You might also like
- Modern Wound Care Practical Aspects of Non Interventional Topical Treatment of Patients With Chronic WoundsDocument14 pagesModern Wound Care Practical Aspects of Non Interventional Topical Treatment of Patients With Chronic WoundsDauz ArashNo ratings yet
- TIMEDocument19 pagesTIMEela.mcab8No ratings yet
- Clinical Dermatology Open Access Journal: A Review of Wound Dressing PracticesDocument12 pagesClinical Dermatology Open Access Journal: A Review of Wound Dressing PracticesnurhariNo ratings yet
- Amnion in The Treatment of Pediatric Partial Thickness Facial BurnsDocument7 pagesAmnion in The Treatment of Pediatric Partial Thickness Facial BurnsInggrid Ayusari AsaliNo ratings yet
- Use of Cold Plasma in the Treatment of Infected WoundDocument10 pagesUse of Cold Plasma in the Treatment of Infected WoundAthenaeum Scientific PublishersNo ratings yet
- Gerpac 2014 ReviewDocument3 pagesGerpac 2014 ReviewTim SandleNo ratings yet
- Treatment of Burns in The First 24 Hours: Simple and Practical Guide by Answering 10 Questions in A Step-By-Step FormDocument11 pagesTreatment of Burns in The First 24 Hours: Simple and Practical Guide by Answering 10 Questions in A Step-By-Step FormtiaraNo ratings yet
- Clinical Use of Polihexanide On Acute and Chronic Wounds For Antisepsis and DecontaminationDocument7 pagesClinical Use of Polihexanide On Acute and Chronic Wounds For Antisepsis and DecontaminationHllerdNo ratings yet
- J Deutsche Derma Gesell - 2019 - Augustin - Diagnosis and Treatment of Xerosis Cutis A Position PaperDocument32 pagesJ Deutsche Derma Gesell - 2019 - Augustin - Diagnosis and Treatment of Xerosis Cutis A Position PaperAlisher YermekNo ratings yet
- Evidence-Based Care of Acute Wounds: A PerspectiveDocument9 pagesEvidence-Based Care of Acute Wounds: A PerspectiveWilliams MenaNo ratings yet
- Qué Poner y Qué No Poner en Una HeridaDocument4 pagesQué Poner y Qué No Poner en Una HeridaFlor Hernández RosasNo ratings yet
- Effect of Ozone Therapy Dressing Technique On The Healing Process of Recent 2nd Degree BurnsDocument24 pagesEffect of Ozone Therapy Dressing Technique On The Healing Process of Recent 2nd Degree BurnsIOSRjournalNo ratings yet
- View Doc 635470672036959908Document6 pagesView Doc 635470672036959908abhishekbmcNo ratings yet
- Impact of Nursing Rehabilitation Program On Minimizing Post - Burn Joint ContractureDocument15 pagesImpact of Nursing Rehabilitation Program On Minimizing Post - Burn Joint ContractureIJAR JOURNALNo ratings yet
- A Review of Wound Dressing PracticesDocument13 pagesA Review of Wound Dressing PracticesAnonymous 1nMTZWmzNo ratings yet
- Hydrogel DressingDocument13 pagesHydrogel Dressingrevina aNo ratings yet
- Maggot Debridement Therapy For Diabetic Foot Ulcer: Experience From Maggot Treatment Centers Http://ajpp - InDocument4 pagesMaggot Debridement Therapy For Diabetic Foot Ulcer: Experience From Maggot Treatment Centers Http://ajpp - InOsmela PutriNo ratings yet
- Remove Barriers To Healing: Focus On Wound Bed Preparation: Meeting ReportDocument4 pagesRemove Barriers To Healing: Focus On Wound Bed Preparation: Meeting ReportAFRIANSYAHNo ratings yet
- 2010 - Octenidine Dihydrochloride, A Modern Antiseptic For Skin, Mucous Membranes and WoundsDocument15 pages2010 - Octenidine Dihydrochloride, A Modern Antiseptic For Skin, Mucous Membranes and Woundsnovia100% (2)
- Surgical Site InfectionsDocument22 pagesSurgical Site InfectionsSheryl DurrNo ratings yet
- Updated Guidelines for Managing Hypertrophic Scars and KeloidsDocument9 pagesUpdated Guidelines for Managing Hypertrophic Scars and KeloidssonuguptapeeyushNo ratings yet
- Banana Leaf DressingDocument6 pagesBanana Leaf DressingOmomomo781No ratings yet
- Undisturbedhealing JWCRipponetalDocument9 pagesUndisturbedhealing JWCRipponetalRachel RiordanNo ratings yet
- How To... Ten Top Questions and Answers On The Use of Dressings For Pressure Ulcer PreventionDocument32 pagesHow To... Ten Top Questions and Answers On The Use of Dressings For Pressure Ulcer Preventionelviana kabanNo ratings yet
- How To... Ten Top Questions and Answers On The Use of Dressings For Pressure Ulcer PreventionDocument32 pagesHow To... Ten Top Questions and Answers On The Use of Dressings For Pressure Ulcer Preventionelviana kabanNo ratings yet
- BiocellulosaDocument4 pagesBiocellulosadesi mitraNo ratings yet
- Most Essential Learning CompetencyDocument6 pagesMost Essential Learning CompetencyPaolo OcampoNo ratings yet
- Updated Scar Management Practical Guidelines Non-IDocument10 pagesUpdated Scar Management Practical Guidelines Non-IChilo PrimaNo ratings yet
- Content Woundcare Effective Skin and Wound Management of Non-Complex Burns BestPracticeGuidelinesDocument28 pagesContent Woundcare Effective Skin and Wound Management of Non-Complex Burns BestPracticeGuidelinesBayu Pratama PutraNo ratings yet
- Wound Dressing PDFDocument6 pagesWound Dressing PDFaprilia siregarNo ratings yet
- Clinical Applied Anatomy in Wound CareDocument18 pagesClinical Applied Anatomy in Wound CareKlinik Komuniti Perwira100% (2)
- Wound Dressings Update: Carolina Weller, Geoff SussmanDocument7 pagesWound Dressings Update: Carolina Weller, Geoff SussmanKevin AdrianNo ratings yet
- Hospital Burn CareDocument9 pagesHospital Burn CareAgung Rizka PratamaNo ratings yet
- 1471 2334 14 315Document8 pages1471 2334 14 315Aqib Nabil HakimNo ratings yet
- Emergency Treatment On Facial Laceration of Dog Bite Wounds With Immediate Primary Closure: A Prospective Randomized Trial StudyDocument5 pagesEmergency Treatment On Facial Laceration of Dog Bite Wounds With Immediate Primary Closure: A Prospective Randomized Trial StudyJC QuezadaNo ratings yet
- s15 - Hypochlorous - Acid - Add HOCLDocument40 pagess15 - Hypochlorous - Acid - Add HOCLMichael de la BarraNo ratings yet
- S1 guideline tinea capitisDocument19 pagesS1 guideline tinea capitisCasey GondoNo ratings yet
- Quemaduras: Primeras 24 HorasDocument10 pagesQuemaduras: Primeras 24 HorasLuis BetancourtNo ratings yet
- Ijccm 18 479 - 1Document1 pageIjccm 18 479 - 1Renata RicciardiNo ratings yet
- Negative Pressure Wound TherapyDocument9 pagesNegative Pressure Wound TherapySuharyonoNo ratings yet
- PP FMH NPQ Y6 J 9 H RK 7 CPXNTLFDocument6 pagesPP FMH NPQ Y6 J 9 H RK 7 CPXNTLFburhanNo ratings yet
- Promote Severe Wound Healing by Pvpi Dry Powder Spray Case Series ReportDocument4 pagesPromote Severe Wound Healing by Pvpi Dry Powder Spray Case Series ReportShira michaelNo ratings yet
- Applied Wound ManagementDocument21 pagesApplied Wound ManagementBrian Harris100% (3)
- EBSCOhost 3 PDFDocument27 pagesEBSCOhost 3 PDFWawan Febri RamdaniNo ratings yet
- Wound Cleansing: Benefits of Hypochlorous AcidDocument5 pagesWound Cleansing: Benefits of Hypochlorous Acidlps DiamondNo ratings yet
- An Asian Perspective On Povidone Iodine in Wound Healing: Review PaperDocument11 pagesAn Asian Perspective On Povidone Iodine in Wound Healing: Review PaperAsmita KurniaNo ratings yet
- Hydrocolloid Dressing PDFDocument17 pagesHydrocolloid Dressing PDFeyleenNo ratings yet
- Infection Control in AnaesthesiaDocument19 pagesInfection Control in AnaesthesiaSherifMohamedNo ratings yet
- A New Approach To Local Burn Wound Care: Moist Exposed Therapy. A Multiphase, Multicenter StudyDocument9 pagesA New Approach To Local Burn Wound Care: Moist Exposed Therapy. A Multiphase, Multicenter StudyNur Sidiq Agung SNo ratings yet
- Wound Healing With Vitamin CDocument4 pagesWound Healing With Vitamin CAntonio TovarNo ratings yet
- Gueltzow 2018Document12 pagesGueltzow 2018burhanNo ratings yet
- 2007 Sa Sawma Wound Cleansing and Dressing Procedure Nov 07Document23 pages2007 Sa Sawma Wound Cleansing and Dressing Procedure Nov 07Kristine Artes AguilarNo ratings yet
- Regular Use of A Hand Cream Can Attenuate Skin Dryness and Roughness Caused by Frequent Hand WashingDocument6 pagesRegular Use of A Hand Cream Can Attenuate Skin Dryness and Roughness Caused by Frequent Hand Washingmewtiny31No ratings yet
- EBP EONSMalignantFungatingWoundsDocument30 pagesEBP EONSMalignantFungatingWoundsNaoval Meilandi Nurjaman100% (1)
- Fbioe 07 00342Document16 pagesFbioe 07 00342Reynee Shaira MatulacNo ratings yet
- The Wound Dressings and Their Applications in Wound Healing and ManagementDocument2 pagesThe Wound Dressings and Their Applications in Wound Healing and ManagementJohn FredNo ratings yet
- IWGDF Guidance On The Diagnosis and Management of Foot Infections in Persons With DiabeteDocument30 pagesIWGDF Guidance On The Diagnosis and Management of Foot Infections in Persons With DiabeteSarwan Hadi-llNo ratings yet
- Clinical Relevance MicrobiologyDocument14 pagesClinical Relevance Microbiologyeva arna abrarNo ratings yet
- Community Wound BacteriDocument11 pagesCommunity Wound Bacterieva arna abrarNo ratings yet
- Biomarker For InfectionDocument21 pagesBiomarker For Infectioneva arna abrarNo ratings yet
- Identification InfectionDocument6 pagesIdentification Infectioneva arna abrarNo ratings yet
- The Wound-Burn GuidelinesDocument22 pagesThe Wound-Burn GuidelinesAdelaVargasRojasNo ratings yet
- Chronic Wound BiofilmDocument9 pagesChronic Wound Biofilmeva arna abrarNo ratings yet
- Bioburden in Chronic WoundDocument24 pagesBioburden in Chronic Woundeva arna abrarNo ratings yet
- Federman Et Al-2016-Wound Repair and RegenerationDocument9 pagesFederman Et Al-2016-Wound Repair and Regenerationeva arna abrarNo ratings yet
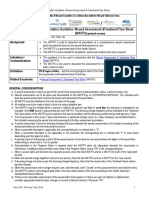
- Documentation Guideline: Wound Assessment &treatment Flow Sheet (Watfs)Document4 pagesDocumentation Guideline: Wound Assessment &treatment Flow Sheet (Watfs)eva arna abrarNo ratings yet
- Research Methods For Nurses and MidwivesDocument5 pagesResearch Methods For Nurses and Midwiveseva arna abrarNo ratings yet
- Documentation Guideline: Wound Assessment &treatment Flow Sheet (Watfs)Document4 pagesDocumentation Guideline: Wound Assessment &treatment Flow Sheet (Watfs)eva arna abrarNo ratings yet
- Women & Diabetes Our Right To A Healthy FutureDocument4 pagesWomen & Diabetes Our Right To A Healthy Futureeva arna abrarNo ratings yet
- HSE National Wound Management Guidelines 2018 PDFDocument367 pagesHSE National Wound Management Guidelines 2018 PDFMaria Asri PranataNo ratings yet
- Management of Wounds in The Community: Five Principles: Clinical FocusDocument4 pagesManagement of Wounds in The Community: Five Principles: Clinical Focuseva arna abrarNo ratings yet
- Documentation Guideline: Wound Assessment &treatment Flow Sheet (WATFS) Portrait Version With PSLS#Document6 pagesDocumentation Guideline: Wound Assessment &treatment Flow Sheet (WATFS) Portrait Version With PSLS#eva arna abrarNo ratings yet
- ABC of Wound Healing PDFDocument4 pagesABC of Wound Healing PDFMrJPhaetonNo ratings yet
- Wound Assessment: A Step-By-Step ProcessDocument3 pagesWound Assessment: A Step-By-Step Processeva arna abrarNo ratings yet
- JR 1Document10 pagesJR 1Nurul FajriahNo ratings yet
- 6b1de98d155522d8aa02e9c2f23b9cf1Document6 pages6b1de98d155522d8aa02e9c2f23b9cf1Katrina SuarezNo ratings yet
- Ound Ssessment and Anagement: Document Summary/Key PointsDocument21 pagesOund Ssessment and Anagement: Document Summary/Key Pointseva arna abrarNo ratings yet
- ABC of Wound Healing PDFDocument4 pagesABC of Wound Healing PDFMrJPhaetonNo ratings yet
- Unit 1 Part 2Document100 pagesUnit 1 Part 220331a1212No ratings yet
- Unfamiliar Words Activity 1Document1 pageUnfamiliar Words Activity 1Sharmaine Ann AustriaNo ratings yet
- Ftre 2014 Sample Paper Class 8 Paper 1 PDFDocument13 pagesFtre 2014 Sample Paper Class 8 Paper 1 PDFPushpa PalNo ratings yet
- MICRO Lecture 1 Introduction To Microbiology and Parasitology 1 PDFDocument29 pagesMICRO Lecture 1 Introduction To Microbiology and Parasitology 1 PDFJireh AcabalNo ratings yet
- Merda SeccaDocument25 pagesMerda Seccamothafukka100% (5)
- CBSE Class 9 Biology The Fundamental Unit of LifeDocument3 pagesCBSE Class 9 Biology The Fundamental Unit of Lifeaaditya100% (1)
- Obat Herbal Untuk AritmiaDocument17 pagesObat Herbal Untuk AritmiaFerina Nadya PratamaNo ratings yet
- (English) Vision - Crash Course A&P #18 (DownSub - Com)Document8 pages(English) Vision - Crash Course A&P #18 (DownSub - Com)bank townNo ratings yet
- BCH 203 & 202Document28 pagesBCH 203 & 202metasynthronos748No ratings yet
- IAH AC Introduction To HomotoxicologyDocument60 pagesIAH AC Introduction To HomotoxicologywurtukukNo ratings yet
- Biology Exam 2022 Form4Document12 pagesBiology Exam 2022 Form4Yahya Abdiwahab100% (1)
- Analyze Paragraphs on Professors' Duties, Open-Heart Surgery, Anti-Smoking Efforts, Laser SurgeryDocument2 pagesAnalyze Paragraphs on Professors' Duties, Open-Heart Surgery, Anti-Smoking Efforts, Laser Surgeryratu wilhelminaNo ratings yet
- JuteDocument54 pagesJuteAkash BhowmikNo ratings yet
- Aakash Rank Booster Test Series For NEET-2020Document17 pagesAakash Rank Booster Test Series For NEET-2020Indian VanguardsNo ratings yet
- Stage-7-English-Paper-1 Alr FinishDocument12 pagesStage-7-English-Paper-1 Alr FinishMr. GreenNo ratings yet
- Quiz 4 (Pass - Quizchapter4) (Page 1 of 2)Document1 pageQuiz 4 (Pass - Quizchapter4) (Page 1 of 2)co caNo ratings yet
- Review General & USMLE Microbiology MCQsDocument51 pagesReview General & USMLE Microbiology MCQsM7md AllahhamNo ratings yet
- The Effectiveness of Evening Primrose Oil Gel Capsule As A Cervical Ripening Agent During Labor InductionDocument4 pagesThe Effectiveness of Evening Primrose Oil Gel Capsule As A Cervical Ripening Agent During Labor InductionHazel Anne Ison Dumayas100% (1)
- DNS A InstructionsDocument2 pagesDNS A InstructionsWilda PanjaitanNo ratings yet
- CAPSTONE For Grade 12Document16 pagesCAPSTONE For Grade 12Rona RuizNo ratings yet
- X Science QPDocument7 pagesX Science QPhritikaray4475No ratings yet
- Answer Paper 2 PAP 1 2015Document7 pagesAnswer Paper 2 PAP 1 2015Nick LeeNo ratings yet
- 20 Bio TDocument20 pages20 Bio Tchehan tony 22No ratings yet
- DK - Strengthen.your - Back P2PDocument130 pagesDK - Strengthen.your - Back P2Palina_gheorghe_8No ratings yet
- Mini-CLIA SystemDocument6 pagesMini-CLIA SystemVictoria AnnaNo ratings yet
- RGO TOP Reviewer MarcosDocument29 pagesRGO TOP Reviewer MarcosREALYN ZAMBASNo ratings yet
- El Engaño Del EvolucionismoDocument136 pagesEl Engaño Del EvolucionismoRichard OliverosNo ratings yet
- Why Aren't Signals of Female Quality More Common? D. J. Hosken, S. H. Alonzo, N. Wedell 2016Document3 pagesWhy Aren't Signals of Female Quality More Common? D. J. Hosken, S. H. Alonzo, N. Wedell 2016methyl_vanillinNo ratings yet
- Postpartum HemorrhageDocument11 pagesPostpartum HemorrhageColeen Aubrey TanNo ratings yet
- The Perceptual Implications of GaiaDocument12 pagesThe Perceptual Implications of Gaiaapi-279625022No ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (403)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (20)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (5)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- 12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosFrom Everand12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosRating: 4.5 out of 5 stars4.5/5 (207)
- Daniel Kahneman's "Thinking Fast and Slow": A Macat AnalysisFrom EverandDaniel Kahneman's "Thinking Fast and Slow": A Macat AnalysisRating: 3.5 out of 5 stars3.5/5 (130)
- Algorithms to Live By: The Computer Science of Human DecisionsFrom EverandAlgorithms to Live By: The Computer Science of Human DecisionsRating: 4.5 out of 5 stars4.5/5 (722)
- Gut: the new and revised Sunday Times bestsellerFrom EverandGut: the new and revised Sunday Times bestsellerRating: 4 out of 5 stars4/5 (392)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Summary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedRating: 4 out of 5 stars4/5 (11)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningFrom EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningRating: 4 out of 5 stars4/5 (3)