You might also like
- JURNAL DR - marzuki.BACA 2023Document36 pagesJURNAL DR - marzuki.BACA 2023iman prawiraNo ratings yet
- DifferentialDocument8 pagesDifferentialJorgeNo ratings yet
- Aspen Vs EspenDocument3 pagesAspen Vs EspeninoesienaNo ratings yet
- Nutrition Journal of Parenteral and Enteral: Less or More? Enteral Nutrition in Critically Ill Septic PatientsDocument4 pagesNutrition Journal of Parenteral and Enteral: Less or More? Enteral Nutrition in Critically Ill Septic PatientsMarco Antonio BravoNo ratings yet
- 1 s2.0 S2405457722000432 MainDocument7 pages1 s2.0 S2405457722000432 MainjvracuyaNo ratings yet
- Casa Er 2015Document12 pagesCasa Er 2015Anonymous h0DxuJTNo ratings yet
- Nutrition of The Critically Ill Patient and Effects of Implementing A Nutritional Support Algorithm in ICUDocument10 pagesNutrition of The Critically Ill Patient and Effects of Implementing A Nutritional Support Algorithm in ICUFildzah Aulia UlhaqNo ratings yet
- Clinical Impact of Prescribed Doses of Nutrients For Patients Exclusively Receiving Parenteral Nutrition in Japanese HospitalsDocument9 pagesClinical Impact of Prescribed Doses of Nutrients For Patients Exclusively Receiving Parenteral Nutrition in Japanese Hospitalsmarco marcoNo ratings yet
- Cocca 29 101Document7 pagesCocca 29 101Rasime Sevgi CenanNo ratings yet
- Post-ICU Nutrition The Neglected Side of Metabolic SupportDocument3 pagesPost-ICU Nutrition The Neglected Side of Metabolic SupportHubert PastasNo ratings yet
- Nutrients 15 03814Document18 pagesNutrients 15 03814Rasime Sevgi CenanNo ratings yet
- A Stepwise Enteral Nutrition Algorithm For Critically (Susan Dan Nilesh Mehta)Document7 pagesA Stepwise Enteral Nutrition Algorithm For Critically (Susan Dan Nilesh Mehta)NyomanGinaHennyKristiantiNo ratings yet
- Epidural HematomaDocument10 pagesEpidural HematomaNida Nur AmaliaNo ratings yet
- Nutrition Therapy in Critically Ill Patients A Review of Current Evidence For CliniciansDocument7 pagesNutrition Therapy in Critically Ill Patients A Review of Current Evidence For CliniciansangiolikkiaNo ratings yet
- ESPEN Guideline Clinical Nutrition in SurgeryDocument28 pagesESPEN Guideline Clinical Nutrition in SurgeryekalospratamaNo ratings yet
- ESPEN Guideline Clinical Nutrition in SurgeryDocument28 pagesESPEN Guideline Clinical Nutrition in SurgeryMicheline Tereza PiresNo ratings yet
- Combined Enteral Feeding and Total Parenteral Nutritional Support Improves Outcome in Surgical Intensive Care Unit PatientsDocument5 pagesCombined Enteral Feeding and Total Parenteral Nutritional Support Improves Outcome in Surgical Intensive Care Unit PatientsSiska KhairNo ratings yet
- Negative Impact of Hypocaloric Feeding and Energy Balance On Clinical Outcome in ICU PatientsDocument8 pagesNegative Impact of Hypocaloric Feeding and Energy Balance On Clinical Outcome in ICU PatientsDaniela HernandezNo ratings yet
- Impact of A Computerized InforDocument10 pagesImpact of A Computerized Inforsaya amirazNo ratings yet
- Persistent Critical Illness & Nutrition Considerations - JPEN 2024 (Viner)Document9 pagesPersistent Critical Illness & Nutrition Considerations - JPEN 2024 (Viner)Daniela QuirogaNo ratings yet
- Perioperative Nutrition in Extremely Preterm Infants Undergoing Surgery For Patent Ductus ArteriosusDocument12 pagesPerioperative Nutrition in Extremely Preterm Infants Undergoing Surgery For Patent Ductus ArteriosusOctavianus KevinNo ratings yet
- Early High Protein Intake and Mortality in Critically Ill ICU Patients With Low Skeletal Muscle Area and - DensityDocument10 pagesEarly High Protein Intake and Mortality in Critically Ill ICU Patients With Low Skeletal Muscle Area and - Densitylila_triNo ratings yet
- The Effect of Higher Protein Dosing in Critically Ill Patients With High Nutritional Risk (EFFORT Protein)Document9 pagesThe Effect of Higher Protein Dosing in Critically Ill Patients With High Nutritional Risk (EFFORT Protein)Laura LondoñoNo ratings yet
- MO S02 LecturaDocument9 pagesMO S02 LecturaCynthia Ramirez QuintanaNo ratings yet
- Preoperative Nutritional Support in Cancer Patients With No Clinical Signs of Malnutrition - Prospective Randomized Controlled TrialDocument6 pagesPreoperative Nutritional Support in Cancer Patients With No Clinical Signs of Malnutrition - Prospective Randomized Controlled TrialtttttNo ratings yet
- Clinical Nutrition: Original ArticleDocument8 pagesClinical Nutrition: Original ArticleCristina Correa SalazarNo ratings yet
- 1 s2.0 S0261561420301941 MainDocument8 pages1 s2.0 S0261561420301941 MainNatalia BeltranNo ratings yet
- Seguridad en CovidDocument6 pagesSeguridad en CovidedithNo ratings yet
- Nutrition Therapy and Critical Illness Practical GDocument10 pagesNutrition Therapy and Critical Illness Practical GVictoria PoNo ratings yet
- Optimal Timing For Introducing Enteral Nutrition in The Neonatal Intensive Care UnitDocument8 pagesOptimal Timing For Introducing Enteral Nutrition in The Neonatal Intensive Care UnitAnonymous 1EQutBNo ratings yet
- Enteral Nutrition in The Critically Ill Marik PDFDocument8 pagesEnteral Nutrition in The Critically Ill Marik PDFCami Cuevas VergaraNo ratings yet
- Research Open Access: Critical CareDocument9 pagesResearch Open Access: Critical Carerpgleblanc2No ratings yet
- Nutritional Management of The Critically Ill.29Document16 pagesNutritional Management of The Critically Ill.29Ririn Muthia ZukhraNo ratings yet
- CalorimetriaDocument7 pagesCalorimetriaEduardo GirónNo ratings yet
- PIIS240545772100245XDocument5 pagesPIIS240545772100245Xsulemi castañonNo ratings yet
- ESPEN Practical Guideline Home Enteral NutritionDocument21 pagesESPEN Practical Guideline Home Enteral NutritionJeanCarlosNo ratings yet
- How To Avoid Harm With Feeding CriticallyDocument9 pagesHow To Avoid Harm With Feeding CriticallyRejannedeOliveiraNo ratings yet
- Mortensen 2019 Proten Energy Intake Intervent HospitalizedDocument6 pagesMortensen 2019 Proten Energy Intake Intervent HospitalizedArina Nurul IhsaniNo ratings yet
- ESPEN Guideline - Clinical Nutrition in SurgeryDocument28 pagesESPEN Guideline - Clinical Nutrition in SurgeryyousorNo ratings yet
- Meta Analise CIDocument11 pagesMeta Analise CIInes MendonçaNo ratings yet
- Home Enteral Nutrition in Oncogeriatry Infusion Versus Energy NeedsDocument6 pagesHome Enteral Nutrition in Oncogeriatry Infusion Versus Energy NeedsHerald Scholarly Open AccessNo ratings yet
- ESPEN Guideline Clinical Nutrition in SurgeryDocument28 pagesESPEN Guideline Clinical Nutrition in SurgeryMeliSsa DanielaNo ratings yet
- Inicio de La Alimentacion Parenteral en El Niño Criticamente EnfermoDocument10 pagesInicio de La Alimentacion Parenteral en El Niño Criticamente EnfermoNATALIA LEMOS CALLENo ratings yet
- ESPEN Practical Guideline Clinical Nutrition in SurgeryDocument17 pagesESPEN Practical Guideline Clinical Nutrition in SurgeryMaríaJoséVegaNo ratings yet
- Children 09 01031Document12 pagesChildren 09 01031AIRA MARIE DOROTEONo ratings yet
- Nutrition in Critical Care: R. Chowdhury and S. LobazDocument6 pagesNutrition in Critical Care: R. Chowdhury and S. LobazVictoria PoNo ratings yet
- 1 SMDocument9 pages1 SMNi Putu Anita CandriNo ratings yet
- International Journal of Gerontology: Original ArticleDocument5 pagesInternational Journal of Gerontology: Original ArticleFitri RahmadaniNo ratings yet
- 1 s2.0 S222541101630181X MainDocument5 pages1 s2.0 S222541101630181X Mainsiska khairNo ratings yet
- Enteral Nutrition in The Critically Ill Myths And.24Document8 pagesEnteral Nutrition in The Critically Ill Myths And.24adinacomNo ratings yet
- Clinical Nutrition Guidelines for Parenteral Nutrition in Elderly PatientsDocument5 pagesClinical Nutrition Guidelines for Parenteral Nutrition in Elderly PatientsIvhajannatannisa KhalifatulkhusnulkhatimahNo ratings yet
- Enteral Feedings in Hospitalized Patients: Early Versus Delayed Enteral NutritionDocument7 pagesEnteral Feedings in Hospitalized Patients: Early Versus Delayed Enteral NutritionokipashaNo ratings yet
- Clinical Nutrition: Original ArticleDocument8 pagesClinical Nutrition: Original ArticleSiska KhairNo ratings yet
- ESPEN Guidelines On Parenteral Nutrition Surgery 2006Document9 pagesESPEN Guidelines On Parenteral Nutrition Surgery 2006Jorge OsorioNo ratings yet
- 9994CNR - CNR 7 48Document8 pages9994CNR - CNR 7 48dr.martynchukNo ratings yet
- s13054 022 04047 4Document13 pagess13054 022 04047 4Mays OthmanNo ratings yet
- Enteral Nutrition: What The Dietitian Prescribes Is Not What The Burn Patient Gets!Document9 pagesEnteral Nutrition: What The Dietitian Prescribes Is Not What The Burn Patient Gets!anjarwatiNo ratings yet
- ESPEN Guideline Clinical Nutrition in Surgery 2017Document28 pagesESPEN Guideline Clinical Nutrition in Surgery 2017Jorge OsorioNo ratings yet
- ESPEN Guidelines On (Enteral Nutrition) Intensive CareDocument14 pagesESPEN Guidelines On (Enteral Nutrition) Intensive Careputugede_ict2007100% (1)
- Micronutrients and Risk of Parkinson's Disease: A Systematic ReviewDocument11 pagesMicronutrients and Risk of Parkinson's Disease: A Systematic Reviewiman prawiraNo ratings yet
- Jurnal Reading PPT FixxeddDocument36 pagesJurnal Reading PPT Fixxeddiman prawiraNo ratings yet
- Assessing The Relationship Between Dietaryintake Hygienic Practices and ProDocument12 pagesAssessing The Relationship Between Dietaryintake Hygienic Practices and Proiman prawiraNo ratings yet
- Obesity - 2022 - Christoffersen - Beyond Appetite Regulation Targeting Energy Expenditure Fat Oxidation and Lean MassDocument18 pagesObesity - 2022 - Christoffersen - Beyond Appetite Regulation Targeting Energy Expenditure Fat Oxidation and Lean Massiman prawiraNo ratings yet
- Consumption of Broccoli Sprouts Attenuatesintracellular p38 Map Kinase andDocument7 pagesConsumption of Broccoli Sprouts Attenuatesintracellular p38 Map Kinase andiman prawiraNo ratings yet
- Micronutrients and Risk of Parkinson's Disease: A Systematic ReviewDocument11 pagesMicronutrients and Risk of Parkinson's Disease: A Systematic Reviewiman prawiraNo ratings yet
- Drug Enutrient Interactions in Renal Failure: Raimund HirschbergDocument10 pagesDrug Enutrient Interactions in Renal Failure: Raimund Hirschbergiman prawiraNo ratings yet
- 2016 Article 99Document9 pages2016 Article 99iman prawiraNo ratings yet
- Artichoke Leaf Extract for Oxidative Stress in Metabolic SyndromeDocument31 pagesArtichoke Leaf Extract for Oxidative Stress in Metabolic Syndromeiman prawiraNo ratings yet
- Aliyani Association Between Vitamin D Deficiency and Psoriasis A CasecontrolstudyDocument5 pagesAliyani Association Between Vitamin D Deficiency and Psoriasis A CasecontrolstudyAzmi FadhlihNo ratings yet
- Vitamin D Receptor Genotypes Ultraviolet RadiationDocument8 pagesVitamin D Receptor Genotypes Ultraviolet Radiationiman prawiraNo ratings yet
- Research: Diet and Non-Hodgkin's Lymphoma RiskDocument12 pagesResearch: Diet and Non-Hodgkin's Lymphoma RiskJose AbadiaNo ratings yet
- Albuminuria Levels in Diabetic Patients With and Without CHDDocument5 pagesAlbuminuria Levels in Diabetic Patients With and Without CHDRindaBabaroNo ratings yet
- Ch11 Nutrition Therapy PDFDocument16 pagesCh11 Nutrition Therapy PDFiman prawiraNo ratings yet
- 0 - Nutrition Therapy For Hemiparesis of Non Hemorrhagic StrokeDocument1 page0 - Nutrition Therapy For Hemiparesis of Non Hemorrhagic Strokeiman prawiraNo ratings yet
- 1806 9282 Ramb 64 07 0643 PDFDocument6 pages1806 9282 Ramb 64 07 0643 PDFiman prawiraNo ratings yet
- Digestive Involvement in Retroperitoneal FibrosisDocument4 pagesDigestive Involvement in Retroperitoneal Fibrosisiman prawiraNo ratings yet
- Diet and Respiratory DiseaseDocument4 pagesDiet and Respiratory Diseaseiman prawiraNo ratings yet
- Digestive Involvement in Retroperitoneal FibrosisDocument4 pagesDigestive Involvement in Retroperitoneal Fibrosisiman prawiraNo ratings yet
- Cancer CahexiaDocument9 pagesCancer Cahexiaiman prawiraNo ratings yet
- A Meta-Analysis of N-3 Polyunsaturated Fatty Acids Effects OnDocument11 pagesA Meta-Analysis of N-3 Polyunsaturated Fatty Acids Effects Oniman prawiraNo ratings yet
- Diet and Respiratory DiseaseDocument4 pagesDiet and Respiratory Diseaseiman prawiraNo ratings yet
- Barriers To ListeningDocument2 pagesBarriers To ListeningHammad Ali ShahzadNo ratings yet
- Evaluation of The Flow Rate of 3 Endodontic Sealers: Sealer 26, AH Plus, and MTA ObturaDocument3 pagesEvaluation of The Flow Rate of 3 Endodontic Sealers: Sealer 26, AH Plus, and MTA ObturaSai KarthikNo ratings yet
- Planning ProcessDocument9 pagesPlanning ProcessSimran JosanNo ratings yet
- Photob 2022 0067Document10 pagesPhotob 2022 0067Marilene da Conceicao Felix da SilvaNo ratings yet
- Pestle Analysis On Reliance Industries: MBA Student - DBS Module International ManagementDocument15 pagesPestle Analysis On Reliance Industries: MBA Student - DBS Module International ManagementshubhamNo ratings yet
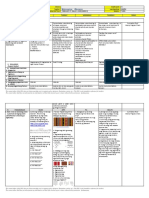
- MAPEH Daily Lesson LogDocument11 pagesMAPEH Daily Lesson LogMARTIN YUI LOPEZNo ratings yet
- Management: Fourteenth EditionDocument46 pagesManagement: Fourteenth EditionAmjad J AliNo ratings yet
- 1 Caixin Lei PSY 2012 General PsychologyDocument2 pages1 Caixin Lei PSY 2012 General PsychologyKaty LeiNo ratings yet
- Training and DevelopmentDocument2 pagesTraining and DevelopmentBeing Rohit ThakurNo ratings yet
- Graduation Certificates: Speech TherapyDocument10 pagesGraduation Certificates: Speech Therapyliza khalilNo ratings yet
- Presentation 1Document6 pagesPresentation 1Joarlin BianesNo ratings yet
- 4.1.10 Practice Grammar FeedbackDocument10 pages4.1.10 Practice Grammar FeedbackbaileyNo ratings yet
- VA - DQA Specialist IBTCIDocument5 pagesVA - DQA Specialist IBTCIT. Woibah SuwoNo ratings yet
- BS BuzzDocument10 pagesBS BuzzBS Central, Inc. "The Buzz"No ratings yet
- Yoga e CogniçãoDocument6 pagesYoga e CogniçãoMessias FilhoNo ratings yet
- Quality Life Scale PDFDocument7 pagesQuality Life Scale PDFFayza RihastaraNo ratings yet
- Mom 202108003Document2 pagesMom 202108003Ckucku AranetaNo ratings yet
- SV The Coronation of King Charles IIIDocument9 pagesSV The Coronation of King Charles IIIMaria GromovaNo ratings yet
- This Study Determined The Effectiveness of Mnemonics in Improving Memory Among Nursing Students in GCON, BikanerDocument3 pagesThis Study Determined The Effectiveness of Mnemonics in Improving Memory Among Nursing Students in GCON, BikanerNaveen ShrivasNo ratings yet
- College of Liberal Arts University of LuzonDocument9 pagesCollege of Liberal Arts University of LuzonChristianne Joyse MerreraNo ratings yet
- Amit Surati 29Document3 pagesAmit Surati 29api-286592025No ratings yet
- Sharpen The Saw - Activity WorksheetDocument6 pagesSharpen The Saw - Activity WorksheetClarence Tan100% (1)
- AF Catheter AblationDocument37 pagesAF Catheter AblationSnehal JayaramNo ratings yet
- Post-Test Sas 13, 14 & 15 Nur 151 Cooa A4: Questions 1 To 10Document2 pagesPost-Test Sas 13, 14 & 15 Nur 151 Cooa A4: Questions 1 To 10Sistine Rose LabajoNo ratings yet
- Capillary Blood Glucose Performance Checklist: Numerical Rating Adjectival Description DescriptionDocument2 pagesCapillary Blood Glucose Performance Checklist: Numerical Rating Adjectival Description DescriptionAngeline NavarroNo ratings yet
- Trainee's Record Book SWBLDocument12 pagesTrainee's Record Book SWBLaaronjules100% (2)
- Culture's Influence on Ethics in BusinessDocument4 pagesCulture's Influence on Ethics in Businesssotiredofrepeating0% (2)
- Government Issues Relief Guidelines for Victims of AtrocitiesDocument4 pagesGovernment Issues Relief Guidelines for Victims of AtrocitiesDept . WD&CW Andhra PradeshNo ratings yet
- Hemodynamic Effects of Dexmedetomidine vs ClonidineDocument12 pagesHemodynamic Effects of Dexmedetomidine vs ClonidinezzzzNo ratings yet
- Role Play Script BHS INGGRISDocument6 pagesRole Play Script BHS INGGRISardiyantiNo ratings yet