You might also like
- Test Bank For Medical Terminology and Anatomy For Coding 3rd Edition by ShilandDocument8 pagesTest Bank For Medical Terminology and Anatomy For Coding 3rd Edition by Shilanda5967275420% (2)
- Im 2Document3 pagesIm 2neni budiNo ratings yet
- Simplified Pediatric ECGDocument11 pagesSimplified Pediatric ECGSuman MondalNo ratings yet
- 779 FullDocument6 pages779 FullAlexander G. Álvarez RojasNo ratings yet
- JurnalDocument6 pagesJurnalBhenNo ratings yet
- Proximal RCA Occlusion Producing Anterior ST Segment Elevation, Q Waves, and T Wave InversionDocument5 pagesProximal RCA Occlusion Producing Anterior ST Segment Elevation, Q Waves, and T Wave InversionsunhaolanNo ratings yet
- Wswecocekgdasar2018Document34 pagesWswecocekgdasar2018Hendra AbeitNo ratings yet
- Supraventricular TachycardiDocument8 pagesSupraventricular TachycardiHairunisa 0049No ratings yet
- ECG A Methodical Approach - Leaflet Print - Patient UKDocument7 pagesECG A Methodical Approach - Leaflet Print - Patient UKBen MpanzuNo ratings yet
- Ecg PDFDocument70 pagesEcg PDFlauras3005No ratings yet
- Ecg 7 Der y AvrDocument9 pagesEcg 7 Der y AvrElmer MoscosoNo ratings yet
- Normal Impulse Conduction: Sinoatrial Node AV Node Bundle of His Bundle Branches Purkinje FibersDocument73 pagesNormal Impulse Conduction: Sinoatrial Node AV Node Bundle of His Bundle Branches Purkinje FibersIndra ToshiwayNo ratings yet
- 7.article - Nurse Method For Quick Interpret ECGDocument13 pages7.article - Nurse Method For Quick Interpret ECGEvieta CallysthaNo ratings yet
- Onderwijs ECG Quiz 2019Document15 pagesOnderwijs ECG Quiz 2019Kelsey van SonNo ratings yet
- Establishing The Mechanism of Supraventricular Tachycardia in The Electrophysiology LaboratoryDocument15 pagesEstablishing The Mechanism of Supraventricular Tachycardia in The Electrophysiology LaboratorySamuelNo ratings yet
- TSV Con Aberrancia o TVDocument7 pagesTSV Con Aberrancia o TVOliverVasconcelosNo ratings yet
- Taquicardias Ventriculares Qhion Cheng y Andrea Natale 2020Document16 pagesTaquicardias Ventriculares Qhion Cheng y Andrea Natale 2020Vallejo Romo Alberto CristianNo ratings yet
- Fetal and Neonatal Arrythmias 2015Document13 pagesFetal and Neonatal Arrythmias 2015Diana Catalina Lopez MoraNo ratings yet
- Normal Impulse Conduction: Sinoatrial Node AV Node Bundle of His Bundle Branches Purkinje FibersDocument73 pagesNormal Impulse Conduction: Sinoatrial Node AV Node Bundle of His Bundle Branches Purkinje FibersIndra ToshiwayNo ratings yet
- AHA/ACCF/HRS Recommendations For The Standardization and Interpretation of The ElectrocardiogramDocument6 pagesAHA/ACCF/HRS Recommendations For The Standardization and Interpretation of The ElectrocardiogramArya BimaNo ratings yet
- Kjped 60 344Document9 pagesKjped 60 344hinduja reddipilliNo ratings yet
- Criterii EKG Mayo ClinicDocument45 pagesCriterii EKG Mayo ClinicAnca LunguNo ratings yet
- Echocardiography ExaminationDocument10 pagesEchocardiography ExaminationYanira NoemíNo ratings yet
- Introduction To Interpretation V10.0 (2017-2018)Document91 pagesIntroduction To Interpretation V10.0 (2017-2018)Muhammad AsrudinNo ratings yet
- Kuliah Penyegaran Basic Ecg DR IbanDocument44 pagesKuliah Penyegaran Basic Ecg DR IbanGoez Aditya NugrahaNo ratings yet
- Tachdjian 5Document8 pagesTachdjian 5Abrudan GabrielNo ratings yet
- Arritmias Ventriculares en Corazones NormalesDocument14 pagesArritmias Ventriculares en Corazones Normalessanalejo0290No ratings yet
- A El Outline June 2007Document82 pagesA El Outline June 2007neysaonlineNo ratings yet
- Basics of EKG InterpretationDocument132 pagesBasics of EKG InterpretationArif Imam HidayatNo ratings yet
- An Important Cause of Wide Complex Tachycardia: Case PresentationDocument2 pagesAn Important Cause of Wide Complex Tachycardia: Case PresentationLuis Fernando Morales JuradoNo ratings yet
- (PDF.3) Management of Heart AttackDocument33 pages(PDF.3) Management of Heart AttackTheany Be SmilerNo ratings yet
- IV A Ecg Preparation 12 Lead Placements NCM 118 Nursing Care of Clients With Life Threatening CondDocument13 pagesIV A Ecg Preparation 12 Lead Placements NCM 118 Nursing Care of Clients With Life Threatening CondRio DanteNo ratings yet
- Clinical ElectrocardiographyDocument134 pagesClinical ElectrocardiographyHossain MuhammadNo ratings yet
- Morgan 2012Document5 pagesMorgan 2012aixacamila3No ratings yet
- EKG Basics - LongDocument40 pagesEKG Basics - Longمحمد خالدNo ratings yet
- Interpretasi ECG Dr. SallyDocument66 pagesInterpretasi ECG Dr. SallyRichard GunawanNo ratings yet
- Ecg PDFDocument87 pagesEcg PDFSabir KhanNo ratings yet
- Luis Fernando Pava MolanoDocument5 pagesLuis Fernando Pava MolanoVallejo Romo Alberto CristianNo ratings yet
- EKG ATLAS InterpretationDocument316 pagesEKG ATLAS InterpretationDumitrescu Roxana100% (1)
- ECG in Emergency Medicine (2006)Document234 pagesECG in Emergency Medicine (2006)EcoGert100% (1)
- 1 s2.0 S0002914915018445 MainDocument8 pages1 s2.0 S0002914915018445 MainFaomix de la HouseNo ratings yet
- Cath SAP 5Document47 pagesCath SAP 5Angel AliNo ratings yet
- 15 Walters LLSA ArticlesDocument33 pages15 Walters LLSA ArticlesericNo ratings yet
- Importance of Ecgs in Management of CV DiseasesDocument50 pagesImportance of Ecgs in Management of CV DiseasesPragnesh ShahNo ratings yet
- 12 - Lead ECG-A Web Brain For Easy InterpretationDocument54 pages12 - Lead ECG-A Web Brain For Easy Interpretatione-kino3692100% (1)
- Ecg Utah EduDocument87 pagesEcg Utah EduMos Viorel DanutNo ratings yet
- Jamainternal Zhang 2021 Ce 210028 1635441147.09994Document2 pagesJamainternal Zhang 2021 Ce 210028 1635441147.09994gwyneth.green.512No ratings yet
- 5 ECG Interpretation With AnswersDocument48 pages5 ECG Interpretation With AnswersQusai Ibraheem100% (1)
- Interesting ECG Sharing: Ms. Yiu Sau-Chi, GigiDocument49 pagesInteresting ECG Sharing: Ms. Yiu Sau-Chi, GigiCarmen FongNo ratings yet
- OYAMADocument94 pagesOYAMAAndrea zabala veraNo ratings yet
- Adverse Diastolic Remodeling After Reperfused ST-elevation Myocardial Infarction: An Important Prognostic IndicatorDocument11 pagesAdverse Diastolic Remodeling After Reperfused ST-elevation Myocardial Infarction: An Important Prognostic IndicatorCatia MoraesNo ratings yet
- Diagnostic Pacing Maneuvers Part 1Document16 pagesDiagnostic Pacing Maneuvers Part 1chirudarsiNo ratings yet
- ABC of Pediatric ECGDocument5 pagesABC of Pediatric ECGThalita SophiaNo ratings yet
- Rido, Rudini - Paediatric ECGDocument51 pagesRido, Rudini - Paediatric ECGFikriYTNo ratings yet
- Basics of EKG InterpretationDocument53 pagesBasics of EKG InterpretationHala BahaaNo ratings yet
- 1 s2.0 S0929664608602041 MainDocument9 pages1 s2.0 S0929664608602041 MainEko SiswantoNo ratings yet
- ARVCDocument6 pagesARVCCatur UtamiNo ratings yet
- Atlas of 3D Transesophageal Echocardiography in Structural Heart Disease Interventions: Cases and VideosFrom EverandAtlas of 3D Transesophageal Echocardiography in Structural Heart Disease Interventions: Cases and VideosNo ratings yet
- Electrocardiography of Inherited Arrhythmias and Cardiomyopathies: From Basic Science to Clinical PracticeFrom EverandElectrocardiography of Inherited Arrhythmias and Cardiomyopathies: From Basic Science to Clinical PracticeNo ratings yet
- Localisation of PVCDocument7 pagesLocalisation of PVCDenny IntanNo ratings yet
- Pocket Book For PhysiotherapistDocument339 pagesPocket Book For PhysiotherapistEloisaNo ratings yet
- Cor Pulmonale - Introduction To Cor Pulmonale, Etiology and Pathophysiology of Cor Pulmonale, Epidemiology of Cor PulmonaleDocument18 pagesCor Pulmonale - Introduction To Cor Pulmonale, Etiology and Pathophysiology of Cor Pulmonale, Epidemiology of Cor PulmonaleRicky SpideyNo ratings yet
- Tip-Tv: Program Supplement CT: Cardiac ApplicationsDocument47 pagesTip-Tv: Program Supplement CT: Cardiac ApplicationsvitapabloNo ratings yet
- Lecture - 3 Properties of Cardiac MuscleDocument35 pagesLecture - 3 Properties of Cardiac MuscleMRM7MDNo ratings yet
- Se1201 PDFDocument138 pagesSe1201 PDFIrina BuracNo ratings yet
- ECG EKG Examples and QuizDocument26 pagesECG EKG Examples and QuizBUBBUNo ratings yet
- Interpretarea Ritmului CardiacDocument40 pagesInterpretarea Ritmului CardiacBatraneluNo ratings yet
- CVS Physio Case Files p1Document4 pagesCVS Physio Case Files p1dawnparkNo ratings yet
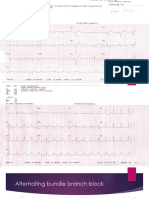
- Alternating Bundle Branch BlockDocument9 pagesAlternating Bundle Branch BlockSyifa Mahmud Syukran AkbarNo ratings yet
- BPL-DF 2617aedrDocument3 pagesBPL-DF 2617aedrBiomedical Incharge SRM TrichyNo ratings yet
- Equipo de Contrapulsacion Arrow-KaatDocument103 pagesEquipo de Contrapulsacion Arrow-KaatCarito HernandezNo ratings yet
- Healthcare Monitoring System and Transforming Monitored Data Into Real Time Clinical Feedback Based On Iot Using Raspberry PiDocument7 pagesHealthcare Monitoring System and Transforming Monitored Data Into Real Time Clinical Feedback Based On Iot Using Raspberry Pimikko intalNo ratings yet
- Universidad Pedagógica Y Tecnológica de Colombia Engineering FacultyDocument6 pagesUniversidad Pedagógica Y Tecnológica de Colombia Engineering Facultyluigilops 1No ratings yet
- ECG-based Human Authentication: A Review: Abstract-The Electrocardiogram (ECG) Is An EmergingDocument6 pagesECG-based Human Authentication: A Review: Abstract-The Electrocardiogram (ECG) Is An EmergingmuraliNo ratings yet
- Module - 6.advance 12 Lead InterpretationDocument30 pagesModule - 6.advance 12 Lead InterpretationFerry SofyanriNo ratings yet
- R-Peak Detection Algorithm For Ecg Using Double Difference and RR Interval ProcessingDocument5 pagesR-Peak Detection Algorithm For Ecg Using Double Difference and RR Interval ProcessingArash MinNo ratings yet
- Contrapulsatore Aortico Autocat 2 Wave Education MaterialsDocument52 pagesContrapulsatore Aortico Autocat 2 Wave Education MaterialsJose Moreno100% (1)
- Bonaventura 0Document1 pageBonaventura 0hvillafuertebNo ratings yet
- Basic ECG InterpretationDocument7 pagesBasic ECG InterpretationAprilJaedeeSanAgustinNo ratings yet
- The Confi Dent Touch: Philips Pagewriter Tc20 CardiographDocument4 pagesThe Confi Dent Touch: Philips Pagewriter Tc20 CardiographGeneral Health CareNo ratings yet
- SOP ElectrocardiographsDocument7 pagesSOP ElectrocardiographsDodik E. PrasetyoNo ratings yet
- Project Arduino1Document31 pagesProject Arduino1Hussein KadhmNo ratings yet
- Unit 7 Cardiac (S)Document78 pagesUnit 7 Cardiac (S)Cheyenne SchimpfNo ratings yet
- Low Power Portable Solar Based ECG SystemDocument3 pagesLow Power Portable Solar Based ECG SystemInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- 26 124MWDocument47 pages26 124MWfaymeghaniNo ratings yet
- Recognizing Normal ECGDocument50 pagesRecognizing Normal ECGJosiephine Bucalon100% (3)
- Operating Manual Ergometrics ER 900 (English)Document84 pagesOperating Manual Ergometrics ER 900 (English)miryangelNo ratings yet