You might also like
- Mental Status Examination FormatDocument7 pagesMental Status Examination FormatMala Rasaily100% (3)
- ISO 13485 Version 2016 Requirements NotesDocument24 pagesISO 13485 Version 2016 Requirements Notesda_reaper_dasNo ratings yet
- CABG Case Study ReportDocument83 pagesCABG Case Study ReportSherena NicolasNo ratings yet
- The Neuroscience of Autism Spectrum DisordersDocument10 pagesThe Neuroscience of Autism Spectrum DisorderssouciNo ratings yet
- Advanced Endovascular Therapy of Aortic DiseaseFrom EverandAdvanced Endovascular Therapy of Aortic DiseaseAlan B. LumsdenNo ratings yet
- 29 Full PDFDocument7 pages29 Full PDFDHIVYANo ratings yet
- Cardiac Stab WoundDocument7 pagesCardiac Stab WoundYogi Permana AgustaNo ratings yet
- Omar 2014Document5 pagesOmar 2014Fede WeckesserNo ratings yet
- Coronary Angiographic Morphology in Myocardial Infarction: A Link Between The Pathogenesis of Unstable Angina and Myocardial InfarctionDocument6 pagesCoronary Angiographic Morphology in Myocardial Infarction: A Link Between The Pathogenesis of Unstable Angina and Myocardial InfarctionSabila RosyidaNo ratings yet
- De Neuville 2000Document5 pagesDe Neuville 2000Anonymous WPiPld6npNo ratings yet
- 1 s2.0 S2210261223011938 MainDocument3 pages1 s2.0 S2210261223011938 Mainkalebberhane9No ratings yet
- Sudden Hypotension Occurring After 4 Days of Left-Sided Central Catheter PlacementDocument3 pagesSudden Hypotension Occurring After 4 Days of Left-Sided Central Catheter PlacementFaqih SultonfaqNo ratings yet
- Coronary Stent Infections A Case of Pericardial Abscess and Stent Displacement After Repeated PTCA Procedures Which Required An Emergency SurgeryDocument4 pagesCoronary Stent Infections A Case of Pericardial Abscess and Stent Displacement After Repeated PTCA Procedures Which Required An Emergency SurgeryAthenaeum Scientific PublishersNo ratings yet
- Circulation 1975 Burggraf 146 56Document12 pagesCirculation 1975 Burggraf 146 56Zikri Putra Lan LubisNo ratings yet
- Pericardiectomy For Tuberculous Effusive-Constrictive PericarditisDocument5 pagesPericardiectomy For Tuberculous Effusive-Constrictive PericarditisIJAR JOURNALNo ratings yet
- Case Report: Transmediastinal and Transcardiac Gunshot Wound With Hemodynamic StabilityDocument4 pagesCase Report: Transmediastinal and Transcardiac Gunshot Wound With Hemodynamic StabilityAmriansyah PranowoNo ratings yet
- Indikasi Torakotomi Chest TraumaDocument6 pagesIndikasi Torakotomi Chest TraumaanglingNo ratings yet
- Griffith 1996Document10 pagesGriffith 1996Sowmya ANo ratings yet
- Atrial Hemangioma A Case Report and Review of The LiteratureDocument11 pagesAtrial Hemangioma A Case Report and Review of The LiteratureSaya MenarikNo ratings yet
- Ali TransechoDocument2 pagesAli TransechoUtama Hadiputra SurbaktiNo ratings yet
- Paracardiac Masses Caused A Right Coronary Artery Aneurysm and A Saphenous Vein Graft AneurysmDocument3 pagesParacardiac Masses Caused A Right Coronary Artery Aneurysm and A Saphenous Vein Graft AneurysmSheikh Mizanur RahmanNo ratings yet
- Traumatic Rupture Aortic DX TXDocument6 pagesTraumatic Rupture Aortic DX TXprisselya anisaNo ratings yet
- Pi Is 0003497500014818Document7 pagesPi Is 0003497500014818GKNo ratings yet
- Clinical Clues To The Causes of Large Pericardial EffusionsDocument7 pagesClinical Clues To The Causes of Large Pericardial EffusionsDewinsNo ratings yet
- Management of Neoplastic Pericardial EffusionsDocument4 pagesManagement of Neoplastic Pericardial EffusionsMamamia DonchanNo ratings yet
- Transcatheter Coil Embolotherapy: A Safe and Evective Option For Major Colonic HaemorrhageDocument7 pagesTranscatheter Coil Embolotherapy: A Safe and Evective Option For Major Colonic Haemorrhagemuhammad gagas sasongkoNo ratings yet
- Left Hemothorax: Unusual Manifestation of Aortic DissectionDocument5 pagesLeft Hemothorax: Unusual Manifestation of Aortic DissectionIJAR JOURNALNo ratings yet
- Cardiac Autotransplantation: Cooley Society 15th International SymposiumDocument5 pagesCardiac Autotransplantation: Cooley Society 15th International SymposiumPeter Paul PascualNo ratings yet
- 30143-Article Text-56534-1-10-20220323Document5 pages30143-Article Text-56534-1-10-20220323Octavia SohanggrainyNo ratings yet
- Diagnosis and Treatment of Pericallosal Artery Aneurysms: SciencedirectDocument4 pagesDiagnosis and Treatment of Pericallosal Artery Aneurysms: SciencedirectRais RyuzakiNo ratings yet
- Haemodialysis Access by Inferior Vena Cava Catheterisation: Cientific EttersDocument7 pagesHaemodialysis Access by Inferior Vena Cava Catheterisation: Cientific EttersmochkurniawanNo ratings yet
- The Use of A Vascular Patch CorMatrix ECM® For Reconstruction of Carotid Arteries in The Treatment of Postoperative Wound InfectionDocument3 pagesThe Use of A Vascular Patch CorMatrix ECM® For Reconstruction of Carotid Arteries in The Treatment of Postoperative Wound InfectionMircea Eugen MutuNo ratings yet
- 45 1057Document5 pages45 1057Gabriela PinticanNo ratings yet
- Spontaneous HaemopneumothoraxDocument2 pagesSpontaneous HaemopneumothoraxAshok PanjwaniNo ratings yet
- 2011 Early Cannulation Grafts in Straight Axillo Axillary AngioaccessesDocument4 pages2011 Early Cannulation Grafts in Straight Axillo Axillary AngioaccessesKindylight KindylightNo ratings yet
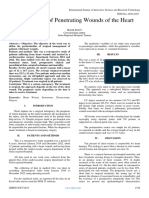
- Management of Penetrating Wounds of The HeartDocument2 pagesManagement of Penetrating Wounds of The HeartInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Intrinsic Third Ventricular Craniopharyngiomas: Report On Six Cases and A Review of The LiteratureDocument8 pagesIntrinsic Third Ventricular Craniopharyngiomas: Report On Six Cases and A Review of The LiteratureAmina GoharyNo ratings yet
- Word 1663843244389Document11 pagesWord 1663843244389Atik PurwandariNo ratings yet
- Acosta 2003Document5 pagesAcosta 2003Mihaela MocanNo ratings yet
- Angiosarcoma of SVCDocument4 pagesAngiosarcoma of SVCDevi MNo ratings yet
- Accidente Cerebrovascular Isquémico en Pacientes Con Trombo Intracavitario: Experiencia Con Tratamientos Distintos en Fase AgudaDocument5 pagesAccidente Cerebrovascular Isquémico en Pacientes Con Trombo Intracavitario: Experiencia Con Tratamientos Distintos en Fase AgudaDENNISSENo ratings yet
- Catete RDocument3 pagesCatete ROdalis AltamiranoNo ratings yet
- Cric2018 7237454Document4 pagesCric2018 7237454Muhammad Nur Ardhi LahabuNo ratings yet
- Spontaneous Vertebral Artery Dissection: Report of 16 Cases: Original ArticleDocument7 pagesSpontaneous Vertebral Artery Dissection: Report of 16 Cases: Original ArticleAyu Yoniko CimplukNo ratings yet
- Obstructed Pulmonary Venous Drainage Common in TAPVC to Coronary SinusDocument5 pagesObstructed Pulmonary Venous Drainage Common in TAPVC to Coronary Sinuswiyay34652ceoshubcomNo ratings yet
- JOURNALDocument4 pagesJOURNALChiara FajardoNo ratings yet
- Cardiac Tamponade A Rare Complication of Nissen FundoplicationDocument3 pagesCardiac Tamponade A Rare Complication of Nissen FundoplicationDaniel PredaNo ratings yet
- American Journal of Emergency Medicine - cardiac tamponadeDocument3 pagesAmerican Journal of Emergency Medicine - cardiac tamponadefloNo ratings yet
- 2000 - Stamm Et Al. - Surgery For Bilateral Outflow Tract Obstruction in Elastin ArteriopathyDocument9 pages2000 - Stamm Et Al. - Surgery For Bilateral Outflow Tract Obstruction in Elastin ArteriopathybanupluNo ratings yet
- Disseccao Tipo b2Document6 pagesDisseccao Tipo b2coopervascba.diradmNo ratings yet
- CLC 4960151208Document7 pagesCLC 4960151208DoraNo ratings yet
- Transhepatic Access: Alternative Approach For Right Heart Catheterization and Pulmonary AngiographyDocument3 pagesTranshepatic Access: Alternative Approach For Right Heart Catheterization and Pulmonary AngiographyDavids MarinNo ratings yet
- Ekim, H. y Tuncer, M. (2009) - Manejo de Lesiones Traumáticas de La Arteria Braquial Informe de 49 PacientesDocument5 pagesEkim, H. y Tuncer, M. (2009) - Manejo de Lesiones Traumáticas de La Arteria Braquial Informe de 49 PacientesEdgar Geovanny Cardenas FigueroaNo ratings yet
- Percutaneous Coronary Intervention in A Patient With Severe Systemic Vasculitis and Myocardial InfarctionDocument4 pagesPercutaneous Coronary Intervention in A Patient With Severe Systemic Vasculitis and Myocardial Infarctionvam buddhaNo ratings yet
- Eriksen Et Al-2002-Clinical Cardiology PDFDocument5 pagesEriksen Et Al-2002-Clinical Cardiology PDFmedskyqqNo ratings yet
- 62 2020 Article 898Document7 pages62 2020 Article 898sinamirjaniNo ratings yet
- Aranda 1998Document5 pagesAranda 1998Sarly FebrianaNo ratings yet
- Acs 03 03 234Document13 pagesAcs 03 03 234IwanNo ratings yet
- Mitral Valve Endocarditis in Hypertrophic Cardiomyopathy: Case Report and Literature ReviewDocument3 pagesMitral Valve Endocarditis in Hypertrophic Cardiomyopathy: Case Report and Literature ReviewChristabella Natalia WijayaNo ratings yet
- Perioperative Management of AdrenalectomyDocument13 pagesPerioperative Management of AdrenalectomyTJ LapuzNo ratings yet
- A Case Series of Intracardiac Thrombosis Revealing Behcets Disease in Moroccan PatientsDocument4 pagesA Case Series of Intracardiac Thrombosis Revealing Behcets Disease in Moroccan PatientsIJAR JOURNALNo ratings yet
- AcNch05-The Risk of Rebleeding After External Lumbar Drainage in Patients With Untreated RupturedDocument6 pagesAcNch05-The Risk of Rebleeding After External Lumbar Drainage in Patients With Untreated RupturedWaldemar PiñaNo ratings yet
- Pulmonary Endarterectomy: Experience and Lessons Learned in 1,500 CasesDocument8 pagesPulmonary Endarterectomy: Experience and Lessons Learned in 1,500 CasesRoxana Maria MunteanuNo ratings yet
- Jamainternal Kim 2019 Oi 180114Document9 pagesJamainternal Kim 2019 Oi 180114api-541676441No ratings yet
- Jamainternal Kim 2019 Oi 180114Document9 pagesJamainternal Kim 2019 Oi 180114api-541676441No ratings yet
- ExtracorporealDocument1 pageExtracorporealapi-541676441No ratings yet
- Guidelines Revasc FT PDFDocument55 pagesGuidelines Revasc FT PDFAlina TomaNo ratings yet
- Vascular SubstitutesDocument1 pageVascular Substitutesapi-541676441No ratings yet
- Comparativo Valvullas 1Document2 pagesComparativo Valvullas 1api-541676441No ratings yet
- Catalogo Cardio Sharol 1Document11 pagesCatalogo Cardio Sharol 1api-541676441No ratings yet
- Polimeros Sharol 1Document1 pagePolimeros Sharol 1api-541676441No ratings yet
- Cotizacion de Instrumental de CardioDocument4 pagesCotizacion de Instrumental de Cardioapi-541676441No ratings yet
- Farmacologia CardiacaDocument2 pagesFarmacologia Cardiacaapi-541676441No ratings yet
- Inmobiliario de Un Quirofano 1Document2 pagesInmobiliario de Un Quirofano 1api-541676441No ratings yet
- Catalogo Cardio Sharol 1Document11 pagesCatalogo Cardio Sharol 1api-541676441No ratings yet
- Sistema de ConduccionDocument3 pagesSistema de Conduccionapi-541676441No ratings yet
- Diagrama en Blanco 2 1Document1 pageDiagrama en Blanco 2 1api-541676441No ratings yet
- Embryonic DevelopmentDocument9 pagesEmbryonic Developmentapi-541676441No ratings yet
- Boston Globe Article - Jonnie Williams & Frank O'DonnellDocument3 pagesBoston Globe Article - Jonnie Williams & Frank O'DonnellFuzzy PandaNo ratings yet
- Samruddhi ComplexDocument7 pagesSamruddhi ComplexNews Side Effects.No ratings yet
- Berkowitz Et Al (2010) - Skills For Psychological Recovery - Field Operations GuideDocument154 pagesBerkowitz Et Al (2010) - Skills For Psychological Recovery - Field Operations GuideRita CamiloNo ratings yet
- 1 Catalyst FundamentalsDocument17 pages1 Catalyst FundamentalsSam AnuNo ratings yet
- GeM Bidding 3702669Document10 pagesGeM Bidding 3702669ANIMESH JAINNo ratings yet
- Edited SCHOOL IN SERVICE TRAINING FOR TEACHERS MID YEAR 2023Document11 pagesEdited SCHOOL IN SERVICE TRAINING FOR TEACHERS MID YEAR 2023Lordennisa MacawileNo ratings yet
- COVID-19 and Flu Vaccination Walgreens Immunization ServicesDocument1 pageCOVID-19 and Flu Vaccination Walgreens Immunization ServicesAitana MaldonadoNo ratings yet
- XII Class Assignment Programs 2023-24Document8 pagesXII Class Assignment Programs 2023-24Sudhir KumarNo ratings yet
- Sony STR Da80esDocument66 pagesSony STR Da80estelstarservicesNo ratings yet
- New Translation and Deciphering of ChineDocument14 pagesNew Translation and Deciphering of ChineRémyNo ratings yet
- SD Series Digital AC Servo System User Manual GuideDocument66 pagesSD Series Digital AC Servo System User Manual GuideAdnene SaanounNo ratings yet
- GRP 10 JV'sDocument43 pagesGRP 10 JV'sManas ChaturvediNo ratings yet
- Manjit Thapp ResearchDocument24 pagesManjit Thapp ResearchDough RodasNo ratings yet
- Allison WallaceDocument3 pagesAllison WallaceOskar KarvajalNo ratings yet
- Method Overloading in JavaDocument6 pagesMethod Overloading in JavaPrerna GourNo ratings yet
- University of Cambridge International Examinations General Certificate of Education Ordinary LevelDocument12 pagesUniversity of Cambridge International Examinations General Certificate of Education Ordinary Levelmstudy123456No ratings yet
- What Is Mean?: Extrapolation InterpolationDocument2 pagesWhat Is Mean?: Extrapolation InterpolationVinod SharmaNo ratings yet
- Strawberry GenerationDocument2 pagesStrawberry GenerationImat12No ratings yet
- F 83179Document6 pagesF 83179pcmfilhoNo ratings yet
- Nursing Care Plans for ChildrenDocument4 pagesNursing Care Plans for ChildrenAlexander Rodriguez OlipasNo ratings yet
- 5 Tips For Faster Mental Multiplication PDFDocument3 pages5 Tips For Faster Mental Multiplication PDFGonzalo Estrán BuyoNo ratings yet
- Chapter (3) Simple Stresses in Machine Parts: Design of Machine Elements I (ME-41031)Document80 pagesChapter (3) Simple Stresses in Machine Parts: Design of Machine Elements I (ME-41031)Dr. Aung Ko LattNo ratings yet
- Titan InvoiceDocument1 pageTitan Invoiceiamdhanush017No ratings yet
- Accounting For Non Specialists Australian 7th Edition Atrill Test BankDocument26 pagesAccounting For Non Specialists Australian 7th Edition Atrill Test BankJessicaMitchelleokj100% (49)
- Islamic Center Design With Islamic ArchiDocument11 pagesIslamic Center Design With Islamic ArchiMuhammad Sufiyan SharafudeenNo ratings yet
- ORPHEUS by GRS Mead - Electronic Text EditionDocument199 pagesORPHEUS by GRS Mead - Electronic Text EditionMartin EuserNo ratings yet
- St. Augustine School of Nursing: Republic of The Philippines Department of Education SASN - Las PiñasDocument2 pagesSt. Augustine School of Nursing: Republic of The Philippines Department of Education SASN - Las PiñasCarl Joseph MasujerNo ratings yet