You might also like
- W19 BMJ Managing Common Breast Feeding Problems in The CommunityDocument9 pagesW19 BMJ Managing Common Breast Feeding Problems in The CommunityGabriel CampolinaNo ratings yet
- Mastitis Prevention and TreatmentDocument25 pagesMastitis Prevention and TreatmentGeetha SoundaryaNo ratings yet
- 001 Lactational MastitisDocument19 pages001 Lactational MastitisMuh AfdholNo ratings yet
- Mastitis 2Document25 pagesMastitis 2Riana Pasca RoshianNo ratings yet
- RLE 109 Group 4 Case Analysis in MastitisDocument20 pagesRLE 109 Group 4 Case Analysis in MastitisEugene MananganNo ratings yet
- MastitisDocument12 pagesMastitisYo ZreNo ratings yet
- Jurnal Mastitis 2Document6 pagesJurnal Mastitis 2Faizal DzikrullahNo ratings yet
- Mast It IsDocument31 pagesMast It IsKuran NitaNo ratings yet
- Breast Abcess PDFDocument4 pagesBreast Abcess PDFponekNo ratings yet
- Diseases of BreastDocument23 pagesDiseases of BreastTalal AbbasiNo ratings yet
- Breast Conditions During Pregnancy and LactationDocument3 pagesBreast Conditions During Pregnancy and LactationOsemwengie VictoriaNo ratings yet
- ABM Protocol #36 PDFDocument17 pagesABM Protocol #36 PDFRana HassanNo ratings yet
- What Is MastitisDocument4 pagesWhat Is MastitiswarlockeNo ratings yet
- Mastitis - Plugged Ducts and Breast InfectionsDocument5 pagesMastitis - Plugged Ducts and Breast InfectionsFayrouz EssawiNo ratings yet
- MDWF 1030 Carter Plugged Duct Mastitis Abscess PGDocument5 pagesMDWF 1030 Carter Plugged Duct Mastitis Abscess PGapi-366292665No ratings yet
- Lactational Mastitis Puerperal 2020Document12 pagesLactational Mastitis Puerperal 2020bgNo ratings yet
- Lactational MastitisDocument2 pagesLactational MastitisMarijosse NavarroNo ratings yet
- Jurnal Postpartum DG MastitisDocument5 pagesJurnal Postpartum DG Mastitisanggit_prihatiNo ratings yet
- Abm Clinical Protocol 4 MastitisDocument4 pagesAbm Clinical Protocol 4 MastitisFayrouz EssawiNo ratings yet
- MastitisDocument8 pagesMastitisAmalia Putri100% (1)
- Incompetent Cervix Case Analysis Subgroup 2Document44 pagesIncompetent Cervix Case Analysis Subgroup 2bunso padillaNo ratings yet
- ArlineDocument16 pagesArlinearline beshraNo ratings yet
- Kataria 2012Document6 pagesKataria 2012jjeongjjangNo ratings yet
- Caring For Women Experiencing Breast Engorgement A Case ReportDocument6 pagesCaring For Women Experiencing Breast Engorgement A Case ReportHENINo ratings yet
- Lactational Mastitis & Breast Abscess Management, An Introspection.Document17 pagesLactational Mastitis & Breast Abscess Management, An Introspection.Fayrouz EssawiNo ratings yet
- LanolinaDocument6 pagesLanolinaSamantha LoveNo ratings yet
- Aloe Vera: Jurnal Penelitian Kesehatan 1Document8 pagesAloe Vera: Jurnal Penelitian Kesehatan 1Viancha SamieraNo ratings yet
- Journal Pone 0273967Document11 pagesJournal Pone 0273967atikahnurhNo ratings yet
- Mastitis, Breast Abscess, and Granulomatous Mastitis: Ramesh Omranipour and Mahtab VasighDocument9 pagesMastitis, Breast Abscess, and Granulomatous Mastitis: Ramesh Omranipour and Mahtab VasighAlejandro Abarca VargasNo ratings yet
- Improvement in Lactation With Traditional Chinese Medicine and Western Herbal Medicine A Case StudyDocument6 pagesImprovement in Lactation With Traditional Chinese Medicine and Western Herbal Medicine A Case StudyCarleta Stan100% (1)
- A Case Study On Uterine MyomaDocument39 pagesA Case Study On Uterine MyomaAj GoNo ratings yet
- Vaginal InfectionDocument14 pagesVaginal InfectionmariaNo ratings yet
- Breast Abscess, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandBreast Abscess, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Article Wound ManagementDocument8 pagesArticle Wound ManagementKhantsa RabbaniNo ratings yet
- Physiological Changes of The PuerperiumDocument6 pagesPhysiological Changes of The PuerperiumBladimir CentenoNo ratings yet
- Medical Hypotheses: SciencedirectDocument3 pagesMedical Hypotheses: SciencedirectZazwani LidiawatiNo ratings yet
- Breast AbscessDocument56 pagesBreast AbscessAnastasia Lilian Suryajaya0% (1)
- Reasons For Miscarriage Sumber: Ancy-Problems/coping-With-Miscarriage/reasons-For-MiscarriageDocument2 pagesReasons For Miscarriage Sumber: Ancy-Problems/coping-With-Miscarriage/reasons-For-MiscarriageMega Safira Mahardini0% (1)
- Uterine FibroidsDocument21 pagesUterine Fibroidsnsrafel0No ratings yet
- Placenta PreviaDocument7 pagesPlacenta PreviaBubblets Margaux GoldiNo ratings yet
- MastatisDocument15 pagesMastatisJoven LorillaNo ratings yet
- Listeriosis in PregnancyDocument18 pagesListeriosis in PregnancyxxdrivexxNo ratings yet
- Ijms - Indonesian Journal On Medical Science - Volume 4 No 2 - 2017Document6 pagesIjms - Indonesian Journal On Medical Science - Volume 4 No 2 - 2017Dicky AhmadNo ratings yet
- Mastitis: By: Hj. Fatimah Usman, OBGYN (C)Document12 pagesMastitis: By: Hj. Fatimah Usman, OBGYN (C)David TurnerNo ratings yet
- NCM 109 Module 8Document45 pagesNCM 109 Module 8capoyljtNo ratings yet
- Pathology of The Breast: DR Panuta AndrianDocument60 pagesPathology of The Breast: DR Panuta AndrianPanuta AndrianNo ratings yet
- Puerperial PyrexiaDocument4 pagesPuerperial Pyrexiakutra3000No ratings yet
- Lo MastitisDocument12 pagesLo MastitisRaul MooreNo ratings yet
- Handouts of Complications of PostnatalDocument12 pagesHandouts of Complications of PostnatalAshish GuptaNo ratings yet
- Treatment of Bbreast InfectionDocument12 pagesTreatment of Bbreast InfectionThắng NguyễnNo ratings yet
- Infant Feeding Mastitis and Breast AbscessDocument8 pagesInfant Feeding Mastitis and Breast AbscessThắng NguyễnNo ratings yet
- Inflammatory Breast Diseases During Lactation MilkDocument6 pagesInflammatory Breast Diseases During Lactation MilkatikahnurhNo ratings yet
- Ectopic Pregnancy Definition of DisorderDocument48 pagesEctopic Pregnancy Definition of DisorderWRONGHEAR100% (1)
- Management of Uterine Fibroids in Pregnancy Recent TrendsDocument7 pagesManagement of Uterine Fibroids in Pregnancy Recent TrendsManishta Menaka DhuromsinghNo ratings yet
- Gestational Trophoblastic Disease (GTD) : Gynecology Department Case PresentationDocument27 pagesGestational Trophoblastic Disease (GTD) : Gynecology Department Case PresentationsonylynneNo ratings yet
- Penanganan Dan Perawatan Pada Ibu Menyusui Dengan Mastitis Di BPM Lukluatun Mubrikoh Qurrotu Aini, Lelly Aprilia VidayatiDocument7 pagesPenanganan Dan Perawatan Pada Ibu Menyusui Dengan Mastitis Di BPM Lukluatun Mubrikoh Qurrotu Aini, Lelly Aprilia VidayatiMutyaa PutriNo ratings yet
- Infections in The Breast - Common Imaging Presentations and MimicsDocument7 pagesInfections in The Breast - Common Imaging Presentations and MimicsAridayana HalideNo ratings yet
- SFBFPC Newsletter 5 August14Document2 pagesSFBFPC Newsletter 5 August14api-265314029No ratings yet
- Cyst Mammae SourceDocument9 pagesCyst Mammae SourcePutri AnggraeniNo ratings yet
- Maternal LEC - Week 3 - TransesDocument21 pagesMaternal LEC - Week 3 - TransesEcka- EckaNo ratings yet
- Terms in ObstetricsDocument22 pagesTerms in ObstetricsYovi pransiska JambiNo ratings yet
- Rare Case of Bicornuate Uterus With Fetal Death in A Multipara WomanDocument2 pagesRare Case of Bicornuate Uterus With Fetal Death in A Multipara WomanInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- 53 JMSCRDocument7 pages53 JMSCRAddinul FitryNo ratings yet
- Breast Pump Nutrition Education MaterialDocument3 pagesBreast Pump Nutrition Education Materialapi-607536364No ratings yet
- Complementary and Alternative Medicine in MidwiferyDocument2 pagesComplementary and Alternative Medicine in MidwiferylilahgreenyNo ratings yet
- Lactation Nation by Sarah Bird For Texas MonthlyDocument2 pagesLactation Nation by Sarah Bird For Texas MonthlySarah BirdNo ratings yet
- IVF Center in Delhi NCRDocument4 pagesIVF Center in Delhi NCRSharda JainNo ratings yet
- Mantel Haenszel Pada Hubungan Antenatal Care (Anc) Terhadap BBLR DiDocument11 pagesMantel Haenszel Pada Hubungan Antenatal Care (Anc) Terhadap BBLR Dinadia harmedikaNo ratings yet
- Health Education On Breast FeedingDocument10 pagesHealth Education On Breast FeedingSoumya Rajeswari100% (3)
- Toxemias of PregnancyDocument3 pagesToxemias of PregnancyJennelyn LumbreNo ratings yet
- Commed PPT (Deepthi)Document22 pagesCommed PPT (Deepthi)Nivedha RajanNo ratings yet
- Antepartal Fetal Assessment: Developed by D. Ann Currie, R.N.,M.S.NDocument38 pagesAntepartal Fetal Assessment: Developed by D. Ann Currie, R.N.,M.S.NismailalviNo ratings yet
- BreastfeedingDocument21 pagesBreastfeedingKarima ChiuriNo ratings yet
- Hubungan Dukungan Keluarga Dengan Tingkat Kecemasna Ibu Hamil Menghadapi Proses PersalinanDocument7 pagesHubungan Dukungan Keluarga Dengan Tingkat Kecemasna Ibu Hamil Menghadapi Proses PersalinanAsryanty AmelindaNo ratings yet
- Lubchenco Curve PDFDocument1 pageLubchenco Curve PDFWarren Lie25% (4)
- Placental ExaminationDocument5 pagesPlacental ExaminationReema Akberali nooraniNo ratings yet
- Breastfeeding Assessment Tool-BAT (Mothers Version)Document1 pageBreastfeeding Assessment Tool-BAT (Mothers Version)paanar100% (1)
- Ob-Gyn Platinum (1st Edition)Document578 pagesOb-Gyn Platinum (1st Edition)vinb100% (2)
- Definition:-The Partograph Is A Simple Chart orDocument12 pagesDefinition:-The Partograph Is A Simple Chart orBharat ThapaNo ratings yet
- Soal+jawaban NCLEX-2Document5 pagesSoal+jawaban NCLEX-2ratnaNo ratings yet
- Pi Is 0002937811009379Document9 pagesPi Is 0002937811009379Mirza FinandarNo ratings yet
- The Effect of Birth Ball Exercises During PregnancDocument8 pagesThe Effect of Birth Ball Exercises During Pregnancmona khosraviNo ratings yet
- Breastfeeding GuidelinesDocument15 pagesBreastfeeding GuidelinesDr Atef Hadedy100% (2)
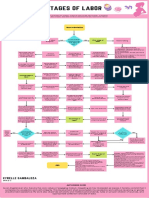
- Stages of Labor FlowchartDocument1 pageStages of Labor FlowchartXyrelle GambalozaNo ratings yet
- 2022 AJOG A Laparoscopic Approach To Cesarean Scar Ectopic PregnancyDocument3 pages2022 AJOG A Laparoscopic Approach To Cesarean Scar Ectopic PregnancyWilliam AlvarezNo ratings yet
- Utilization and Effect of Traditional Birth Attendants Among The Pregnant Women in Kahoora Division Hoima DistrictDocument13 pagesUtilization and Effect of Traditional Birth Attendants Among The Pregnant Women in Kahoora Division Hoima DistrictKIU PUBLICATION AND EXTENSIONNo ratings yet
- Obstetric Highlights Elmar P. Sakala PDFDocument47 pagesObstetric Highlights Elmar P. Sakala PDFwalt65No ratings yet
- MiscarriageDocument1 pageMiscarriageJen BallesterosNo ratings yet
- Emergency Protocol PDFDocument136 pagesEmergency Protocol PDFTasneef Chowdhury100% (1)
- Prolonged LaborDocument32 pagesProlonged Labormaezu50% (2)