You might also like
- Length Tension Testing Book 1, Lower Quadrant: A Workbook of Manual Therapy TechniquesFrom EverandLength Tension Testing Book 1, Lower Quadrant: A Workbook of Manual Therapy TechniquesRating: 3.5 out of 5 stars3.5/5 (3)
- PT Journal Musclel ActivityDocument8 pagesPT Journal Musclel ActivityKarthigaMurugesanNo ratings yet
- Hamstring OM 21Document5 pagesHamstring OM 21Dr Ahmed NabilNo ratings yet
- An Electromyographic Analysis of Trunk and Hip Extensor Muscles During Bridging Exercises - Effect of Voluntary Control of The Pelvic TiltDocument3 pagesAn Electromyographic Analysis of Trunk and Hip Extensor Muscles During Bridging Exercises - Effect of Voluntary Control of The Pelvic TiltNicolás ManonniNo ratings yet
- An Electromyographic Evaluation of Subdividing Active-Assistive Shoulder Elevation ExercisesDocument9 pagesAn Electromyographic Evaluation of Subdividing Active-Assistive Shoulder Elevation ExercisesJuliano BritoNo ratings yet
- An Electromyographic Analysis of Trunk and Hip Extensor Muscles During Bridging Exercises - Effect of Voluntary Control of The Pelvic TiltDocument3 pagesAn Electromyographic Analysis of Trunk and Hip Extensor Muscles During Bridging Exercises - Effect of Voluntary Control of The Pelvic TiltNicolás ManonniNo ratings yet
- December2006RRHardwickDocument8 pagesDecember2006RRHardwickHaile Mariam González GarcíaNo ratings yet
- Contraccion TrunkDocument5 pagesContraccion TrunkSaira Camila Osso SanchezNo ratings yet
- Running MechanicsDocument10 pagesRunning MechanicsPilarRubioFernándezNo ratings yet
- Elastico No OmbrosDocument9 pagesElastico No OmbrosallanboxeNo ratings yet
- Thibordee2014 1 PDFDocument6 pagesThibordee2014 1 PDFMohamad Gilang Harry HNo ratings yet
- The Effects of Kinesio Taping On Quadriceps Strenth During Isokinetic Exercise in Healthy Non-Athlete WomenDocument6 pagesThe Effects of Kinesio Taping On Quadriceps Strenth During Isokinetic Exercise in Healthy Non-Athlete WomenionNo ratings yet
- PMID10569366Document8 pagesPMID10569366Koay WeiNo ratings yet
- Brazilian Journal of Physical TherapyDocument10 pagesBrazilian Journal of Physical TherapyLuis DavidNo ratings yet
- Muscles Activation During Forward LungeDocument8 pagesMuscles Activation During Forward LungeAinnur FitriyaNo ratings yet
- Quantitative Analysis of The Relative Effectiveness of 3 Iliotibial Band StretchesDocument4 pagesQuantitative Analysis of The Relative Effectiveness of 3 Iliotibial Band Stretchessalthill01No ratings yet
- The Effects of Kinesio-Taping On Quadriceps Strength During Isokinetic Exercise in Healthy Non Athlete WomenDocument6 pagesThe Effects of Kinesio-Taping On Quadriceps Strength During Isokinetic Exercise in Healthy Non Athlete WomenSurya DiatmikaNo ratings yet
- Pullover PDFDocument5 pagesPullover PDFRosaneLacerdaNo ratings yet
- 13 Marchetti 380 384 Pullover Copia 3193891071Document5 pages13 Marchetti 380 384 Pullover Copia 3193891071Angelica GarciaNo ratings yet
- Ejercicios Cadera TroncoDocument9 pagesEjercicios Cadera TroncoNicol Jerez ParraNo ratings yet
- Role of The Cervical and Lumbar Proprioceptors During SteppingDocument16 pagesRole of The Cervical and Lumbar Proprioceptors During SteppingFrancisco Vicent PachecoNo ratings yet
- Emg Deltoide Diferentes Exercicios Silveira Lima 2013 PDFDocument5 pagesEmg Deltoide Diferentes Exercicios Silveira Lima 2013 PDFAlexandreNo ratings yet
- Lower-Extremity Muscle Activation During The Star Excursion Balance TestsDocument12 pagesLower-Extremity Muscle Activation During The Star Excursion Balance TestsAZERNo ratings yet
- مقاله اسکاتDocument7 pagesمقاله اسکاتZahra BahadoriNo ratings yet
- Ajsm Serratus Anterior Rehab ExercisesDocument9 pagesAjsm Serratus Anterior Rehab ExercisesBrandon HeatNo ratings yet
- Differences in Muscle Shoulder External Rotation in Open Kinetic Chain and Closed Kinetic Chain Exercises PDFDocument3 pagesDifferences in Muscle Shoulder External Rotation in Open Kinetic Chain and Closed Kinetic Chain Exercises PDFLeonardiniNo ratings yet
- Comparison Electromyographic Activit During Open: ClosedDocument10 pagesComparison Electromyographic Activit During Open: ClosedFernando WagnerNo ratings yet
- Effect of Isometric Horizontal Abduction On Pectoralis Major and Serratus AnteriorDocument7 pagesEffect of Isometric Horizontal Abduction On Pectoralis Major and Serratus AnteriorRudolfGerNo ratings yet
- Research Article Biomechanics Analysis On Muscle Activation During Jumping Jack ExerciseDocument8 pagesResearch Article Biomechanics Analysis On Muscle Activation During Jumping Jack ExerciseIsen HausNo ratings yet
- Effects Prolonged Sitting On Passive Flex I On StiffnessDocument10 pagesEffects Prolonged Sitting On Passive Flex I On StiffnessCharlie HigginsNo ratings yet
- J Jelekin 2014 06 002 PDFDocument38 pagesJ Jelekin 2014 06 002 PDFRommel AndresNo ratings yet
- Obesity CuadricepsDocument5 pagesObesity CuadricepsGonzalo Aguayo AlcayagaNo ratings yet
- Effect of Repetitive Biphasic Muscle Electrostimulation Training On Vertical Jump Performances in Female Volleyball PlayersDocument17 pagesEffect of Repetitive Biphasic Muscle Electrostimulation Training On Vertical Jump Performances in Female Volleyball PlayersMARIA RESENDENo ratings yet
- Manual Therapy: Original ArticleDocument5 pagesManual Therapy: Original ArticleCleber PimentaNo ratings yet
- CathDean (1999) TrainingsittingbalanceIIDocument7 pagesCathDean (1999) TrainingsittingbalanceIIAlyssa TangNo ratings yet
- The Influence of Initial Posture On The Sit-To-Stand MovementDocument6 pagesThe Influence of Initial Posture On The Sit-To-Stand MovementshodhgangaNo ratings yet
- Influence of GenderDocument10 pagesInfluence of Gendersateesh83No ratings yet
- Exaggerated Interlimb Neural Coupling Following Stroke: Tiffany L. Kline, Brian D. Schmit and Derek G. KamperDocument11 pagesExaggerated Interlimb Neural Coupling Following Stroke: Tiffany L. Kline, Brian D. Schmit and Derek G. KamperArup KuntiNo ratings yet
- Situp 7Document8 pagesSitup 7LISTIA NURBAETINo ratings yet
- Dickie 2016Document28 pagesDickie 2016FranciscoNo ratings yet
- Spinal Myo After InjuryDocument12 pagesSpinal Myo After InjuryVincentius Michael WilliantoNo ratings yet
- Biomechanical Analysis of The Standing Long Jump: W - L W, J - H W, H - T L, G - J WDocument4 pagesBiomechanical Analysis of The Standing Long Jump: W - L W, J - H W, H - T L, G - J W陳俞良No ratings yet
- Cavagna On Energy Exchanges in Walking and RunningDocument15 pagesCavagna On Energy Exchanges in Walking and RunningLaboratory in the WildNo ratings yet
- A Study of The Stance LimbDocument5 pagesA Study of The Stance LimbayadandiaNo ratings yet
- Effects of Electrical Muscle Stimulation On Body Composition, Muscle StrengthDocument8 pagesEffects of Electrical Muscle Stimulation On Body Composition, Muscle StrengthphuawlNo ratings yet
- Gefen Et Al. - 2002 - Analysis of Muscular Fatigue and Foot Stability During High-Heeled GaitDocument8 pagesGefen Et Al. - 2002 - Analysis of Muscular Fatigue and Foot Stability During High-Heeled GaitAwatef FituriNo ratings yet
- Case History and Successful Therapy of Toe WalkingDocument8 pagesCase History and Successful Therapy of Toe WalkingSaraNo ratings yet
- Dynamic Joint and Muscle Forces During Knee Isokinetic ExerciseDocument8 pagesDynamic Joint and Muscle Forces During Knee Isokinetic ExerciseFabiano LacerdaNo ratings yet
- 2020 Berckmans Finewire AJSMDocument7 pages2020 Berckmans Finewire AJSMMariaNo ratings yet
- 2020 Berckmans Finewire AJSMDocument7 pages2020 Berckmans Finewire AJSMLívia PogettiNo ratings yet
- Peroneal Reaction Times and Eversion Motor Response in Healthy and Unstable AnklesDocument6 pagesPeroneal Reaction Times and Eversion Motor Response in Healthy and Unstable AnklesPatricia BortolottiNo ratings yet
- Hamstring Muscle Strain Treated by Mobilizing The Sacroiliac JointDocument4 pagesHamstring Muscle Strain Treated by Mobilizing The Sacroiliac JointKarthik BhashyamNo ratings yet
- Articulo #30Document8 pagesArticulo #30LAURA CAMILA CUBILLOS VILLAMILNo ratings yet
- 13 Marchetti 380 384pulloverDocument6 pages13 Marchetti 380 384pullovercderosasNo ratings yet
- 29 - Jpts 2017 341Document4 pages29 - Jpts 2017 341Rafii KhairuddinNo ratings yet
- Escamilla 2001Document15 pagesEscamilla 2001Cristina VicenteNo ratings yet
- Paper 1Document9 pagesPaper 1sbarahonacamilaNo ratings yet
- 2016 Influence of Scapular Position On The CORE Musculature Activation in The Prone Plank ExerciseDocument23 pages2016 Influence of Scapular Position On The CORE Musculature Activation in The Prone Plank ExerciseFrancisco Antonó Castro WeithNo ratings yet
- Dynamic Stretching: The Revolutionary New Warm-up Method to Improve Power, Performance and Range of MotionFrom EverandDynamic Stretching: The Revolutionary New Warm-up Method to Improve Power, Performance and Range of MotionRating: 5 out of 5 stars5/5 (1)
- Jenis Fraktur IstimewaDocument14 pagesJenis Fraktur IstimewaUllya AisyafitriNo ratings yet
- ACL Reconstruction SurgeryDocument8 pagesACL Reconstruction Surgeryjohn hagisNo ratings yet
- Towards Realising Wearable Exoskeletons For Elderly PeopleDocument6 pagesTowards Realising Wearable Exoskeletons For Elderly PeopleRatna SambhavNo ratings yet
- Taping Reference Sheet-3815621Document3 pagesTaping Reference Sheet-3815621api-383568582No ratings yet
- Rehab Individual (Achilles Tendon Injury) - Raihan Naqibah Binti Mohamed (2021515847)Document21 pagesRehab Individual (Achilles Tendon Injury) - Raihan Naqibah Binti Mohamed (2021515847)Jalal NasirNo ratings yet
- Common Gait DeviationsDocument4 pagesCommon Gait Deviationsswimgrl54100% (2)
- The EVOLUTION of The HUMAN FOOTDocument12 pagesThe EVOLUTION of The HUMAN FOOTpetcudanielNo ratings yet
- Lecture 1 TF BiomechanicsDocument63 pagesLecture 1 TF BiomechanicsAlfred JacksonNo ratings yet
- Groin DissectionDocument19 pagesGroin Dissectiondewiswahyu100% (1)
- Vibram FiveFingersDocument6 pagesVibram FiveFingersroberto jimenezNo ratings yet
- TRIANGLES OF THE BODY KEY ANATOMICAL LANDMARKSDocument3 pagesTRIANGLES OF THE BODY KEY ANATOMICAL LANDMARKSMei Bejerano - Roldan100% (1)
- Penatalaksanaan Fisioterapi Pada KondisiDocument10 pagesPenatalaksanaan Fisioterapi Pada KondisiImam Ibrahim22No ratings yet
- CTEVDocument61 pagesCTEVSylvia LoongNo ratings yet
- Deep venous system of the lower extremity: new nomenclatureDocument12 pagesDeep venous system of the lower extremity: new nomenclatureEngie VersabethNo ratings yet
- The Lower ExtremityDocument24 pagesThe Lower ExtremityAlifia AzzahraNo ratings yet
- JUST MEDICAL - Product Catalog - Hip&Knee - Specs - OE - 202206Document41 pagesJUST MEDICAL - Product Catalog - Hip&Knee - Specs - OE - 202206Jack ZhangNo ratings yet
- Portofolio FatmaDocument12 pagesPortofolio FatmafitriaokNo ratings yet
- Repertory To Hering's Condensed Materia MedicaDocument450 pagesRepertory To Hering's Condensed Materia MedicaGhica Gheorghiu100% (1)
- Hallux Valgus: Causes, Symptoms and TreatmentDocument16 pagesHallux Valgus: Causes, Symptoms and TreatmentucssNo ratings yet
- Ankle Block: Dr. S. Parthasarathy MD., DA., DNB, MD (Acu), Dip. Diab. DCA, Dip. Software StatisticsDocument27 pagesAnkle Block: Dr. S. Parthasarathy MD., DA., DNB, MD (Acu), Dip. Diab. DCA, Dip. Software StatisticsRajNo ratings yet
- Tibia Plateau Fractures Final EditDocument96 pagesTibia Plateau Fractures Final EditPRASHANTH H KNo ratings yet
- Working With Hammertoes: The Foot (PT I) (Myofascial Techniques)Document4 pagesWorking With Hammertoes: The Foot (PT I) (Myofascial Techniques)Advanced-Trainings.com100% (5)
- Goniometer Placement Guide for 20 Joint MotionsDocument4 pagesGoniometer Placement Guide for 20 Joint MotionsMichelle Renee AquinoNo ratings yet
- Comparing VMO and Gluteus Medius Strengthening Exercises to Normalize Q Angle in Knee OADocument67 pagesComparing VMO and Gluteus Medius Strengthening Exercises to Normalize Q Angle in Knee OAJigyasa JuyalNo ratings yet
- Vonstein Some Reflections On Maximum Speed Sprinting TechniqueDocument8 pagesVonstein Some Reflections On Maximum Speed Sprinting TechniqueZachary LeeNo ratings yet
- Bones of The FootDocument23 pagesBones of The FootZaid AbdulqadirNo ratings yet
- Mulligan Concept IFI Kudus, 29 Oktober 2017-1Document84 pagesMulligan Concept IFI Kudus, 29 Oktober 2017-1Ilham Sii Pendekar Biru100% (1)
- Self Management - Hip Muscle TrainingDocument2 pagesSelf Management - Hip Muscle Trainingfarrelly14100% (2)
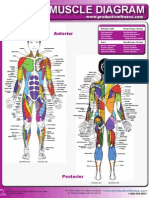
- Female Muscle DiagramDocument1 pageFemale Muscle DiagrammakukikiNo ratings yet
- AO Classification 2018 FootDocument12 pagesAO Classification 2018 FootIvanNo ratings yet