and Mammography EquipmentNo ratings yet
- 8179 USRadiation Safety BrochureDocument10 pages8179 USRadiation Safety BrochureAngelina ProtikNo ratings yet
- Biij 03 E18Document15 pagesBiij 03 E18Lalit GahlotNo ratings yet
- Assessment of Image Quality of Plain Abdominal Radiographs at A Northwestern Nigeria Tertiary HospitalDocument7 pagesAssessment of Image Quality of Plain Abdominal Radiographs at A Northwestern Nigeria Tertiary HospitalmusdalifahNo ratings yet
- Technical Report, 1997Document21 pagesTechnical Report, 1997samsonNo ratings yet
- X Ray Tubes Quality Control in The Optimization of Doses To Patients and Personnel in Conventional RadiologyDocument6 pagesX Ray Tubes Quality Control in The Optimization of Doses To Patients and Personnel in Conventional RadiologypouchkineNo ratings yet
- Evaluation of Reject Analysis of Chest Radiographs in Diagnostic RadiologyDocument5 pagesEvaluation of Reject Analysis of Chest Radiographs in Diagnostic RadiologySiti MutyaNo ratings yet
- AbdoDocument6 pagesAbdosaifulmangopo123No ratings yet
- Digital Intraoral Radiographic Quality AssuranceDocument8 pagesDigital Intraoral Radiographic Quality AssuranceAmelia Rizky HutamiNo ratings yet
- Assesment of Entrance Skin Doses For Patients - Abdullah Medical CityDocument4 pagesAssesment of Entrance Skin Doses For Patients - Abdullah Medical CityGeorgiana KokonaNo ratings yet
- Qaqc Midterm ReviewerDocument4 pagesQaqc Midterm ReviewerCherie lou PizaNo ratings yet
- Fulltext 6Document4 pagesFulltext 6Muhammad Abdul RahmanNo ratings yet
- Biij2007 Vol3 Issue2 Article6 JournalDocument14 pagesBiij2007 Vol3 Issue2 Article6 JournalpritikachandNo ratings yet
- Computers in Radiology: Technologists' Productivity When Using PACSDocument5 pagesComputers in Radiology: Technologists' Productivity When Using PACSBayu Rahmat PerdanaNo ratings yet
- A Novel Risk Analysis of Clinical Reference Dosimetry Based On Failure Modes and Effects AnalysisDocument7 pagesA Novel Risk Analysis of Clinical Reference Dosimetry Based On Failure Modes and Effects AnalysisMichelle LEINo ratings yet
- Quality Control of Gamma Camera With SPECT SystemsDocument8 pagesQuality Control of Gamma Camera With SPECT SystemsMSNo ratings yet
- Final PaperDocument5 pagesFinal PaperEdwin LimlengcoNo ratings yet
- Clinical Efficacy of An Electronic Portal Imaging Device Versus A Physical PhantomDocument12 pagesClinical Efficacy of An Electronic Portal Imaging Device Versus A Physical Phantomxiwevi4103No ratings yet
- MR Artifacts Safety and Quality Control AAPMRSNADocument25 pagesMR Artifacts Safety and Quality Control AAPMRSNAjerry22445550No ratings yet
- Quality Control in Dental Radiology in Serbia: Preliminary ResultsDocument4 pagesQuality Control in Dental Radiology in Serbia: Preliminary ResultsZoran MirkovNo ratings yet
- Jurnal KumarDocument4 pagesJurnal Kumaranindya permatasyafiraNo ratings yet
- 163 FullDocument3 pages163 FullVola FaurisNo ratings yet
- Name:: 1. Ahmad Ardi Pratama 2. Muhammad Eri HDocument11 pagesName:: 1. Ahmad Ardi Pratama 2. Muhammad Eri HAhmad Ardi PratamaNo ratings yet
- Gislason-Lee Et Al 2014 ADRC ECR EposterDocument12 pagesGislason-Lee Et Al 2014 ADRC ECR EposterAnders ErikssonNo ratings yet
- Mahesh 2013Document2 pagesMahesh 2013mestajibehinnegarehNo ratings yet
- Zacharaki - A Digital SubtractionDocument14 pagesZacharaki - A Digital Subtractiondorasani99No ratings yet
- Jurnal Radiologi DasarDocument4 pagesJurnal Radiologi DasarPresty Dwi FitrianiNo ratings yet
- Article1386848180 - Oluwafisoye Et AlDocument5 pagesArticle1386848180 - Oluwafisoye Et AlJojo KawayNo ratings yet
- MJMHS 1004Document8 pagesMJMHS 1004Ayu RositaNo ratings yet
- Akarslan2008 PDFDocument6 pagesAkarslan2008 PDFLaura ImreNo ratings yet
- A Paediatric X-Ray Exposure ChartDocument11 pagesA Paediatric X-Ray Exposure ChartMarco Jimenez HerreraNo ratings yet
- A Paediatric X-Ray Exposure ChartDocument11 pagesA Paediatric X-Ray Exposure Chartdddemourita9249No ratings yet
- Dr. Ebtisam Elhamalawy: MFDS RSC (Edh.), MJDF RSC (Lon.), BDS (Misr International University)Document83 pagesDr. Ebtisam Elhamalawy: MFDS RSC (Edh.), MJDF RSC (Lon.), BDS (Misr International University)Mustafa H. KadhimNo ratings yet
- Biij 06 E5Document6 pagesBiij 06 E5DetonadorJVCNo ratings yet
- The National Academies Press: Airport Passenger Screening Using Backscatter X-Ray Machines: Compliance With StandardsDocument31 pagesThe National Academies Press: Airport Passenger Screening Using Backscatter X-Ray Machines: Compliance With StandardsKaruppasamy PandianNo ratings yet
- X-Ray Special Investigations Rebook Analysis (XSIRA)Document5 pagesX-Ray Special Investigations Rebook Analysis (XSIRA)IOSRjournal100% (1)
- LED-Based Photoacoustic Imaging: From Bench to BedsideFrom EverandLED-Based Photoacoustic Imaging: From Bench to BedsideMithun Kuniyil Ajith SinghNo ratings yet
- ESR 2014 Renewal of Radiological EquipmentDocument4 pagesESR 2014 Renewal of Radiological EquipmentShirley SpenceNo ratings yet
- Quality Management Systems in Radiology: Original ArticleDocument5 pagesQuality Management Systems in Radiology: Original ArticlebekoNo ratings yet
- Radiation Exposure Optimization During Cryobaloon AblationDocument8 pagesRadiation Exposure Optimization During Cryobaloon AblationfofikoNo ratings yet
- The in Uence of Different Technique Factors On Image Quality of Lumbar Spine Radiographs As Evaluated by Established CEC Image CriteriaDocument16 pagesThe in Uence of Different Technique Factors On Image Quality of Lumbar Spine Radiographs As Evaluated by Established CEC Image Criteriaiftitah nailaNo ratings yet
- 2F 5 Radiation Risk AssessmentDocument4 pages2F 5 Radiation Risk AssessmentNurul SyaheerahNo ratings yet
- KistaDocument7 pagesKistaIceu EstuNo ratings yet
- Quality of Periapical Radiographs Taken by Undergraduate Students During Endodontic TreatmentDocument8 pagesQuality of Periapical Radiographs Taken by Undergraduate Students During Endodontic Treatmentbertha t rumsiNo ratings yet
- NHSBSP Equipment Report 0802Document28 pagesNHSBSP Equipment Report 0802vitapabloNo ratings yet
- Rajiv Gandhi University of Health Sciences, Karnataka, BangaloreDocument9 pagesRajiv Gandhi University of Health Sciences, Karnataka, BangaloreAhmed Febri Hertama 'Sinosuke'No ratings yet
- Radiation Dose in Paediatric Interventional ProcedureDocument5 pagesRadiation Dose in Paediatric Interventional Proceduresebastian CarrascoNo ratings yet
- RTFI Course Material PDFDocument133 pagesRTFI Course Material PDFerlon0rodrigues100% (1)
- RTFI Course MaterialDocument133 pagesRTFI Course MaterialDIPPOSNo ratings yet
- ALARA Jadi ALADIPDocument8 pagesALARA Jadi ALADIPalphaniaNo ratings yet
- Stuttering: NIDCD Fact Sheet - Voice, Speech, and LanguageDocument4 pagesStuttering: NIDCD Fact Sheet - Voice, Speech, and LanguageAde Afriza FeraniNo ratings yet
- NCM 116 Medical Surgical ReviewerDocument18 pagesNCM 116 Medical Surgical ReviewerClark Evan PillonarNo ratings yet
- Handbook of RadioembolizationDocument349 pagesHandbook of RadioembolizationEdu MassanaNo ratings yet
- Syngo WARP Metal Artifact Reduction Techniques in MRI 1800000000284426Document2 pagesSyngo WARP Metal Artifact Reduction Techniques in MRI 1800000000284426MELANITH BRAVONo ratings yet
- AI in Cardiovascular DiseaseDocument11 pagesAI in Cardiovascular Diseasepartha sreekarNo ratings yet
- The Contribution History Impact and Future of Physics in MedicineDocument10 pagesThe Contribution History Impact and Future of Physics in MedicineprashantNo ratings yet
- DR Detector Calibration: Key User ManualDocument37 pagesDR Detector Calibration: Key User ManualAku TonyNo ratings yet
- ACTIVITY On Neuro AssessmentDocument25 pagesACTIVITY On Neuro AssessmentGuillana Mae CastellonNo ratings yet
- Clinical Manifestations, Diagnosis, and Prognosis of Crohn Disease in Adults - UpToDateDocument45 pagesClinical Manifestations, Diagnosis, and Prognosis of Crohn Disease in Adults - UpToDateAsclepioNo ratings yet
- BrochureA SERENYS Series 02-CompressedDocument4 pagesBrochureA SERENYS Series 02-CompressedVictor ParedesNo ratings yet
- SIMIND Monte Carlo Simulation of A Single Photon Emission CTDocument8 pagesSIMIND Monte Carlo Simulation of A Single Photon Emission CTMariana CarvalhoNo ratings yet
- PG Ece - 03112017Document55 pagesPG Ece - 03112017Himanshu SinghNo ratings yet
- Prostate Cancer Literature ReviewDocument5 pagesProstate Cancer Literature Reviewea6z9033100% (1)
- Susceptibility of MNCL2Document23 pagesSusceptibility of MNCL2AshwamedhNo ratings yet
- Medical School EssaysDocument3 pagesMedical School EssaysGerardien Elham Afifah33% (3)
- Ian R. McClelland X-Ray Equipment Maintenance and Repairs Workbook For Radiographers and Radiological TechnologistsDocument272 pagesIan R. McClelland X-Ray Equipment Maintenance and Repairs Workbook For Radiographers and Radiological Technologistssavannah78No ratings yet
- 1452pdf PDFDocument5 pages1452pdf PDFOgut AjaNo ratings yet
- Diagnostic ImagingDocument2 pagesDiagnostic ImagingNatalia RamírezNo ratings yet
- Mindray: Expanding The Envelope of Performance and FlexibilityDocument8 pagesMindray: Expanding The Envelope of Performance and FlexibilityLeeNo ratings yet
- Pain Neuroscience EducationDocument26 pagesPain Neuroscience EducationGustavo Cabanas100% (1)
- Non-Invasive Cardiovascular ImagingDocument760 pagesNon-Invasive Cardiovascular ImagingOrlin ZlatarskiNo ratings yet
- Philips Allura Xper FD20 Functional DescriptionDocument40 pagesPhilips Allura Xper FD20 Functional DescriptionHugo TranNo ratings yet
- Mri SequencesDocument13 pagesMri SequencesNorma RamirezNo ratings yet
- CT MRI Field Service EngineerDocument3 pagesCT MRI Field Service Engineerapi-78089992No ratings yet
- P Reddy SAJS 2017Document6 pagesP Reddy SAJS 2017Sumayyah EbrahimNo ratings yet
- LMTDocument6 pagesLMTMostafa AdamNo ratings yet
- Syllabus BMIDocument3 pagesSyllabus BMIMathavaraja JeyaramanNo ratings yet
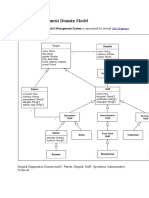
- Hospital Management Domain ModelDocument4 pagesHospital Management Domain Modelvinod kapateNo ratings yet
- 7 Spesifikasi USG Acuson S1000 USG Obgyn 4D UltraPremium W 3 Probes FINAL PDFDocument95 pages7 Spesifikasi USG Acuson S1000 USG Obgyn 4D UltraPremium W 3 Probes FINAL PDFipungNo ratings yet