You might also like
- Assesing The Appropriatenes of Parenteral Nutrition Use in Hospitalized Patients EspenDocument8 pagesAssesing The Appropriatenes of Parenteral Nutrition Use in Hospitalized Patients EspenDarío ParraNo ratings yet
- Clinical NutritionDocument12 pagesClinical NutritionBagus Candra BuanaNo ratings yet
- Bruni 2021Document2 pagesBruni 2021César Avila JimenezNo ratings yet
- The Role of Point-Of-Care Ultrasound in Intra-Abdominal Hypertension ManagementDocument9 pagesThe Role of Point-Of-Care Ultrasound in Intra-Abdominal Hypertension ManagementrjerezrNo ratings yet
- Multicentre, Cluster-Randomized Clinical Trial of Algorithms For Critical-Care Enteral and Parenteral Therapy (ACCEPT)Document8 pagesMulticentre, Cluster-Randomized Clinical Trial of Algorithms For Critical-Care Enteral and Parenteral Therapy (ACCEPT)eryxspNo ratings yet
- Nutritional Support after Gastrointestinal SurgeryFrom EverandNutritional Support after Gastrointestinal SurgeryDonato Francesco AltomareNo ratings yet
- Sezer 2020Document1 pageSezer 2020KarlaPadrelananNo ratings yet
- Protocol oDocument8 pagesProtocol oCynthia ChávezNo ratings yet
- CHRONIC DiseaseDocument6 pagesCHRONIC Diseaseberlian29031992No ratings yet
- Gastric Versus Postpyloric Enteral Nutrition in Elderly Patients (Age 75 Years) On Mechanical Ventilation: A Single-Center Randomized TrialDocument11 pagesGastric Versus Postpyloric Enteral Nutrition in Elderly Patients (Age 75 Years) On Mechanical Ventilation: A Single-Center Randomized TrialDyana NurNo ratings yet
- Nutritional Management of Patients With Enterocutaneous Fistulas: Practice and ProgressionDocument12 pagesNutritional Management of Patients With Enterocutaneous Fistulas: Practice and ProgressionKevin Howser T. ViNo ratings yet
- ContentServer 8Document7 pagesContentServer 8Fitra PahlevyNo ratings yet
- @medicinejournal European Journal of Pediatric Surgery January 2020Document126 pages@medicinejournal European Journal of Pediatric Surgery January 2020Ricardo Uzcategui ArreguiNo ratings yet
- Journal 4Document8 pagesJournal 4I Nyoman SwardyanaNo ratings yet
- 1 s2.0 S0140673623009662 MainDocument14 pages1 s2.0 S0140673623009662 MainKesia MaldonadoNo ratings yet
- 1 s2.0 S222541101630181X MainDocument5 pages1 s2.0 S222541101630181X Mainsiska khairNo ratings yet
- Enteral Versus Parenteral Nutrition in Critically Ill Patients - An Updated Systematic Review and Meta-Analysis of Randomized Controlled TrialsDocument14 pagesEnteral Versus Parenteral Nutrition in Critically Ill Patients - An Updated Systematic Review and Meta-Analysis of Randomized Controlled TrialsLea Bali Ulina SinurayaNo ratings yet
- A Prospective Randomized Controlled Trial On The Value of Prophylactic Supplementation Pral NutritionDocument7 pagesA Prospective Randomized Controlled Trial On The Value of Prophylactic Supplementation Pral NutritionOkky IrawanNo ratings yet
- ASPEN NutritionDocument18 pagesASPEN Nutritionsilvio da costa guerreiroNo ratings yet
- 08 AE 5585 Crespo IngDocument3 pages08 AE 5585 Crespo Ingcarlosalayon2No ratings yet
- 10.1007@s11739 019 02210 4Document7 pages10.1007@s11739 019 02210 4alexandraNo ratings yet
- Clinical Nutrition: Meta-AnalysesDocument13 pagesClinical Nutrition: Meta-AnalysesBby AdelinaNo ratings yet
- Pancreatology: SciencedirectDocument7 pagesPancreatology: SciencedirectLea CisnerosNo ratings yet
- Nutrition in Pancreatic Surg ISGPS 2018Document14 pagesNutrition in Pancreatic Surg ISGPS 2018Dr Ankit SharmaNo ratings yet
- 118 Reignier2010Document7 pages118 Reignier2010tereNo ratings yet
- Gasto de Energía en Reposo Preoperatorio y Postoperatorio de Pacientes Sometidos A Operaciones Abdominales MayoresDocument6 pagesGasto de Energía en Reposo Preoperatorio y Postoperatorio de Pacientes Sometidos A Operaciones Abdominales MayoresAngela SolarteNo ratings yet
- A Prospective Study On Acute Abdomen at Agogo Presbyterian Hospital (APH), Ghana: Identification of Common Causes and Pattern of PresentationDocument7 pagesA Prospective Study On Acute Abdomen at Agogo Presbyterian Hospital (APH), Ghana: Identification of Common Causes and Pattern of PresentationInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- ESPEN Practical Guideline Clinical Nutrition in SurgeryDocument17 pagesESPEN Practical Guideline Clinical Nutrition in SurgeryMaríaJoséVegaNo ratings yet
- Emergency Inguinal Hernia Repair Under Local Anesthesia: A 5-Year Experience in A Teaching HospitalDocument5 pagesEmergency Inguinal Hernia Repair Under Local Anesthesia: A 5-Year Experience in A Teaching HospitalleonardoNo ratings yet
- ESPEN Guideline Clinical Nutrition in SurgeryDocument28 pagesESPEN Guideline Clinical Nutrition in SurgeryMeliSsa DanielaNo ratings yet
- Point-Of-Care Gastric Ultrasound and Aspiration Risk Assessment - A Narrative Review PDFDocument12 pagesPoint-Of-Care Gastric Ultrasound and Aspiration Risk Assessment - A Narrative Review PDFJohana FuentesNo ratings yet
- Safety and Efficacy of Laxatives After Major Abdominal Surgery - Systematic Review and Meta-AnalysisDocument10 pagesSafety and Efficacy of Laxatives After Major Abdominal Surgery - Systematic Review and Meta-AnalysisWarren SeowNo ratings yet
- APPENDIC CASES Cuenco2020Document3 pagesAPPENDIC CASES Cuenco2020Nicole cuencosNo ratings yet
- Epidural Analgesia in Critically Ill Patients With Acute Pancreatitis: The Multicentre Randomised Controlled EPIPAN Study ProtocolDocument10 pagesEpidural Analgesia in Critically Ill Patients With Acute Pancreatitis: The Multicentre Randomised Controlled EPIPAN Study ProtocolApriany Fitri SangajiNo ratings yet
- 1 s2.0 S1015958422008909 MainDocument4 pages1 s2.0 S1015958422008909 MainYohan WijayabahuNo ratings yet
- CKB 3 IpomDocument11 pagesCKB 3 IpomNugrahaNo ratings yet
- 2021-Early Supplemental Jurnal DASDocument6 pages2021-Early Supplemental Jurnal DASiman prawiraNo ratings yet
- An Evaluation of Chest Physiotherapy in The Management of Acute Bronchiolitis Changing Clinical Practice PDFDocument6 pagesAn Evaluation of Chest Physiotherapy in The Management of Acute Bronchiolitis Changing Clinical Practice PDFKopi143No ratings yet
- Management of Peritoneal Metastases- Cytoreductive Surgery, HIPEC and BeyondFrom EverandManagement of Peritoneal Metastases- Cytoreductive Surgery, HIPEC and BeyondAditi BhattNo ratings yet
- Nutrition Practices With A Focus On Parenteral NutDocument10 pagesNutrition Practices With A Focus On Parenteral NutJose VasquezNo ratings yet
- ESPEN Guideline On Clinical Nutrition in - ICUDocument32 pagesESPEN Guideline On Clinical Nutrition in - ICUdroswaldo88No ratings yet
- International Journal of Gerontology: Original ArticleDocument5 pagesInternational Journal of Gerontology: Original ArticleFitri RahmadaniNo ratings yet
- 1 s2.0 S174391910700129X MainDocument6 pages1 s2.0 S174391910700129X MainGiorgio André Gabino GonzalezNo ratings yet
- Utd 04524 Clinical - Article KunduzDocument5 pagesUtd 04524 Clinical - Article Kunduzzenatihanen123No ratings yet
- Incidence of Histopathological Findings in Appendectomy Specimens in A Tertiary Care Hospital in Two-Year TimeDocument5 pagesIncidence of Histopathological Findings in Appendectomy Specimens in A Tertiary Care Hospital in Two-Year Timepatolog32No ratings yet
- Lassen 2008Document9 pagesLassen 2008Kaliane BCNo ratings yet
- AP ReviewDocument13 pagesAP ReviewIslam Al-ShamiNo ratings yet
- Clinical Nutrition: ESPEN GuidelineDocument18 pagesClinical Nutrition: ESPEN GuidelineMariana RodriguesNo ratings yet
- Enteral FeedingDocument5 pagesEnteral Feedingricardo arreguiNo ratings yet
- Journal Homepage: - : Manuscript HistoryDocument11 pagesJournal Homepage: - : Manuscript HistoryIJAR JOURNALNo ratings yet
- Liu 2020Document6 pagesLiu 2020Vanessa CarinoNo ratings yet
- Vaugh Alimentacio nPancreatitisAguda AnnInternMed 2017-2Document15 pagesVaugh Alimentacio nPancreatitisAguda AnnInternMed 2017-2Paula RodriguezNo ratings yet
- Vrecenak 2014Document5 pagesVrecenak 2014sigitdwimulyoNo ratings yet
- 4259 16014 1 PB PDFDocument4 pages4259 16014 1 PB PDFFiki FerindraNo ratings yet
- Perioperative Care in Elective Colonic Surgery ERASDocument18 pagesPerioperative Care in Elective Colonic Surgery ERASBeatriz MDNo ratings yet
- 1 s2.0 S0261561420301941 MainDocument8 pages1 s2.0 S0261561420301941 MainNatalia BeltranNo ratings yet
- Association Between Early Nutrition Support and 28-Day Mortality in Critically Ill Patients: The FRANS Prospective Nutrition Cohort StudyDocument14 pagesAssociation Between Early Nutrition Support and 28-Day Mortality in Critically Ill Patients: The FRANS Prospective Nutrition Cohort StudyAndike Catur WulansariNo ratings yet
- Addressing Frequent Issues of Home Enteral Nutrition PatientsDocument10 pagesAddressing Frequent Issues of Home Enteral Nutrition PatientsRaquel MirandaNo ratings yet
- Fast-Track Recovery Programme After Pancreatico-Duodenectomy Reduces Delayed Gastric EmptyingDocument7 pagesFast-Track Recovery Programme After Pancreatico-Duodenectomy Reduces Delayed Gastric EmptyinghoangducnamNo ratings yet
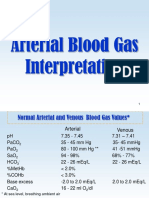
- Arterial Blood Gas InterpretationDocument69 pagesArterial Blood Gas InterpretationostuffeNo ratings yet
- Respiratory Failure PDFDocument5 pagesRespiratory Failure PDFOxana Turcu100% (1)
- KTP 1 RespiratoryDocument5 pagesKTP 1 RespiratoryMarisa TullochNo ratings yet
- Mechanical VentilationDocument29 pagesMechanical VentilationAbdul Hamid Alraiyes100% (8)
- Acute Respiratory Distress Syndrome - The Berlin Definition.Document8 pagesAcute Respiratory Distress Syndrome - The Berlin Definition.drschutterNo ratings yet
- Zhao - 2023 - The Impact of The New Acute Respiratory Distress SDocument10 pagesZhao - 2023 - The Impact of The New Acute Respiratory Distress Sgavain.ferronsNo ratings yet
- Low Flow Oxygen Delivery Via Nasal Cannula To NeonatesDocument4 pagesLow Flow Oxygen Delivery Via Nasal Cannula To NeonateskinemasNo ratings yet
- Acute Respiratory Distress Syndrome NEJM 2018Document11 pagesAcute Respiratory Distress Syndrome NEJM 2018darlingcarvajalduqueNo ratings yet
- Oxygen For A Premature, Newborn, Neonate or InfantDocument3 pagesOxygen For A Premature, Newborn, Neonate or InfantVaseem ZamairNo ratings yet
- Board Exam PrepDocument108 pagesBoard Exam PrepAnonymous FvUBZa100% (1)
- High Flow Formulas PDFDocument16 pagesHigh Flow Formulas PDFFernando Vinícius G. Magro100% (2)
- Metas de Oxigeno 2021Document11 pagesMetas de Oxigeno 2021Javier López CastellanosNo ratings yet
- Disfagia Post Extubación Es Persistente y Asociada A Malos Resultados en Sobrevivientes de Enfermedades CriticasDocument9 pagesDisfagia Post Extubación Es Persistente y Asociada A Malos Resultados en Sobrevivientes de Enfermedades CriticasKatherine Lepe AbarcaNo ratings yet
- The Sequential Organ Failure Assessment (SOFA) ScoreDocument5 pagesThe Sequential Organ Failure Assessment (SOFA) ScoreDimitri GusmaoNo ratings yet
- ARDS Berlin Definition - JAMADocument8 pagesARDS Berlin Definition - JAMAaji_jati_2005No ratings yet
- Acute Respiratory FailureDocument11 pagesAcute Respiratory FailureRicardoOswaldoValdiviesoValdiviesoNo ratings yet
- Acute Respiratory FailureDocument13 pagesAcute Respiratory FailureKartikaNo ratings yet
- Newly Proposed Diagnostic Criteria For Acute Respiratory Distress Syndrome - Does Inclusion of High Flow Nasal Cannula Solve The Problem? - PMCDocument13 pagesNewly Proposed Diagnostic Criteria For Acute Respiratory Distress Syndrome - Does Inclusion of High Flow Nasal Cannula Solve The Problem? - PMCThiago Antonio FontouraNo ratings yet
- Arterial Blood Gas Analysis: FK Uph May26, 2022Document52 pagesArterial Blood Gas Analysis: FK Uph May26, 2022FirmanHidayatNo ratings yet
- ARDS Berlin Definition JAMA2012Document8 pagesARDS Berlin Definition JAMA2012mondial200No ratings yet
- Arterial Blood Gas AnalysisDocument60 pagesArterial Blood Gas Analysismedico_bhalla100% (2)
- Respiratory Monitoring in The IcuDocument14 pagesRespiratory Monitoring in The IcuLorena DobrescuNo ratings yet
- Concept Map Complex Care 2017Document7 pagesConcept Map Complex Care 2017api-401537905No ratings yet
- Test Banks Gary PersingDocument35 pagesTest Banks Gary PersingAlexander Santiago ParelNo ratings yet
- ARBR 2806 Edit ReportDocument5 pagesARBR 2806 Edit ReportJosé Manuel Valencia GallardoNo ratings yet
- Clinical Findings of 104 Hospitalized Covid 19 Patients From Khyber Pakhtunkhwa Province 839Document8 pagesClinical Findings of 104 Hospitalized Covid 19 Patients From Khyber Pakhtunkhwa Province 839Anab Rehan TaseerNo ratings yet
- ARDS Meduri JAMA 1998Document8 pagesARDS Meduri JAMA 1998Rivaneide AmorimNo ratings yet
- Acute Respiratory Distress SyndromeDocument70 pagesAcute Respiratory Distress SyndromeAndrea Del Villar100% (1)
- Intra-Operative PEEP Vs ZEEPDocument37 pagesIntra-Operative PEEP Vs ZEEPMohamed RifanNo ratings yet
- 0bbamechanical VentilationDocument85 pages0bbamechanical VentilationKamal MohamedNo ratings yet