You might also like
- The Crash CartDocument39 pagesThe Crash Cartpramod kumawat100% (1)
- IM On Call (LANGE On Call) PDFDocument738 pagesIM On Call (LANGE On Call) PDFindia2puppy100% (8)
- Pharmacology Viva QuestionsDocument24 pagesPharmacology Viva QuestionsMinhaz Islam100% (1)
- Basic Pharmacology And Drug Calculations [Practice Questions And Answers]From EverandBasic Pharmacology And Drug Calculations [Practice Questions And Answers]Rating: 4 out of 5 stars4/5 (1)
- Antiarrhythmic Drugs Classification (Vaughan Williams)Document8 pagesAntiarrhythmic Drugs Classification (Vaughan Williams)ana100% (1)
- Emergency DrugsDocument47 pagesEmergency DrugsBesimanNo ratings yet
- Anti-Anginal DrugsDocument39 pagesAnti-Anginal Drugspoonam rana100% (1)
- Angina Pectoris & Anti Anginal DrugsDocument46 pagesAngina Pectoris & Anti Anginal DrugsMohammad AliNo ratings yet
- LECTURE 9 Positive InotropicDocument5 pagesLECTURE 9 Positive InotropicanaNo ratings yet
- 06 JunioDocument152 pages06 Juniocristian GamaNo ratings yet
- 25 Address PDF MergedDocument1,744 pages25 Address PDF Mergedsanjay_gawaliNo ratings yet
- ACLS DrugsDocument16 pagesACLS Drugstostc100% (2)
- Drugs Used in Myocardial InfarctionDocument53 pagesDrugs Used in Myocardial InfarctionSandeep KannegantiNo ratings yet
- Pharmacology of The Gastrointestinal Drugs (I)Document12 pagesPharmacology of The Gastrointestinal Drugs (I)anaNo ratings yet
- Price List Pt. Hexpharm Jaya 2020Document3 pagesPrice List Pt. Hexpharm Jaya 2020RetnoSFadhillahNo ratings yet
- On Emergency DrugsDocument25 pagesOn Emergency DrugsBikram Chhetry100% (1)
- ANTI-ARRHYTHMIC DRUGS Veterinary PharmacologyDocument5 pagesANTI-ARRHYTHMIC DRUGS Veterinary PharmacologyljramosNo ratings yet
- Nitrates andDocument61 pagesNitrates andMrunalini DandamudiNo ratings yet
- Pharmacology RevisedDocument59 pagesPharmacology Revisedjohnstockton12100% (1)
- Nitrates Comparison ChartDocument7 pagesNitrates Comparison ChartModi Evana PutriNo ratings yet
- Pharmacology of Antianginal Drugs: Tri Widyawati M. IchwanDocument43 pagesPharmacology of Antianginal Drugs: Tri Widyawati M. IchwanYohanna SinuhajiNo ratings yet
- Drugs 2018 FebDocument143 pagesDrugs 2018 FebTuliNo ratings yet
- Role of Nitrates in Angina: Satabdi Ghosh Phase A Resident Department of Pharmacology, BSMMUDocument17 pagesRole of Nitrates in Angina: Satabdi Ghosh Phase A Resident Department of Pharmacology, BSMMUMehediNo ratings yet
- Supply Chain & Inventory ControlDocument99 pagesSupply Chain & Inventory ControlSUMIT MASKENo ratings yet
- Emergency Drugs GuideDocument8 pagesEmergency Drugs GuideShehnaz SheikhNo ratings yet
- ED Dilution Guide 2018 - Jan 2019Document42 pagesED Dilution Guide 2018 - Jan 2019asyrafrusydi9901No ratings yet
- Emergency Tray PesentationDocument14 pagesEmergency Tray Pesentationgaladimawa2002No ratings yet
- A Drug Study On: EpinephrineDocument16 pagesA Drug Study On: EpinephrineJay Jay JayyiNo ratings yet
- Online Practice Tests, Live Classes, Tutoring, Study Guides Q&A, Premium Content and MoreDocument112 pagesOnline Practice Tests, Live Classes, Tutoring, Study Guides Q&A, Premium Content and MoreabctutorNo ratings yet
- Antianginal Drugs Antianginal Drugs Are Used Primarily To Restore The Balance Between TheDocument10 pagesAntianginal Drugs Antianginal Drugs Are Used Primarily To Restore The Balance Between TheMIR SARTAJNo ratings yet
- Cardiac DrugDocument32 pagesCardiac DrugSalim MinjNo ratings yet
- Drugs Study Neh Jai2xDocument10 pagesDrugs Study Neh Jai2xjai2xNo ratings yet
- Cad Sihd 2Document67 pagesCad Sihd 2mohammedghassan53No ratings yet
- InotropicsDocument20 pagesInotropicsMalathi VarnaNo ratings yet
- Clinical Cases Pharmacology PDFDocument7 pagesClinical Cases Pharmacology PDFAnkur HazraNo ratings yet
- BretyliumDocument4 pagesBretyliumButchay LumbabNo ratings yet
- Cardiac Medications: 1. Antiplatelet Aggregation Therapy: Antiplatelet Aggregation TherapyDocument14 pagesCardiac Medications: 1. Antiplatelet Aggregation Therapy: Antiplatelet Aggregation TherapyMaria OnofreiNo ratings yet
- Antidotes, Anticholinergics and Antibiotics: Amrit Pokhrel PharmacistDocument21 pagesAntidotes, Anticholinergics and Antibiotics: Amrit Pokhrel PharmacistheenamaharjanNo ratings yet
- Farma StrokeDocument37 pagesFarma StrokeDAHLIANo ratings yet
- Relief of Pain, Inflammation and Rheumatic ConditionsDocument16 pagesRelief of Pain, Inflammation and Rheumatic Conditionsdemolay03No ratings yet
- Antiarrhytmic Talk For ResidenDocument90 pagesAntiarrhytmic Talk For ResidenMusa yohanaNo ratings yet
- Outpatient MedicineDocument190 pagesOutpatient MedicineLikoh TimothyNo ratings yet
- Mosby - Mosby's Drug Reference For Health Professions, 4e-Mosby (2013) - DeletedDocument3 pagesMosby - Mosby's Drug Reference For Health Professions, 4e-Mosby (2013) - DeletedehsanNo ratings yet
- Problem 2Document9 pagesProblem 2Chan Myae NaingNo ratings yet
- Atrial Flutter Medication: Drugs DoseDocument8 pagesAtrial Flutter Medication: Drugs DoseVictoria Castillo TamayoNo ratings yet
- Management Strategy in Hypertensive Crisis The Role of NicardipineDocument38 pagesManagement Strategy in Hypertensive Crisis The Role of Nicardipinezulfikar adiNo ratings yet
- Cardiac DrugsDocument21 pagesCardiac DrugsMona MahfouzNo ratings yet
- OBAT PADA REAKSI HIPERSENSITIVITASDocument59 pagesOBAT PADA REAKSI HIPERSENSITIVITASM Rasya SanimanNo ratings yet
- CardioDocument28 pagesCardioKristine Joy CamusNo ratings yet
- Master Emergency Drugs Before U Practise DR Vishwa Medical CoachingDocument6 pagesMaster Emergency Drugs Before U Practise DR Vishwa Medical Coachingابو عبد الرحمنNo ratings yet
- Atropine: IndicationDocument2 pagesAtropine: IndicationgugicevdzoceNo ratings yet
- Cardiovascular Drugs and Therapies Nitrates Comparison ChartDocument7 pagesCardiovascular Drugs and Therapies Nitrates Comparison ChartArvi J-idNo ratings yet
- ST-Elevation Myocardial Infarction (STEMI) Diagnosis and TreatmentDocument8 pagesST-Elevation Myocardial Infarction (STEMI) Diagnosis and TreatmentamiraNo ratings yet
- Lab 9 RespitatoryDocument3 pagesLab 9 RespitatoryanaNo ratings yet
- Cardiology and endocrine dosesDocument3 pagesCardiology and endocrine dosesSelim TarekNo ratings yet
- AMI Management For 2 ND Year StudentsDocument3 pagesAMI Management For 2 ND Year StudentsShubham TarapureNo ratings yet
- Common Emergency DrugsDocument61 pagesCommon Emergency DrugsFebee Gee100% (1)
- Commonly Used Critical Care Medications: IV Bolus 6 MG, If Conversion To NSR Does Not Occur Within 1-2Document7 pagesCommonly Used Critical Care Medications: IV Bolus 6 MG, If Conversion To NSR Does Not Occur Within 1-2ciptaarynNo ratings yet
- Prescription Writing 1Document10 pagesPrescription Writing 1amaygokhale26802No ratings yet
- 2 2015 Nsaid Analgetik AntipiretikaDocument65 pages2 2015 Nsaid Analgetik AntipiretikasekarNo ratings yet
- Antianginal Drugs Are Used Primarily To Restore The Balance Between The Oxygen SupplyDocument8 pagesAntianginal Drugs Are Used Primarily To Restore The Balance Between The Oxygen SupplyUzma KhanNo ratings yet
- GP RSD KALABAHI drug formularyDocument2 pagesGP RSD KALABAHI drug formularyyosaNo ratings yet
- Cardiac Glycosides and Phosphodiesterase InhibitorsDocument30 pagesCardiac Glycosides and Phosphodiesterase Inhibitorskenneth santosNo ratings yet
- Pertemuan 7 LiyanaDocument36 pagesPertemuan 7 LiyanaLiyana SafitriNo ratings yet
- Infant Care - Practical Course PDFDocument165 pagesInfant Care - Practical Course PDFBogdan MariusNo ratings yet
- Ultrasound 20atlas 20of 20clinical 20casesDocument119 pagesUltrasound 20atlas 20of 20clinical 20casesTimbur IgorNo ratings yet
- Chirurgie PrimaraDocument144 pagesChirurgie PrimaraElena ConstantinNo ratings yet
- Vladimir Fluture-The Path From The Surgical Dream To The Perfect Operation Ebook Final PDFDocument115 pagesVladimir Fluture-The Path From The Surgical Dream To The Perfect Operation Ebook Final PDFAdriana DuțăNo ratings yet
- Infant 20care 202020 PDFDocument226 pagesInfant 20care 202020 PDFRusaneanu Robert-CatalinNo ratings yet
- Infant 20care 202020 PDFDocument226 pagesInfant 20care 202020 PDFRusaneanu Robert-CatalinNo ratings yet
- LAB 8 MGE-drugsDocument2 pagesLAB 8 MGE-drugsanaNo ratings yet
- Lab PharmacoDocument51 pagesLab PharmacoanaNo ratings yet
- The 20human 20body. 20a 20sum 20of 20anthropological 20introductions PDFDocument136 pagesThe 20human 20body. 20a 20sum 20of 20anthropological 20introductions PDFRusaneanu Robert-CatalinNo ratings yet
- Farmaco LectureDocument117 pagesFarmaco LectureanaNo ratings yet
- Lab 7-Practic Aplic.Document5 pagesLab 7-Practic Aplic.anaNo ratings yet
- Infant Care - Practical Course PDFDocument165 pagesInfant Care - Practical Course PDFBogdan MariusNo ratings yet
- Human Anatomy Central Nervous System PDFDocument75 pagesHuman Anatomy Central Nervous System PDFBogdan MariusNo ratings yet
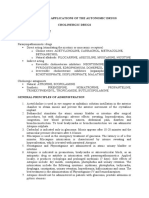
- Practical Applications of The Antihypertensive Drugs I. Theoretical Part ClassificationDocument4 pagesPractical Applications of The Antihypertensive Drugs I. Theoretical Part ClassificationanaNo ratings yet
- Lab 9 RespitatoryDocument3 pagesLab 9 RespitatoryanaNo ratings yet
- The Pharmacology of AntithromboticsDocument14 pagesThe Pharmacology of AntithromboticsanaNo ratings yet
- LAB 12+13 Blood Medic.Document4 pagesLAB 12+13 Blood Medic.anaNo ratings yet
- Human Body and Skeleton Medical VocabularyDocument3 pagesHuman Body and Skeleton Medical VocabularyanaNo ratings yet
- Human Anatomy Central Nervous System PDFDocument75 pagesHuman Anatomy Central Nervous System PDFBogdan MariusNo ratings yet
- Pharmacology of The Gastrointestinal Drugs (Ii) Choleretics, Cholagogues and Other Biliary Secretion ModifiersDocument14 pagesPharmacology of The Gastrointestinal Drugs (Ii) Choleretics, Cholagogues and Other Biliary Secretion ModifiersanaNo ratings yet
- LECTURE 8 AntihypertensiveDocument18 pagesLECTURE 8 AntihypertensiveanaNo ratings yet
- Drugs Acting On The Blood and The Blood-Forming Organs Pharmacology of Antianemic DrugsDocument6 pagesDrugs Acting On The Blood and The Blood-Forming Organs Pharmacology of Antianemic DrugsanaNo ratings yet
- Dialog Medic PacientDocument4 pagesDialog Medic PacientanaNo ratings yet
- Pulmonary Pharmacology Anticoughing AgentsDocument10 pagesPulmonary Pharmacology Anticoughing AgentsanaNo ratings yet
- Laporan Apotik Ugd Stok OpnameDocument26 pagesLaporan Apotik Ugd Stok OpnameIndSara 07No ratings yet
- PRICELIST JANUARI 2022 (AutoRecovered)Document26 pagesPRICELIST JANUARI 2022 (AutoRecovered)taufanmjNo ratings yet
- Antitussives & MucolyticsDocument50 pagesAntitussives & MucolyticsSaha DirllahNo ratings yet
- Bogash 1963Document5 pagesBogash 1963wahyu santikaNo ratings yet
- Ejercicio 1. Unidad 1 ReadingDocument5 pagesEjercicio 1. Unidad 1 ReadingLenNo ratings yet
- Transes Fundamentals of PharmacologyDocument4 pagesTranses Fundamentals of PharmacologyCHINGCHONG SLAYERNo ratings yet
- Pharmacology Assignment - Medicines and MealsDocument15 pagesPharmacology Assignment - Medicines and MealsFarhat JahanNo ratings yet
- Dosage FormDocument5 pagesDosage Formqbn9vx7t9jNo ratings yet
- Laporan Perencanaan Perbekalan FarmasiDocument11 pagesLaporan Perencanaan Perbekalan FarmasikarinaNo ratings yet
- warfarin (Coumadin) - UW Medicine Anticoagulation Services Https Sites - Uw.edu Anticoag Drugs WarfarinDocument12 pageswarfarin (Coumadin) - UW Medicine Anticoagulation Services Https Sites - Uw.edu Anticoag Drugs Warfarintl drNo ratings yet
- Basic principles of pharmacology classification and drug administrationDocument4 pagesBasic principles of pharmacology classification and drug administrationJayla MarieNo ratings yet
- Copaxone - Ms Drug StudyDocument1 pageCopaxone - Ms Drug StudygraceNo ratings yet
- Injeksi & Oplosan ObatDocument16 pagesInjeksi & Oplosan ObatFebriani RatnaNo ratings yet
- 3.one Compartment Open ModelDocument15 pages3.one Compartment Open ModelSAM KNo ratings yet
- Dangerous DrugsDocument9 pagesDangerous DrugsEarvin Recel GuidangenNo ratings yet
- Sympathomimetics Physical MCQDocument4 pagesSympathomimetics Physical MCQMohamed MoustafaNo ratings yet
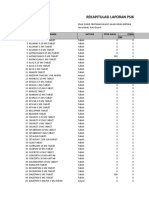
- Rekapitulasi Laporan Psikotropika: NO Nama Satuan Stok Awal Pemasukan PBFDocument9 pagesRekapitulasi Laporan Psikotropika: NO Nama Satuan Stok Awal Pemasukan PBFlarasNo ratings yet
- Websitecompanies NewDocument33 pagesWebsitecompanies NewRajiv JulakantiNo ratings yet
- LED-Face-Mask-Consultation-Form - 2Document2 pagesLED-Face-Mask-Consultation-Form - 2Hanan AnsariNo ratings yet
- List Signals Discussed Prac September 2012 - en Till 31-07-2023Document62 pagesList Signals Discussed Prac September 2012 - en Till 31-07-2023Amany HagageNo ratings yet
- @jeeneetprep PGMEE Test SeriesDocument410 pages@jeeneetprep PGMEE Test SeriesL.ABHISHEK KUMARNo ratings yet
- Autocoids 1Document9 pagesAutocoids 1Rutwik YNo ratings yet
- Active Ingredients: Benzocaine, Bismuth Subgallate, Zinc Oxide, MentholDocument2 pagesActive Ingredients: Benzocaine, Bismuth Subgallate, Zinc Oxide, MentholHellcroZNo ratings yet
- Biovion Pharma Product List January 2021Document4 pagesBiovion Pharma Product List January 2021syedsajjadaliNo ratings yet
- Pharmexil - All MixedDocument14 pagesPharmexil - All MixedLisa RayNo ratings yet
- Principles of Drug TherapyDocument8 pagesPrinciples of Drug TherapySNo ratings yet




![Basic Pharmacology And Drug Calculations [Practice Questions And Answers]](https://imgv2-2-f.scribdassets.com/img/word_document/475660044/149x198/2c7fc45015/1691161640?v=1)