You might also like
- Wound Assessment ChartDocument4 pagesWound Assessment ChartSinichi Kudo100% (1)
- Emergency NursingDocument56 pagesEmergency NursingNur SanaaniNo ratings yet
- Nursing Care PlanDocument6 pagesNursing Care PlanChesca MejiaNo ratings yet
- Universally Accepted AbbreviationsDocument4 pagesUniversally Accepted AbbreviationsPamela Dela Cerna BrionesNo ratings yet
- NHS Fife Assessment Chart For Wound ManagementDocument3 pagesNHS Fife Assessment Chart For Wound ManagementImran KhanNo ratings yet
- COMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideFrom EverandCOMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideNo ratings yet
- MS 3 Case Analysis DownloadableDocument1 pageMS 3 Case Analysis DownloadableCharissa Magistrado De LeonNo ratings yet
- NLE Poisons and AntidotesDocument2 pagesNLE Poisons and AntidotesGodfrey Franco100% (1)
- NURSING CARE OF ADULTS II: Passbooks Study GuideFrom EverandNURSING CARE OF ADULTS II: Passbooks Study GuideNo ratings yet
- Vital Signs PDFDocument2 pagesVital Signs PDFsaguliteNo ratings yet
- Musculoskeletal BulletsDocument9 pagesMusculoskeletal Bulletswinner gift flowersNo ratings yet
- Nur 111 Session 18 Sas 1Document11 pagesNur 111 Session 18 Sas 1Zzimply Tri Sha UmaliNo ratings yet
- Abg Specimen Collection Test RequisitionDocument7 pagesAbg Specimen Collection Test RequisitionVangie OriginesNo ratings yet
- Activity 1 Assessment of Patients With Cardiovascular Disorders PDFDocument1 pageActivity 1 Assessment of Patients With Cardiovascular Disorders PDFJarda DacuagNo ratings yet
- Management of Tuberculosis: A guide for clinicians (eBook edition)From EverandManagement of Tuberculosis: A guide for clinicians (eBook edition)No ratings yet
- Pediatric AppendicitisDocument15 pagesPediatric AppendicitisPatricia MoránNo ratings yet
- Emergency DrugsDocument26 pagesEmergency DrugsSiergs Smith GervacioNo ratings yet
- Nursing Responsibilities in Handling AntibioticsDocument4 pagesNursing Responsibilities in Handling Antibioticsrichardmd20% (1)
- Pharm Exam ReviewDocument13 pagesPharm Exam ReviewAshleyNo ratings yet
- Name of Student: - InstructionDocument31 pagesName of Student: - InstructionPaul Jackson50% (2)
- Fall Risk Assessment FormDocument3 pagesFall Risk Assessment FormMichael Silva100% (1)
- CVPDocument13 pagesCVPmeisin kuraesinNo ratings yet
- Necrotizing Otitis 2022Document20 pagesNecrotizing Otitis 2022asmashNo ratings yet
- Med Surg (Oncology)Document169 pagesMed Surg (Oncology)DardarConstantinoNo ratings yet
- Impaired Skin IntegrityDocument8 pagesImpaired Skin IntegrityMacmac ReyesNo ratings yet
- Board Questions 2009Document16 pagesBoard Questions 2009Erick EspinoNo ratings yet
- NP1 NotesDocument59 pagesNP1 NotesBrianMarBeltranNo ratings yet
- Nursing Care Plan Sample For BeginnersDocument15 pagesNursing Care Plan Sample For BeginnersMoe KhanNo ratings yet
- Cardiovascular FunctionDocument157 pagesCardiovascular FunctionJonnabelle PadillaNo ratings yet
- Tracheostomy Care - An Evidence-Based Guide - American Nurse TodayDocument4 pagesTracheostomy Care - An Evidence-Based Guide - American Nurse TodayZulaikah Nur IstiqomahNo ratings yet
- Critical Thinking Nursing Care LippincotsDocument35 pagesCritical Thinking Nursing Care Lippincotseric100% (1)
- Narratives Case NotesDocument4 pagesNarratives Case NotesKnigh RiderNo ratings yet
- Top Up Training Center and Research Consultancy Communicable Disease NursingDocument3 pagesTop Up Training Center and Research Consultancy Communicable Disease NursingSTEFFI GABRIELLE GOLEZNo ratings yet
- A Simple Guide to Abdominal Aortic Aneurysm, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Abdominal Aortic Aneurysm, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Nursing Care Plan - MergedDocument13 pagesNursing Care Plan - MergedJuls Flares SycaycoNo ratings yet
- Renal Fabs NotesDocument9 pagesRenal Fabs NotesLucky GomezNo ratings yet
- Chapter 69 Nursing Management EmergencyDocument6 pagesChapter 69 Nursing Management EmergencyMeganNo ratings yet
- Classification of Burns Based On Depth CharacteristicsDocument2 pagesClassification of Burns Based On Depth CharacteristicsmexelleNo ratings yet
- Veteran Memorial Medical Center Citizens - Charter - 2015 - EditionDocument25 pagesVeteran Memorial Medical Center Citizens - Charter - 2015 - EditionJun MadrigalNo ratings yet
- Nursing Dummy ChartDocument4 pagesNursing Dummy Chartis_aradanasNo ratings yet
- Fluids and Electrolytes ConceptDocument31 pagesFluids and Electrolytes ConceptDarwin AndalNo ratings yet
- Omaha System Journal ReadingDocument4 pagesOmaha System Journal ReadingAya PaquitNo ratings yet
- Perioperative CareDocument48 pagesPerioperative CareBryan FederizoNo ratings yet
- FundaDocument81 pagesFundatzuquinoNo ratings yet
- West Visayas State University: Nursing ProcessDocument4 pagesWest Visayas State University: Nursing ProcessPhylum Chordata100% (1)
- Harris Regional ICU Daily Sedation Vacation GuidelinesDocument1 pageHarris Regional ICU Daily Sedation Vacation GuidelinesFebri Yudha Adhi KurniawanNo ratings yet
- Critical Care Nurses' Knowledge RegardingManagement of Patients WithAtrial Fibrillation at Baghdad CityDocument5 pagesCritical Care Nurses' Knowledge RegardingManagement of Patients WithAtrial Fibrillation at Baghdad CityIOSRjournalNo ratings yet
- DOH Herbal PlantsDocument16 pagesDOH Herbal Plantskyra_naomiNo ratings yet
- ColostomyDocument13 pagesColostomyKetali JambhavdekarNo ratings yet
- DARDocument4 pagesDARfritzroseNo ratings yet
- AbbreviationDocument19 pagesAbbreviationJayson NatividadNo ratings yet
- Pointers To Review Updated 2016Document18 pagesPointers To Review Updated 2016Rubelyn Arriola Nioko100% (1)
- NCM 122 Ratio FinalsDocument2 pagesNCM 122 Ratio FinalsLorenz Jude CańeteNo ratings yet
- 9 Tips On How To Make A Good SOAPIEDocument7 pages9 Tips On How To Make A Good SOAPIEMagbanua Airene MarielNo ratings yet
- START / Jump START Triage: ImmediateDocument2 pagesSTART / Jump START Triage: ImmediateJerome DanielNo ratings yet
- Concept Map FinalDocument1 pageConcept Map Finalapi-383763177No ratings yet
- Care of Clients Requiring SurgeryDocument4 pagesCare of Clients Requiring SurgeryMichelle Tamor100% (1)
- C C C M MMMM MM M MMM 3mm MMMMM MM M MMMMMDocument4 pagesC C C M MMMM MM M MMM 3mm MMMMM MM M MMMMMjohkieNo ratings yet
- The Wound-Burn GuidelinesDocument22 pagesThe Wound-Burn GuidelinesAdelaVargasRojasNo ratings yet
- Identification InfectionDocument6 pagesIdentification Infectioneva arna abrarNo ratings yet
- Modern Wound Care (Article Journal)Document14 pagesModern Wound Care (Article Journal)eva arna abrarNo ratings yet
- IWGDF Guidance On The Diagnosis and Management of Foot Infections in Persons With DiabeteDocument30 pagesIWGDF Guidance On The Diagnosis and Management of Foot Infections in Persons With DiabeteSarwan Hadi-llNo ratings yet
- Clinical Relevance MicrobiologyDocument14 pagesClinical Relevance Microbiologyeva arna abrarNo ratings yet
- Biomarker For InfectionDocument21 pagesBiomarker For Infectioneva arna abrarNo ratings yet
- Bioburden in Chronic WoundDocument24 pagesBioburden in Chronic Woundeva arna abrarNo ratings yet
- Research Methods For Nurses and MidwivesDocument5 pagesResearch Methods For Nurses and Midwiveseva arna abrarNo ratings yet
- Community Wound BacteriDocument11 pagesCommunity Wound Bacterieva arna abrarNo ratings yet
- Chronic Wound BiofilmDocument9 pagesChronic Wound Biofilmeva arna abrarNo ratings yet
- Women & Diabetes Our Right To A Healthy FutureDocument4 pagesWomen & Diabetes Our Right To A Healthy Futureeva arna abrarNo ratings yet
- Federman Et Al-2016-Wound Repair and RegenerationDocument9 pagesFederman Et Al-2016-Wound Repair and Regenerationeva arna abrarNo ratings yet
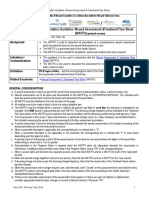
- Documentation Guideline: Wound Assessment &treatment Flow Sheet (Watfs)Document4 pagesDocumentation Guideline: Wound Assessment &treatment Flow Sheet (Watfs)eva arna abrarNo ratings yet
- HSE National Wound Management Guidelines 2018 PDFDocument367 pagesHSE National Wound Management Guidelines 2018 PDFMaria Asri PranataNo ratings yet
- Management of Wounds in The Community: Five Principles: Clinical FocusDocument4 pagesManagement of Wounds in The Community: Five Principles: Clinical Focuseva arna abrarNo ratings yet
- Wound Assessment: A Step-By-Step ProcessDocument3 pagesWound Assessment: A Step-By-Step Processeva arna abrarNo ratings yet
- Ound Ssessment and Anagement: Document Summary/Key PointsDocument21 pagesOund Ssessment and Anagement: Document Summary/Key Pointseva arna abrarNo ratings yet
- ABC of Wound Healing PDFDocument4 pagesABC of Wound Healing PDFMrJPhaetonNo ratings yet
- Documentation Guideline: Wound Assessment &treatment Flow Sheet (Watfs)Document4 pagesDocumentation Guideline: Wound Assessment &treatment Flow Sheet (Watfs)eva arna abrarNo ratings yet
- 6b1de98d155522d8aa02e9c2f23b9cf1Document6 pages6b1de98d155522d8aa02e9c2f23b9cf1Katrina SuarezNo ratings yet
- ABC of Wound Healing PDFDocument4 pagesABC of Wound Healing PDFMrJPhaetonNo ratings yet
- JR 1Document10 pagesJR 1Nurul FajriahNo ratings yet
- Dolby Atmos Specifications PDFDocument24 pagesDolby Atmos Specifications PDFVanya ValdovinosNo ratings yet
- 4 FAR EAST BANK & TRUST COMPANY V DIAZ REALTY INCDocument3 pages4 FAR EAST BANK & TRUST COMPANY V DIAZ REALTY INCDanielleNo ratings yet
- HRM OmantelDocument8 pagesHRM OmantelSonia Braham100% (1)
- A Comprehensive Review On Renewable and Sustainable Heating Systems For Poultry FarmingDocument22 pagesA Comprehensive Review On Renewable and Sustainable Heating Systems For Poultry FarmingPl TorrNo ratings yet
- LaMOT Rupture DiscsDocument20 pagesLaMOT Rupture Discshlrich99No ratings yet
- (Ambition) Malaysia 2023 Market Insights ReportDocument46 pages(Ambition) Malaysia 2023 Market Insights ReportMaz Izman BudimanNo ratings yet
- Carpio V ValmonteDocument2 pagesCarpio V ValmonteErvin John Reyes100% (2)
- Renvoi in Private International LawDocument4 pagesRenvoi in Private International LawAgav VithanNo ratings yet
- Non-Hazardous Areas Adjustable Pressure Switch: 6900P - Piston SensorDocument2 pagesNon-Hazardous Areas Adjustable Pressure Switch: 6900P - Piston SensorDiana ArredondoNo ratings yet
- Meco ReviewerDocument9 pagesMeco ReviewerKang ChulNo ratings yet
- DMP 2021 TPJ SRDocument275 pagesDMP 2021 TPJ SRishu sNo ratings yet
- TM9-238 Deepwater Fording of Ordnance Materiel PDFDocument35 pagesTM9-238 Deepwater Fording of Ordnance Materiel PDFdieudecafeNo ratings yet
- FC2060Document10 pagesFC2060esnNo ratings yet
- 15.910 Draft SyllabusDocument10 pages15.910 Draft SyllabusSaharNo ratings yet
- Where To Eat PizzaDocument3 pagesWhere To Eat PizzaLiliancitaLcJsNo ratings yet
- Factors Affecting The Rate of Chemical Reactions Notes Key 1Document3 pagesFactors Affecting The Rate of Chemical Reactions Notes Key 1api-292000448No ratings yet
- Imp121 1isDocument6 pagesImp121 1isErnesto AyzenbergNo ratings yet
- B&G 3DX LiteratureDocument2 pagesB&G 3DX LiteratureAnonymous 7xHNgoKE6eNo ratings yet
- Setup LogDocument221 pagesSetup LogCarlos MendezNo ratings yet
- Hospital Management System DatabaseDocument18 pagesHospital Management System DatabasesamdhathriNo ratings yet
- Craske - Mastering Your Fears and FobiasDocument174 pagesCraske - Mastering Your Fears and Fobiasjuliana218No ratings yet
- The Perceived Barriers and Entrepreneurial Intention of Young Technical ProfessionalsDocument6 pagesThe Perceived Barriers and Entrepreneurial Intention of Young Technical ProfessionalsAnatta OngNo ratings yet
- Item No. 6 Diary No 6856 2024 ConsolidatedDocument223 pagesItem No. 6 Diary No 6856 2024 Consolidatedisha NagpalNo ratings yet
- Eastern Bank Limited: Name: ID: American International University of Bangladesh Course Name: Faculty Name: Due DateDocument6 pagesEastern Bank Limited: Name: ID: American International University of Bangladesh Course Name: Faculty Name: Due DateTasheen MahabubNo ratings yet
- Phet Body Group 1 ScienceDocument42 pagesPhet Body Group 1 ScienceMebel Alicante GenodepanonNo ratings yet
- Cam 12 Test 2 ReadingDocument7 pagesCam 12 Test 2 ReadingLê Nguyễn Ái DuyênNo ratings yet
- On The Backward Problem For Parabolic Equations With MemoryDocument19 pagesOn The Backward Problem For Parabolic Equations With MemorykamranNo ratings yet
- WS-250 4BB 60 Cells 40mm DatasheetDocument2 pagesWS-250 4BB 60 Cells 40mm DatasheetTejash NaikNo ratings yet
- BSDC CCOE DRAWING FOR 2x6 KL R-1Document1 pageBSDC CCOE DRAWING FOR 2x6 KL R-1best viedosNo ratings yet
- Power Dense and Robust Traction Power Inverter For The Second Generation Chevrolet Volt Extended Range EDocument8 pagesPower Dense and Robust Traction Power Inverter For The Second Generation Chevrolet Volt Extended Range Ejrz000No ratings yet