You might also like
- Dr.-andrew-moulden-EVERY VACCINE PRODUCES HARMDocument123 pagesDr.-andrew-moulden-EVERY VACCINE PRODUCES HARMPollyana Furtado Junqueira50% (4)
- Wash Rinse Sanitize PosterDocument1 pageWash Rinse Sanitize PosterAlexis OrganisNo ratings yet
- Adverse Effects Pine Bark ExtractDocument4 pagesAdverse Effects Pine Bark ExtractAvelox FloxNo ratings yet
- 7es Science Lesson Plan ExampleDocument9 pages7es Science Lesson Plan ExampleKing GarciaNo ratings yet
- Stryker 1488Document10 pagesStryker 1488Victor Hugo Lazarte Gonzalez100% (1)
- Document Name Document Number Date Created Date Implemented Name: Designation: Signature: Name: Designation: SignatureDocument49 pagesDocument Name Document Number Date Created Date Implemented Name: Designation: Signature: Name: Designation: Signaturecorona virusNo ratings yet
- Cleaning and SanitizingDocument30 pagesCleaning and SanitizingAngie Filler100% (3)
- Hope RequirementsDocument7 pagesHope Requirementscorona virusNo ratings yet
- Self-Learning Module in Tle-He Wellness Massage GRADE 7/8 Week 2 Maintain Tools and EquipmentDocument11 pagesSelf-Learning Module in Tle-He Wellness Massage GRADE 7/8 Week 2 Maintain Tools and EquipmentElaeca AbenNo ratings yet
- Business Research Methodology: Group No 2Document10 pagesBusiness Research Methodology: Group No 2Jojo DiazNo ratings yet
- Care Cleaning Disinfection and SterilizationDocument16 pagesCare Cleaning Disinfection and SterilizationCHARMAINE FEARL FABROSNo ratings yet
- Government Regulation No. 86 - 2019 On Food Safety PDFDocument49 pagesGovernment Regulation No. 86 - 2019 On Food Safety PDFAndi WibowoNo ratings yet
- Solution List and ClassificationDocument7 pagesSolution List and ClassificationckNo ratings yet
- Surface Cleaning Protocols For LR OT PNC WardsDocument8 pagesSurface Cleaning Protocols For LR OT PNC WardsArchana SahuNo ratings yet
- Hedge HicnDocument8 pagesHedge HicnSubramanya Seeta Ram PrasadNo ratings yet
- Sterilization: Psysical Method Thermal Chemical MethodDocument19 pagesSterilization: Psysical Method Thermal Chemical MethodCh WilungchapbouNo ratings yet
- Hospital Infection ControlDocument13 pagesHospital Infection ControlNazaqat FarooqNo ratings yet
- Disinfectant Available Chlorine Required Chlorine Required Chlorine Contact Period Amount of Disinfectant To Be Dissolved in 1 LTR of WaterDocument3 pagesDisinfectant Available Chlorine Required Chlorine Required Chlorine Contact Period Amount of Disinfectant To Be Dissolved in 1 LTR of WaterAsmi MohamedNo ratings yet
- Surface Cleaning in Gendral Ward Question 5Document8 pagesSurface Cleaning in Gendral Ward Question 5Keerthi AnbazhaganNo ratings yet
- Sterilization ProtocolDocument6 pagesSterilization ProtocolChellamani UmakanthanNo ratings yet
- Nail Salon BrochureDocument2 pagesNail Salon BrochureKrizza BalanganNo ratings yet
- A Practical Manual On Visual Screening For Cervical NeoplasiaDocument1 pageA Practical Manual On Visual Screening For Cervical NeoplasiaDeborah AkanyareNo ratings yet
- Cleaning and Disinfecting Full-Face Masks: Procedures and Specifications (Machine and Manual)Document6 pagesCleaning and Disinfecting Full-Face Masks: Procedures and Specifications (Machine and Manual)ieki aiainNo ratings yet
- Disinfection: DR - NandkumarDocument19 pagesDisinfection: DR - NandkumarCCMP dr waruNo ratings yet
- Nebulized Hypertonic Saline: Use of This Medicine How Do I Prepare The Hypertonic Saline Solution?Document3 pagesNebulized Hypertonic Saline: Use of This Medicine How Do I Prepare The Hypertonic Saline Solution?Marco GeraçãoNo ratings yet
- Cleaning Guide WA FlexiPort CuffsDocument1 pageCleaning Guide WA FlexiPort CuffsShahid HasanNo ratings yet
- Hospital Housekeeping IpcDocument33 pagesHospital Housekeeping IpcBrian VargasNo ratings yet
- ChromogenicFFPE ProtocolDocument3 pagesChromogenicFFPE ProtocolpeuterNo ratings yet
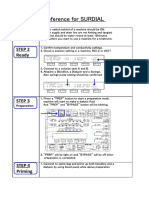
- Quick Reference For SURDIAL: Step 1 Confirm Step 2 ReadyDocument3 pagesQuick Reference For SURDIAL: Step 1 Confirm Step 2 ReadyDuglas Camilo Cediel RuizNo ratings yet
- Revised Guidelines Home Isolation 4Document14 pagesRevised Guidelines Home Isolation 4Vaishakh NairNo ratings yet
- Total Dissolved Solids by Gravimetric Determination: AMBL-105-BDocument6 pagesTotal Dissolved Solids by Gravimetric Determination: AMBL-105-BRoger YapNo ratings yet
- Hand Sanitisers KKS WHO 09062020 V 1Document47 pagesHand Sanitisers KKS WHO 09062020 V 1ew1 rNo ratings yet
- Cleaning and Sanitation - KitchenDocument23 pagesCleaning and Sanitation - Kitchensanju osNo ratings yet
- RP 09 - Respiration in Single Celled OrganismsDocument3 pagesRP 09 - Respiration in Single Celled OrganismsHailey WongNo ratings yet
- Operating Instructions: Dishwasher GV67260Document32 pagesOperating Instructions: Dishwasher GV67260Jessica RiveraNo ratings yet
- Food and Satety SanitationDocument7 pagesFood and Satety SanitationMary ann DeniegaNo ratings yet
- Conv - INIFU SunMed Conventional Reusable Laryngoscope Rev.2Document2 pagesConv - INIFU SunMed Conventional Reusable Laryngoscope Rev.2Maria Jose Marin Castaño100% (1)
- Handwashing FlyerDocument1 pageHandwashing Flyerapi-735758255No ratings yet
- Instrument Processing NDocument26 pagesInstrument Processing Nermias UmerNo ratings yet
- TSS Procedure PDFDocument6 pagesTSS Procedure PDFSusi MulyaniNo ratings yet
- Disinfecting Your HomeDocument3 pagesDisinfecting Your HomeMichelle O'NeillNo ratings yet
- Module 3 and 4Document16 pagesModule 3 and 4MOHD ROSNIZAM BIN MOHD YUSOFF MoeNo ratings yet
- AntisepticsDocument11 pagesAntisepticsriyasavlaNo ratings yet
- Guidelines at Odisha Hotels, EcoTourism, Resorts, PropertiesDocument14 pagesGuidelines at Odisha Hotels, EcoTourism, Resorts, PropertiesGD CONSULTANCYNo ratings yet
- Bac To Basics: Benzalkonium Chloride 10% ConcentrateDocument7 pagesBac To Basics: Benzalkonium Chloride 10% ConcentrateAqui GacusanNo ratings yet
- Technical DataDocument4 pagesTechnical Datakevinmendez2009No ratings yet
- Opaster Anios Fiche Technique 00000 enDocument2 pagesOpaster Anios Fiche Technique 00000 enArwil Fadillah100% (2)
- Tissue Culture SOPDocument12 pagesTissue Culture SOPManoj Kumar pandreNo ratings yet
- Linen S: By: Group 2 Xymon, Jade, Jared, Tyron, Jackilyn, Katie and ElijahDocument9 pagesLinen S: By: Group 2 Xymon, Jade, Jared, Tyron, Jackilyn, Katie and ElijahBatong Jansen BryleNo ratings yet
- Disinfecting Building Facility HDocument3 pagesDisinfecting Building Facility Hhaykal2robotNo ratings yet
- Esteer ProductsDocument12 pagesEsteer ProductsRaisa EndahNo ratings yet
- Home Quarantine Guideline For Home Confinee enDocument1 pageHome Quarantine Guideline For Home Confinee enLoulou Von SpielNo ratings yet
- Sterlization ProtocolsDocument10 pagesSterlization ProtocolsSarathchandran BalachandranNo ratings yet
- 81r RCgkADLDocument11 pages81r RCgkADLlimonNo ratings yet
- Cleaning and Disinfecting Your Home: How To Clean and DisinfectDocument6 pagesCleaning and Disinfecting Your Home: How To Clean and DisinfectStephenNo ratings yet
- Safelight: Scope AdaptersDocument214 pagesSafelight: Scope AdaptersLuis Arturo Tavera ParedesNo ratings yet
- Gehc Care Card Tee Probe Care CardDocument2 pagesGehc Care Card Tee Probe Care CardIqra ChuhanNo ratings yet
- DisinfectionDocument30 pagesDisinfectionBabita PatnaikNo ratings yet
- Cleaning - Important!: Once A WeekDocument1 pageCleaning - Important!: Once A WeekcozerNo ratings yet
- Operating and Installation Instructions: Wash&dry 10D52 Wash&dry 12D52Document67 pagesOperating and Installation Instructions: Wash&dry 10D52 Wash&dry 12D52ПРЕДРАГNo ratings yet
- Nail Care Lesson 2Document5 pagesNail Care Lesson 2Tin TinNo ratings yet
- Nail Care Lesson 2Document5 pagesNail Care Lesson 2Tin TinNo ratings yet
- Cleaning Guide: Banking HardwareDocument1 pageCleaning Guide: Banking HardwareAtendra ShresthaNo ratings yet
- Hydris Hydris™: Disinfectant CleanerDocument1 pageHydris Hydris™: Disinfectant Cleanernikors65No ratings yet
- Rockstar System InstructionsDocument8 pagesRockstar System InstructionsSilvio DTNo ratings yet
- Easy Peasy Homemade Sanitizer Wipes: A Quick Guide with Visuals for Making Disposable Sanitizing Wipes Against MicrobesFrom EverandEasy Peasy Homemade Sanitizer Wipes: A Quick Guide with Visuals for Making Disposable Sanitizing Wipes Against MicrobesNo ratings yet
- Registered Office: 3 CIN: L17110MH1973PLC019786: Floor, Maker Chambers IV, 222, Nariman Point, Mumbai 400 021Document2 pagesRegistered Office: 3 CIN: L17110MH1973PLC019786: Floor, Maker Chambers IV, 222, Nariman Point, Mumbai 400 021corona virusNo ratings yet
- Security Services Tender - IKDRC (New)Document87 pagesSecurity Services Tender - IKDRC (New)corona virusNo ratings yet
- Laboratory Section:: Answer: Yes Remarks: NC: NC DetailsDocument22 pagesLaboratory Section:: Answer: Yes Remarks: NC: NC Detailscorona virusNo ratings yet
- Unit 2-NotesDocument10 pagesUnit 2-NotesStudy StudyNo ratings yet
- Theories of Personality 3 (Alfred Adler)Document42 pagesTheories of Personality 3 (Alfred Adler)Anne Jeanneth DiazNo ratings yet
- Coaching PhilosophyDocument24 pagesCoaching PhilosophySim BuenNo ratings yet
- SOAL English USBN 2022Document10 pagesSOAL English USBN 2022Amrina RosyadaNo ratings yet
- Asian American Pacific Islander Communities and Mental HealthDocument10 pagesAsian American Pacific Islander Communities and Mental Healthapi-581842870No ratings yet
- SA 1055 RH Fire Safety 2014Document7 pagesSA 1055 RH Fire Safety 2014Salma AbedNo ratings yet
- Running Techniques 1Document5 pagesRunning Techniques 1Bill LeeNo ratings yet
- HSE-302 Water Management StandardDocument9 pagesHSE-302 Water Management StandardLck OfficialNo ratings yet
- BioinstrumentationDocument394 pagesBioinstrumentationapi-370230280% (5)
- Resume - 2022 07 03 095726Document4 pagesResume - 2022 07 03 095726Nessa LarrierNo ratings yet
- Personality Attributes of A Professional Counselor and Its Impact On Counseling Process A ReviewDocument9 pagesPersonality Attributes of A Professional Counselor and Its Impact On Counseling Process A ReviewAnaghaNo ratings yet
- CTD Module 4 - SafetyDocument113 pagesCTD Module 4 - SafetyacbgdvNo ratings yet
- QuestionnaireDocument4 pagesQuestionnairevin_jai08100% (1)
- Textbook of Orthodontics: Fig. 9.32HDocument7 pagesTextbook of Orthodontics: Fig. 9.32HNathalia AmeldaNo ratings yet
- Applied Statistics Basic ConceptsDocument28 pagesApplied Statistics Basic ConceptsYousra OsmanNo ratings yet
- Ayantu MekonnenDocument30 pagesAyantu Mekonnenmbgeletu1221No ratings yet
- Medical Report Template-88245314Document3 pagesMedical Report Template-88245314Alvin WongNo ratings yet
- Study Literature Review: Hubungan Tingkat Depresi: Dengan Kualitas Tidur Pada Lanjut UsiaDocument10 pagesStudy Literature Review: Hubungan Tingkat Depresi: Dengan Kualitas Tidur Pada Lanjut UsiaEla NurlaelaNo ratings yet
- Lifting, Moving and Rapid ExDocument13 pagesLifting, Moving and Rapid Expdfs.olpNo ratings yet
- Project Proposal: Total Beneficiaries Include The FollowingDocument8 pagesProject Proposal: Total Beneficiaries Include The FollowingBoris MbiazoNo ratings yet
- Psychosocial Assessment SWK Practice IIIDocument7 pagesPsychosocial Assessment SWK Practice IIIapi-628734736No ratings yet
- NHS FPX 6004 Assessment 2 Policy ProposalDocument5 pagesNHS FPX 6004 Assessment 2 Policy Proposalzadem5266No ratings yet
- TSR Meeting GuidelinesDocument19 pagesTSR Meeting GuidelinesShafis KhanNo ratings yet
- Raid Home Insect Killer EDocument8 pagesRaid Home Insect Killer EFillo IbrahimNo ratings yet
- Research Methodology and Statistics: Diwakar Education HubDocument291 pagesResearch Methodology and Statistics: Diwakar Education HubChanthniNo ratings yet