You might also like
- The Strange ICA Stones of PeruDocument31 pagesThe Strange ICA Stones of PeruRoman Aleshkevich100% (1)
- Structural Notes and Specifications for ConcreteDocument1 pageStructural Notes and Specifications for Concreteroger100% (2)
- Form Ibpr Haul Road PDFDocument2 pagesForm Ibpr Haul Road PDFelvandi100% (1)
- Bonanza A36 ChecklistDocument10 pagesBonanza A36 Checklistalbucur100% (4)
- Muscle Mag August 2014Document148 pagesMuscle Mag August 2014ElthonJeffrey100% (5)
- Ultrasound Imaging of The AbdomenDocument224 pagesUltrasound Imaging of The AbdomenAsztalos Attila100% (9)
- Basic Principles of Growth DevelopmentDocument19 pagesBasic Principles of Growth DevelopmentMikz Chua100% (1)
- Unidrive Classic User Guide PDFDocument195 pagesUnidrive Classic User Guide PDFkukaNo ratings yet
- Benign Retroperitoneal Schwannoma A Case Series and Review of The LiteratureDocument4 pagesBenign Retroperitoneal Schwannoma A Case Series and Review of The LiteratureafmzzqrhardloaNo ratings yet
- Biliary Cystadenocarcinoma With Mesenchymal Stroma: A Case ReportDocument7 pagesBiliary Cystadenocarcinoma With Mesenchymal Stroma: A Case ReportAnalia RodriguezNo ratings yet
- Panc NeopDocument10 pagesPanc NeopShahid HussainNo ratings yet
- Nej M CPC 079007Document10 pagesNej M CPC 079007Pandu Nugroho KantaNo ratings yet
- Mixed Adenoneuroendocrine Carcinoma of The Gallbladder: Case PresentationDocument3 pagesMixed Adenoneuroendocrine Carcinoma of The Gallbladder: Case PresentationGeorgiana WltNo ratings yet
- Rare Pancreatic Tumor Case ReportDocument3 pagesRare Pancreatic Tumor Case ReportcostachemfNo ratings yet
- Pancreatic Head Mass: What Can Be Done ? Diagnosis: UltrasonographyDocument4 pagesPancreatic Head Mass: What Can Be Done ? Diagnosis: UltrasonographyMolla WariNo ratings yet
- 1 s2.0 S1930043321006816 MainDocument5 pages1 s2.0 S1930043321006816 MainFatimah AssagafNo ratings yet
- Jurnal 7Document3 pagesJurnal 7rahayuNo ratings yet
- Weissferdt 2015Document6 pagesWeissferdt 2015gabrielnunesNo ratings yet
- Esophageal Cancer: Diagnosis and Management: Ai Zheng Aizheng Chinese Journal of Cancer October 2010Document13 pagesEsophageal Cancer: Diagnosis and Management: Ai Zheng Aizheng Chinese Journal of Cancer October 2010Al VlaovicNo ratings yet
- Committee 3: Diagnostic Terminology: BackgroundDocument36 pagesCommittee 3: Diagnostic Terminology: BackgroundDaniel KurtyczNo ratings yet
- TangDocument8 pagesTangPatricia BezneaNo ratings yet
- Abdominal-Pelvic Mass Revealing A Krukenberg Tumour: A Case RepportDocument4 pagesAbdominal-Pelvic Mass Revealing A Krukenberg Tumour: A Case RepportIJAR JOURNALNo ratings yet
- 2007-03 - Intestinal Autotransplantation For Adenocarcinoma of Pancreas Involving The Mesenteric Root - Our Experience and Literature Review PDFDocument3 pages2007-03 - Intestinal Autotransplantation For Adenocarcinoma of Pancreas Involving The Mesenteric Root - Our Experience and Literature Review PDFNawzad SulayvaniNo ratings yet
- Pancreatic Head Mass: What Can Be Done ? Diagnosis: UltrasonographyDocument4 pagesPancreatic Head Mass: What Can Be Done ? Diagnosis: Ultrasonographynarsing59No ratings yet
- 54 Raviswami EtalDocument3 pages54 Raviswami EtaleditorijmrhsNo ratings yet
- Synchronous Pancreatic Neuroendocrine Tumor and Pancreatic Cyst A Case ReportDocument4 pagesSynchronous Pancreatic Neuroendocrine Tumor and Pancreatic Cyst A Case ReportWorld Journal of Clinical SurgeryNo ratings yet
- Kista PankreasDocument16 pagesKista PankreasNur Islah AgustiNo ratings yet
- Frantz TumorDocument5 pagesFrantz TumorAndu1991No ratings yet
- Journal of Pediatric Surgery Case Reports: Wandering Mesenteric CystDocument4 pagesJournal of Pediatric Surgery Case Reports: Wandering Mesenteric CysthilalNo ratings yet
- 1 s2.0 S1930043316302217 MainDocument5 pages1 s2.0 S1930043316302217 MainGemiNo ratings yet
- Current Diagnosis and Management of Retroperitoneal SarcomaDocument11 pagesCurrent Diagnosis and Management of Retroperitoneal SarcomaMaximiliano TorresNo ratings yet
- Spontaneous Regression of Pancreatic Cancer: A Case Report and Literature ReviewDocument5 pagesSpontaneous Regression of Pancreatic Cancer: A Case Report and Literature ReviewHitomi-No ratings yet
- Undifferentiated Pleomorphic Sarcoma of The Pancreas With Metachronious Liver Metastasis, A Rare Case ReportDocument8 pagesUndifferentiated Pleomorphic Sarcoma of The Pancreas With Metachronious Liver Metastasis, A Rare Case ReportIJAR JOURNALNo ratings yet
- Annals of Medicine and Surgery: Uwe Scheuermann, Rizky Widyaningsih, Maria Hoppe-Lotichius, Michael Heise, Gerd OttoDocument7 pagesAnnals of Medicine and Surgery: Uwe Scheuermann, Rizky Widyaningsih, Maria Hoppe-Lotichius, Michael Heise, Gerd OttoClinton InfantNo ratings yet
- Unexplained ascites sign of rare cancerDocument3 pagesUnexplained ascites sign of rare cancersandzatNo ratings yet
- Rare Case of Pelvic Schwannoma Mimicking Intra-Ligamenter Uterine Fibroid A Case ReportDocument5 pagesRare Case of Pelvic Schwannoma Mimicking Intra-Ligamenter Uterine Fibroid A Case ReportSatrya WibawaNo ratings yet
- Cervical Cancer With Bilateral Ovarian Metastases: Case Report and Review of LiteratureDocument3 pagesCervical Cancer With Bilateral Ovarian Metastases: Case Report and Review of Literatureevi ermawatiNo ratings yet
- Pancreatoblastoma: A Case Report: Indrawati, Rahmayani, Susi Hariyati, SoeriptoDocument5 pagesPancreatoblastoma: A Case Report: Indrawati, Rahmayani, Susi Hariyati, SoeriptoMelati SatriasNo ratings yet
- JournalDocument5 pagesJournalMuhammad SyariefNo ratings yet
- Pertanyaan Referat CA SigmoidDocument9 pagesPertanyaan Referat CA SigmoidBelladinaMMNo ratings yet
- Cattel-Braash Maneur With SMartery FirstDocument5 pagesCattel-Braash Maneur With SMartery FirstabxazNo ratings yet
- Mucoepidermoidcarcinoma of The Pancreas: A Case ReportDocument3 pagesMucoepidermoidcarcinoma of The Pancreas: A Case ReportIJAR JOURNALNo ratings yet
- Casereports 18 125 PDFDocument6 pagesCasereports 18 125 PDFAstrianti Kusuma WardaniNo ratings yet
- Rare Squamous Cell Carcinoma of the PancreasDocument2 pagesRare Squamous Cell Carcinoma of the Pancreaserick_khristianNo ratings yet
- Urology Case ReportsDocument2 pagesUrology Case ReportsCardio FK UMPNo ratings yet
- Prognosis Node-Positive Cancer: ColonDocument3 pagesPrognosis Node-Positive Cancer: ColonEdward Arthur IskandarNo ratings yet
- Understanding Ampullary CarcinomaDocument18 pagesUnderstanding Ampullary CarcinomaNguyễn Trịnh Xuân HợpNo ratings yet
- Magnetic Resonance Imaging - 2003 - Danet - Liver Metastases From Pancreatic Adenocarcinoma MR Imaging CharacteristicsDocument8 pagesMagnetic Resonance Imaging - 2003 - Danet - Liver Metastases From Pancreatic Adenocarcinoma MR Imaging CharacteristicsPaolo FerranteNo ratings yet
- PancreatoblastomaDocument16 pagesPancreatoblastomaDr Farman AliNo ratings yet
- 2 SinovialsarcomaDocument6 pages2 Sinovialsarcomacindy315No ratings yet
- BAB I PancreatoblastomaDocument5 pagesBAB I PancreatoblastomaHana YunikoNo ratings yet
- A Rare Case of Colon Cancer in A Young Patient: A Case Report and Literature ReviewDocument5 pagesA Rare Case of Colon Cancer in A Young Patient: A Case Report and Literature ReviewIJAR JOURNALNo ratings yet
- Surgical Management of Solid Tumor-4674Document7 pagesSurgical Management of Solid Tumor-4674Theofhila AldelaNo ratings yet
- Metastatic Breast Cancer Presenting As A Gallstone Ileus: Case ReportDocument3 pagesMetastatic Breast Cancer Presenting As A Gallstone Ileus: Case ReportMaghfirah MahmuddinNo ratings yet
- Urachal Carcinoma: Clinicopathologic Features and Long-Term Outcomes of An Aggressive MalignancyDocument9 pagesUrachal Carcinoma: Clinicopathologic Features and Long-Term Outcomes of An Aggressive MalignancyDario D'AmbraNo ratings yet
- Eyelid TattoingDocument15 pagesEyelid Tattoing小島隆司No ratings yet
- Fibrolamellar Variant of Hepatocellular Carcinoma in A Young FemaleDocument3 pagesFibrolamellar Variant of Hepatocellular Carcinoma in A Young FemaleIKIKIKIKIKI999999No ratings yet
- CR1.1 - Masriana - Adenocarcinoma of Gallbladder.Document23 pagesCR1.1 - Masriana - Adenocarcinoma of Gallbladder.sarahadila7762No ratings yet
- PancreasDocument6 pagesPancreasPatricia BezneaNo ratings yet
- YagciDocument7 pagesYagciPatricia BezneaNo ratings yet
- Pancreatic Adenocarcinoma Mimicking PseudocystDocument3 pagesPancreatic Adenocarcinoma Mimicking PseudocystInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- s40792 018 0489 1Document7 pagess40792 018 0489 1Laura PredescuNo ratings yet
- Primary Congenital Choledochal Cyst With Squamous Cell Carcinoma: A Case ReportDocument6 pagesPrimary Congenital Choledochal Cyst With Squamous Cell Carcinoma: A Case ReportRais KhairuddinNo ratings yet
- Retroperitoneal Tumors: Clinical ManagementFrom EverandRetroperitoneal Tumors: Clinical ManagementCheng-Hua LuoNo ratings yet
- Salivary Gland Cancer: From Diagnosis to Tailored TreatmentFrom EverandSalivary Gland Cancer: From Diagnosis to Tailored TreatmentLisa LicitraNo ratings yet
- Iapapa Evidencebased Guidelines For The Management of Acute Panc 2013Document15 pagesIapapa Evidencebased Guidelines For The Management of Acute Panc 2013ali aydemirNo ratings yet
- Karas 2011Document6 pagesKaras 2011ali aydemirNo ratings yet
- American Society Prolapso RectalDocument11 pagesAmerican Society Prolapso RectalvictorNo ratings yet
- Cirugi A Espan Ola: Relationship Between Metabolic Syndrome and Postmenopausal Breast CancerDocument7 pagesCirugi A Espan Ola: Relationship Between Metabolic Syndrome and Postmenopausal Breast Cancerali aydemirNo ratings yet
- International Journal of Surgery ResearchDocument4 pagesInternational Journal of Surgery Researchali aydemirNo ratings yet
- HN E-Catalog CableDocument36 pagesHN E-Catalog CableMin Min AungNo ratings yet
- 3 - 2017 - Superia X 5 StarDocument26 pages3 - 2017 - Superia X 5 Starsomnath serviceNo ratings yet
- Duarte Et Al - Resin CementsDocument28 pagesDuarte Et Al - Resin Cementsjfrascarolo100% (4)
- ARTIKEL 44 Famuntamah 391-399Document9 pagesARTIKEL 44 Famuntamah 391-399Dandi Aksan MasjudNo ratings yet
- Topic - 2015 Quality MethotdDocument12 pagesTopic - 2015 Quality MethotdclaudiaNo ratings yet
- Beginning Algebra 9th Edition Tobey Solutions Manual 1Document39 pagesBeginning Algebra 9th Edition Tobey Solutions Manual 1kyle100% (30)
- Brooks MT 3018Document16 pagesBrooks MT 3018Martin AndradeNo ratings yet
- Agco - DBB - f68.f69Document6 pagesAgco - DBB - f68.f69Mohd Khairi Mohd NorzianNo ratings yet
- BKTK-2010, Failure in Material ConstructionsDocument17 pagesBKTK-2010, Failure in Material ConstructionsSorulay Way-neyNo ratings yet
- Entrepreneurs That Changed The Face of IndiaDocument4 pagesEntrepreneurs That Changed The Face of Indiamarykavitha_6No ratings yet
- Innogy Invitation For Seminar PCODocument6 pagesInnogy Invitation For Seminar PCOTivorshio MacabodbodNo ratings yet
- Product Overview: NCV71208: Octal Solenoid Current Controller With N-FET PredriversDocument1 pageProduct Overview: NCV71208: Octal Solenoid Current Controller With N-FET PredriversDimitar PetrovNo ratings yet
- Project: M/S Cae-Gondia at Nagpur Cable Schedule For Proposed ProjectDocument26 pagesProject: M/S Cae-Gondia at Nagpur Cable Schedule For Proposed ProjectMurali MohanNo ratings yet
- DBXLH 8585B VTMDocument4 pagesDBXLH 8585B VTMmau_mmx5738No ratings yet
- RR No. 6-2015 PDFDocument5 pagesRR No. 6-2015 PDFErlene CompraNo ratings yet
- Plano Grupo ElectrogenoDocument2 pagesPlano Grupo Electrogenoluis alberto rodriguezNo ratings yet
- Listing of Equipment For Network DesignDocument3 pagesListing of Equipment For Network DesignJake D La MadridNo ratings yet
- Bitsat 2023Document1 pageBitsat 2023Kavyansh GoyalNo ratings yet
- NeseritideDocument28 pagesNeseritideNavojit Chowdhury100% (1)
- Nikon Nivo C Series Instruction ManualDocument65 pagesNikon Nivo C Series Instruction ManualBambang Deriyanto100% (1)
- F9Q816Document4 pagesF9Q816Charaf-eddine RamehNo ratings yet
- Caffeine Natural Coffee BeanDocument1 pageCaffeine Natural Coffee BeanMayang TariNo ratings yet
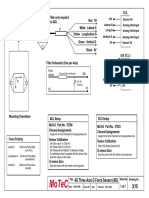
- Filter and wiring schematic for 3-axis ADL G-force sensorDocument1 pageFilter and wiring schematic for 3-axis ADL G-force sensorJuan Ramón Pérez LorenzoNo ratings yet