You might also like
- Damage Control in Trauma Care: An Evolving Comprehensive Team ApproachFrom EverandDamage Control in Trauma Care: An Evolving Comprehensive Team ApproachJuan DuchesneNo ratings yet
- Dec24 16 PDFDocument8 pagesDec24 16 PDFijasrjournalNo ratings yet
- Mastitis 2Document4 pagesMastitis 2lolytofarisaNo ratings yet
- Clinical Presentation of Peritoneal MesotheliomaDocument5 pagesClinical Presentation of Peritoneal Mesotheliomamalvina.sekolonik911No ratings yet
- Liang 2016Document4 pagesLiang 2016danielleclimacoNo ratings yet
- A Case of Gastric Schwannoma: Sciences, Porompat, Imphal. Sciences, Porompat, Imphal. Imphal. Sciences, Porompat, ImphalDocument7 pagesA Case of Gastric Schwannoma: Sciences, Porompat, Imphal. Sciences, Porompat, Imphal. Imphal. Sciences, Porompat, ImphalFerina Nur HaqiqiNo ratings yet
- Ovarian Cysts and Tumors in Infancy and Childhood: Riginal RticleDocument4 pagesOvarian Cysts and Tumors in Infancy and Childhood: Riginal RticleIwan Budianto HadiNo ratings yet
- Management Fam 1998Document5 pagesManagement Fam 1998Envhy WinaNo ratings yet
- Faz Zio 2016Document9 pagesFaz Zio 2016seruniallisaaslimNo ratings yet
- Dematos 1997Document6 pagesDematos 1997Ali AmokraneNo ratings yet
- The Cystic MesotheliomaDocument7 pagesThe Cystic MesotheliomaInternational Medical PublisherNo ratings yet
- Ojped 2024030813565746Document6 pagesOjped 2024030813565746Nicolás Mosso F.No ratings yet
- A Case of Giant Uterine Fibroid in A Toung WomanDocument5 pagesA Case of Giant Uterine Fibroid in A Toung WomanTETINOUNo ratings yet
- Nephroblastoma: Radiological and Pathological Diagnosis of A Case With Liver MetastasesDocument5 pagesNephroblastoma: Radiological and Pathological Diagnosis of A Case With Liver MetastasesfifahcantikNo ratings yet
- Lipoma of The Uterine Corpus Exceptional Eventuality Combined With An Ovarian ThecomaDocument5 pagesLipoma of The Uterine Corpus Exceptional Eventuality Combined With An Ovarian ThecomaAlex HydronNo ratings yet
- Invaginasi Jurnal2 PDFDocument4 pagesInvaginasi Jurnal2 PDFZieky YoansyahNo ratings yet
- GMC PublishedDocument3 pagesGMC PublishedAyanawNo ratings yet
- Testicular Tumors in Undescended Testes in Children Below 5 y of AgeDocument4 pagesTesticular Tumors in Undescended Testes in Children Below 5 y of AgeDhruv MahajanNo ratings yet
- Skipidip Skipidap Colonic Hernia YyeewaghDocument4 pagesSkipidip Skipidap Colonic Hernia YyeewaghSu-sake KonichiwaNo ratings yet
- Medicine: Recurrent Juvenile Fibroadenoma of The Breast in An AdolescentDocument3 pagesMedicine: Recurrent Juvenile Fibroadenoma of The Breast in An AdolescentnovaNo ratings yet
- Askin TumorDocument6 pagesAskin TumorGaluh Kresna BayuNo ratings yet
- Benign Esophageal TumorsDocument24 pagesBenign Esophageal TumorsMikael Angeloo100% (1)
- Cap Polyposis in Children: Case Report and Literature ReviewDocument6 pagesCap Polyposis in Children: Case Report and Literature ReviewLuis ArrietaNo ratings yet
- Neonatal Extra-Renal Wilm's Tumour: Division of Paediatric Surgery, Aga Khan University Hospital, KarachiDocument2 pagesNeonatal Extra-Renal Wilm's Tumour: Division of Paediatric Surgery, Aga Khan University Hospital, Karachidydy_7193No ratings yet
- Meigs' Syndrome and Pseudo-Meigs' Syndrome: Report of Four Cases and Literature ReviewsDocument6 pagesMeigs' Syndrome and Pseudo-Meigs' Syndrome: Report of Four Cases and Literature ReviewsAlfa FebriandaNo ratings yet
- Kurtz 2016Document5 pagesKurtz 2016Stevano PattiasinaNo ratings yet
- Jurnal TambahanDocument5 pagesJurnal TambahanKaleb Rudy HartawanNo ratings yet
- Case Report EndometriosisDocument4 pagesCase Report EndometriosischristinejoanNo ratings yet
- AMasculine PresentingFemaleAdolescentaRareCaseofPoorly DifferentiatedSertoli LeydigCellTumorDocument15 pagesAMasculine PresentingFemaleAdolescentaRareCaseofPoorly DifferentiatedSertoli LeydigCellTumorDaniella Ashley BaltesNo ratings yet
- Igg4-Related Hypophysitis Presenting As A Pituitary Adenoma With Systemic DiseaseDocument5 pagesIgg4-Related Hypophysitis Presenting As A Pituitary Adenoma With Systemic DiseasefelipetheNo ratings yet
- HGMX 22 85 3 131-134Document4 pagesHGMX 22 85 3 131-134Julio BarajasNo ratings yet
- Adult Intussussception Int J Student Res 2012Document3 pagesAdult Intussussception Int J Student Res 2012Juan De Dios Diaz-RosalesNo ratings yet
- v1Document8 pagesv1Pulasthi KanchanaNo ratings yet
- 1 s2.0 S2352646718301509 MainDocument3 pages1 s2.0 S2352646718301509 MainGilbert MenesesNo ratings yet
- Casereports 18 125 PDFDocument6 pagesCasereports 18 125 PDFAstrianti Kusuma WardaniNo ratings yet
- Krukenberg Tumour Simulating Uterine Fibroids and Pelvic Inflammatory DiseaseDocument3 pagesKrukenberg Tumour Simulating Uterine Fibroids and Pelvic Inflammatory DiseaseradianrendratukanNo ratings yet
- 02 Rapunzel Syndrome - An Uncommon Problem in ChildrenDocument3 pages02 Rapunzel Syndrome - An Uncommon Problem in ChildrenAli AhmadNo ratings yet
- 10 18017-Iuitfd 308495-296849Document3 pages10 18017-Iuitfd 308495-296849asshagab04No ratings yet
- Mucinous Adenocarcinoma FinalDocument16 pagesMucinous Adenocarcinoma Finalritzy0997No ratings yet
- Tumeurs Ovariennes A Cellulles de La Granulosa Juveniles (1) DjeltiDocument7 pagesTumeurs Ovariennes A Cellulles de La Granulosa Juveniles (1) DjeltiDjelti SihemNo ratings yet
- Stem Cell OsteosarcomaDocument5 pagesStem Cell OsteosarcomaHendrikus Surya Adhi PutraNo ratings yet
- Infectious IleoceicitisDocument2 pagesInfectious IleoceicitisYandiNo ratings yet
- An Unusual Cause of "Appendicular Pain" in A Young Girl: Mesenteric Cystic LymphangiomaDocument3 pagesAn Unusual Cause of "Appendicular Pain" in A Young Girl: Mesenteric Cystic LymphangiomaSherif Abou BakrNo ratings yet
- Giant Adrenal Myelolipoma As A Cause of Chronic Abdominal Pain Abdominal Pain Due To Giant MyelolipomaDocument8 pagesGiant Adrenal Myelolipoma As A Cause of Chronic Abdominal Pain Abdominal Pain Due To Giant MyelolipomaAthenaeum Scientific PublishersNo ratings yet
- Postgrad Med J 2005 Yalamarthi 174 7Document5 pagesPostgrad Med J 2005 Yalamarthi 174 7Novendi RizkaNo ratings yet
- Managing The Risk of Cancer in Cowden Syndrome: A Case ReportDocument4 pagesManaging The Risk of Cancer in Cowden Syndrome: A Case ReportKaisun TeoNo ratings yet
- 1 s2.0 S2210261218301822 MainDocument3 pages1 s2.0 S2210261218301822 Mainfatini hikariNo ratings yet
- Jurnal MelenaDocument4 pagesJurnal MelenaMadetolis PhotoworksNo ratings yet
- Jgo 21 129 PDFDocument3 pagesJgo 21 129 PDFJuan Carlos Parraga SanclementeNo ratings yet
- Abdominal Tuberculosis in Children: You Could Be Reading The Full-Text of This Article Now..Document1 pageAbdominal Tuberculosis in Children: You Could Be Reading The Full-Text of This Article Now..DrMukesh BhaskarNo ratings yet
- Intralesional Bleomycin Sclerotherapy in Childhood LymphangiomaDocument5 pagesIntralesional Bleomycin Sclerotherapy in Childhood LymphangiomaHendrikNo ratings yet
- EndometriosisDocument17 pagesEndometriosisIngrid HerreraNo ratings yet
- Jurnal Radiologi 3Document10 pagesJurnal Radiologi 3Yuni AurraNo ratings yet
- Clin Cas 1Document5 pagesClin Cas 1Dragos Viorel ScripcariuNo ratings yet
- Paper Presentation On Trichobezoars A Hairy Cause of Intestinal ObstructionDocument14 pagesPaper Presentation On Trichobezoars A Hairy Cause of Intestinal ObstructionAimanNo ratings yet
- Idiopathic Granulomatous Mastitis: Case Report and Review of The LiteratureDocument4 pagesIdiopathic Granulomatous Mastitis: Case Report and Review of The LiteratureZaireen TahirNo ratings yet
- International Journal of Surgery Case ReportsDocument3 pagesInternational Journal of Surgery Case ReportsJuan Eduardo Rios RodriguezNo ratings yet
- Lymphangioma Vs HemangiomaDocument5 pagesLymphangioma Vs HemangiomaArif oktavianNo ratings yet
- Patho Lab Git 2Document3 pagesPatho Lab Git 2Jannatul Adnin JinanNo ratings yet
- Juvenile Fibroadenoma of The Breast: Treatment and Literature ReviewDocument5 pagesJuvenile Fibroadenoma of The Breast: Treatment and Literature ReviewnatzevaraNo ratings yet
- Tanaffos 10 052Document5 pagesTanaffos 10 052Lisma EkayantiNo ratings yet
- Colorectal Emergencies Associated With Penetrating or Retained Foreign BodiesDocument5 pagesColorectal Emergencies Associated With Penetrating or Retained Foreign BodiesLisma EkayantiNo ratings yet
- Asm 5 444Document3 pagesAsm 5 444Lisma EkayantiNo ratings yet
- Heterotopic Pregnancy With Successful Pregnancy Outcome: Nasreen Noor, Imam Bano, Shazia ParveenDocument2 pagesHeterotopic Pregnancy With Successful Pregnancy Outcome: Nasreen Noor, Imam Bano, Shazia ParveenLisma EkayantiNo ratings yet
- Tanaffos 10 052Document5 pagesTanaffos 10 052Lisma EkayantiNo ratings yet
- Annals of Medicine and Surgery: E.A. Sule, M.A. Nzegwu, J.C. Okolo, R.U. OnyemekheiaDocument5 pagesAnnals of Medicine and Surgery: E.A. Sule, M.A. Nzegwu, J.C. Okolo, R.U. OnyemekheiaLisma EkayantiNo ratings yet
- Body Mass Index: More Than Just A Number: Endocrinology, Metabolic Disorders, ObesityDocument1 pageBody Mass Index: More Than Just A Number: Endocrinology, Metabolic Disorders, ObesityLisma EkayantiNo ratings yet
- Ghid 2017 Hipertensiune La Copii Si AdolescentiDocument74 pagesGhid 2017 Hipertensiune La Copii Si Adolescentiflori.bNo ratings yet
- EXPERIMENT 3.6: Determining The Concentration of An External Solution Which Is Isotonic To The Cell Sap of A PlantDocument2 pagesEXPERIMENT 3.6: Determining The Concentration of An External Solution Which Is Isotonic To The Cell Sap of A PlantAmsyidi AsmidaNo ratings yet
- Indira Renganathan 2018 18Document1,992 pagesIndira Renganathan 2018 18shubham vedakNo ratings yet
- Approved LaboratoriesDocument22 pagesApproved LaboratoriesPaul CNo ratings yet
- Tomasello, M. (2000) - Culture and Cognitive Development.Document4 pagesTomasello, M. (2000) - Culture and Cognitive Development.Roberto OcampoNo ratings yet
- Masters Portfolio - MSC EmTech (AA, London)Document56 pagesMasters Portfolio - MSC EmTech (AA, London)asad nasirNo ratings yet
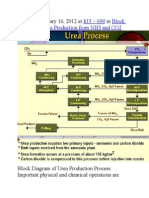
- Published January 16, 2012 at In: 813 × 699 Block Diagram of Urea Production From NH3 and CO2Document9 pagesPublished January 16, 2012 at In: 813 × 699 Block Diagram of Urea Production From NH3 and CO2himanshuchawla654No ratings yet
- Aims Stress - The SeedDocument27 pagesAims Stress - The SeedFx KovacsNo ratings yet
- Blood Doping PPT PresentationDocument26 pagesBlood Doping PPT Presentationee4254100% (1)
- 8610 - 1 Maham AslamDocument21 pages8610 - 1 Maham AslamMuhammad BasitNo ratings yet
- Clinical Biochemistry PDFDocument105 pagesClinical Biochemistry PDFJepri Purwanto67% (3)
- Cat ExamDocument25 pagesCat Examlahsivlahsiv684No ratings yet
- Noncanonical Transnitrosylation Network Contributes To Synapse Loss in Alzheimer's DiseaseDocument18 pagesNoncanonical Transnitrosylation Network Contributes To Synapse Loss in Alzheimer's DiseasedmitworNo ratings yet
- Recent DevelopmentsDocument295 pagesRecent DevelopmentsGabriel PinheiroNo ratings yet
- Jane Goodall BiographyDocument2 pagesJane Goodall BiographyOjas JangalNo ratings yet
- Chapter 1Document4 pagesChapter 1Nikoleta RudnikNo ratings yet
- A Double-Strain TM (gp45) Polypeptide Antigen and Its Application in The Serodiadnosis of Equine Infectius AnemiaDocument8 pagesA Double-Strain TM (gp45) Polypeptide Antigen and Its Application in The Serodiadnosis of Equine Infectius AnemiaFredy MoralesNo ratings yet
- 6.1 MicrobiologyDocument32 pages6.1 MicrobiologyYsabelle BautistaNo ratings yet
- Multiple AlleleDocument3 pagesMultiple AlleleAdroit SangmaNo ratings yet
- Angiogenesis and Direct Myocardial RevascularizationDocument364 pagesAngiogenesis and Direct Myocardial RevascularizationPerdana SidaurukNo ratings yet
- Kimia Daun PandanDocument4 pagesKimia Daun Pandanlutfi_alhayathullahNo ratings yet
- 1 s2.0 S222541102200030X MainDocument11 pages1 s2.0 S222541102200030X Mainaman babuNo ratings yet
- FTS - 11 (Code-A) - 24-04-2020 PDFDocument16 pagesFTS - 11 (Code-A) - 24-04-2020 PDFkavyareddyNo ratings yet
- 0 AlignMeDocument6 pages0 AlignMeCRISTIAN GABRIEL ZAMBRANO VEGANo ratings yet
- PDFDocument570 pagesPDFEshaal FatimaNo ratings yet
- Preparation of Histological SpecimensDocument4 pagesPreparation of Histological SpecimensAqilah HazwaniNo ratings yet
- 300 One Word Substitutions Asked in SSC IBPS UPSC ExamDocument12 pages300 One Word Substitutions Asked in SSC IBPS UPSC ExamRashid AliNo ratings yet
- Social IntelligenceDocument10 pagesSocial IntelligencePeterMarquezNo ratings yet
- Alvin MDocument2 pagesAlvin MRunmel Emmanuel Ramal DampiosNo ratings yet
- G.B.Pant University of Agriculture & Technology, Pantnagar-263145, Distt. Udham Singh Nagar (Uttarakhand) University Website: WWW - Gbpuat.ac - inDocument4 pagesG.B.Pant University of Agriculture & Technology, Pantnagar-263145, Distt. Udham Singh Nagar (Uttarakhand) University Website: WWW - Gbpuat.ac - inJeshiNo ratings yet
- Email To Professor SampleDocument6 pagesEmail To Professor SamplesimplecobraNo ratings yet