You might also like
- Diabetes Study GuideDocument4 pagesDiabetes Study GuideNicole Brassington0% (1)
- Biology Revision Notes Part3Document10 pagesBiology Revision Notes Part3volvanskyNo ratings yet
- Insulin: Deciding How Much Insulin To TakeDocument12 pagesInsulin: Deciding How Much Insulin To Takeராபர்ட் ஆன்றோ ரெனி100% (1)
- Pharmacology Review NotesDocument24 pagesPharmacology Review NotescampbellqueenNo ratings yet
- A Practical Guide To Insulin TherapyDocument42 pagesA Practical Guide To Insulin Therapyseun williams100% (2)
- Modern Power Transformer Practice - R. Feinberg PDFDocument360 pagesModern Power Transformer Practice - R. Feinberg PDFAlberto Ortiz100% (1)
- SYNERGY Fake Job Offer LetterDocument5 pagesSYNERGY Fake Job Offer LetterSyed's Way PoolNo ratings yet
- 2011 - Practical Guide Insulin TherapyDocument6 pages2011 - Practical Guide Insulin Therapytheva_thy100% (1)
- Stephen Spender Selected PoemsDocument28 pagesStephen Spender Selected PoemsWriting Hub100% (1)
- NEBOSH Assignment Report Unit D 2015Document80 pagesNEBOSH Assignment Report Unit D 2015Saeed Malik100% (4)
- Insulin HandbookDocument67 pagesInsulin HandbookThits SarNo ratings yet
- Physiology of Limbic System by DR ShahabDocument23 pagesPhysiology of Limbic System by DR ShahabShahabuddin Shaikh100% (2)
- Types of Insulin: NOTE: Exact Onset, Action, and Duration Are Dependent On The Generic/brand UsedDocument3 pagesTypes of Insulin: NOTE: Exact Onset, Action, and Duration Are Dependent On The Generic/brand Usedask1400No ratings yet
- ESWT - For Myositis Ossificans CaseDocument13 pagesESWT - For Myositis Ossificans CaseSienriesta NovianaNo ratings yet
- Terapi Insulin-1Document46 pagesTerapi Insulin-1Yanti MoonNo ratings yet
- GUIDELINES FOR INPATIENT DIABETES MANAGEMENT هااامDocument1 pageGUIDELINES FOR INPATIENT DIABETES MANAGEMENT هااامAbu HuzaifaNo ratings yet
- Insulin AdministrationDocument15 pagesInsulin Administrationmec17No ratings yet
- Diabetes Insulin InitiationDocument12 pagesDiabetes Insulin InitiationSatinder BhallaNo ratings yet
- Adjusting Your Insulin DoseDocument3 pagesAdjusting Your Insulin DoseLib AsNo ratings yet
- Metabolism and AtpDocument20 pagesMetabolism and AtpAbdul Rafay ShaikhNo ratings yet
- Long Term DiabetesDocument68 pagesLong Term Diabetesnawaraj2044No ratings yet
- Insulin TherapyDocument60 pagesInsulin Therapylight tweenNo ratings yet
- DInsulin Types 1Document22 pagesDInsulin Types 1zahrabokerNo ratings yet
- InsulinDocument4 pagesInsulinHa Zizzle100% (1)
- Type 1 Diabetes Mellitus: TreatmentDocument25 pagesType 1 Diabetes Mellitus: TreatmentironNo ratings yet
- Pharm WK 11 - DiabetesDocument12 pagesPharm WK 11 - DiabetesHope RobersonNo ratings yet
- Treatment of Diabetes MellitusDocument25 pagesTreatment of Diabetes MellitusPurnima ChoudhuryNo ratings yet
- Calculate The Dose of Diabetes MellitusDocument5 pagesCalculate The Dose of Diabetes MellitusOmar Nassir MoftahNo ratings yet
- Insulin in DiabetesDocument9 pagesInsulin in DiabetesAbdul SamadNo ratings yet
- Insulin NewDocument41 pagesInsulin NewSheikNo ratings yet
- Switching Between Insulin Products in Humanitarian Response 2022 Easter Europe 3 18 2022 DDRC English v3Document3 pagesSwitching Between Insulin Products in Humanitarian Response 2022 Easter Europe 3 18 2022 DDRC English v3vijay740No ratings yet
- General Principles of Insulin Therapy in Diabetes MellitusDocument24 pagesGeneral Principles of Insulin Therapy in Diabetes MellitusEDWIN WIJAYANo ratings yet
- Hayatt Univesity College. Faculty of Medicine. Family Medicine. Mohamed Gassim Mohamed. Insulin ManagementDocument14 pagesHayatt Univesity College. Faculty of Medicine. Family Medicine. Mohamed Gassim Mohamed. Insulin ManagementMohammed GassimNo ratings yet
- DM TreatmentDocument9 pagesDM TreatmentAshraf AbdullahNo ratings yet
- General Principles of Insulin Therapy in Diabetes MellitusDocument12 pagesGeneral Principles of Insulin Therapy in Diabetes MellitusRuban RichardNo ratings yet
- Insulin Therapy: by Dr. Adithya PolavarapuDocument18 pagesInsulin Therapy: by Dr. Adithya Polavarapuadithya polavarapuNo ratings yet
- DM Lab 2 - FinalDocument33 pagesDM Lab 2 - FinalMahamed Wefkey OmranNo ratings yet
- Insulin Treatment in DiabetesDocument86 pagesInsulin Treatment in DiabetesAhsan Rauf100% (1)
- General Principles of Insulin Therapy in Diabetes Mellitus - UpToDateDocument20 pagesGeneral Principles of Insulin Therapy in Diabetes Mellitus - UpToDateabdulghaniNo ratings yet
- Diabetic DrugsDocument39 pagesDiabetic DrugsNONDUMISONo ratings yet
- Diabetes Treatment: Dr. Chavan P.R. Pharm DDocument73 pagesDiabetes Treatment: Dr. Chavan P.R. Pharm DAvel ChandNo ratings yet
- Module 9 ElaborateDocument6 pagesModule 9 ElaborateTrishaNo ratings yet
- Oral RevalidaDocument39 pagesOral Revalidajunathancortez123No ratings yet
- Insulin Initiation PPT - PPTX 2Document53 pagesInsulin Initiation PPT - PPTX 2Meno Ali100% (1)
- Types of Insulin PDFDocument3 pagesTypes of Insulin PDFRetno WulanNo ratings yet
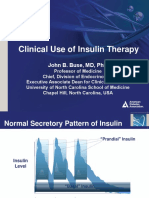
- Slide Clinical Use of Insulin Therapy (ADA)Document36 pagesSlide Clinical Use of Insulin Therapy (ADA)Dian SobaNo ratings yet
- New Microsoft Word DocumentDocument2 pagesNew Microsoft Word Documenteslambasuony98No ratings yet
- Using Insulin: What Is Insulin? Types of InsulinDocument4 pagesUsing Insulin: What Is Insulin? Types of InsulinRyo RyozNo ratings yet
- Managing Diabetes - RaflaDocument38 pagesManaging Diabetes - Raflamsala76No ratings yet
- What Types of Insulin Are Available in Canada?: Types Name (Brand Name) Onset Peak Action DurationDocument2 pagesWhat Types of Insulin Are Available in Canada?: Types Name (Brand Name) Onset Peak Action Durationdebabrata5976No ratings yet
- Insulin TypesDocument4 pagesInsulin TypesMichael Angelo SeñaNo ratings yet
- Insulin Initiation and MonitoringDocument35 pagesInsulin Initiation and Monitoringeka prasepti darusmanNo ratings yet
- ADA 2021 Instensifying Injectable Therapy.v.3Document2 pagesADA 2021 Instensifying Injectable Therapy.v.3Ariel GutierrezNo ratings yet
- InsulinDocument5 pagesInsulinAshan BopitiyaNo ratings yet
- Effective Use of Insulin: PreviewDocument6 pagesEffective Use of Insulin: Previewprad1973No ratings yet
- Interactive Patient Case Management #1Document33 pagesInteractive Patient Case Management #1Luzman HizrianNo ratings yet
- Anti-Diabetic Drugs InsulinDocument26 pagesAnti-Diabetic Drugs Insulinwissam salimNo ratings yet
- Pharmacology - Endocrine SystemDocument9 pagesPharmacology - Endocrine System22bgu0805msNo ratings yet
- Capitol University: Name: Sophia B. Duquinlay Date: 09-16-21 Section/ CN: 137 NCP #: 1Document2 pagesCapitol University: Name: Sophia B. Duquinlay Date: 09-16-21 Section/ CN: 137 NCP #: 1Sophia DuquinlayNo ratings yet
- 03 Diabetes2 DrugsDocument38 pages03 Diabetes2 DrugsPutu Indah SaraswatiNo ratings yet
- Approsch To DM1Document4 pagesApprosch To DM1M MazloumNo ratings yet
- What Are The Things You Need To Know When Receiving A Patient From ER?Document4 pagesWhat Are The Things You Need To Know When Receiving A Patient From ER?Earl Joseph DezaNo ratings yet
- Fit-Diploma 3-2-2024Document57 pagesFit-Diploma 3-2-2024light tweenNo ratings yet
- Insulin Clinician5 PharmacyDocument4 pagesInsulin Clinician5 PharmacydafaloveNo ratings yet
- Pharmacology of Metabolic Drugs: Nurlaili SusantiDocument58 pagesPharmacology of Metabolic Drugs: Nurlaili Susantimillennia zulfaNo ratings yet
- Pharmacology of Metabolic Drugs: Nurlaili SusantiDocument58 pagesPharmacology of Metabolic Drugs: Nurlaili Susantimillennia zulfaNo ratings yet
- How To Switch Insulin Products - Pharm LetterDocument6 pagesHow To Switch Insulin Products - Pharm LetterAraceli LeonNo ratings yet
- Dr. Roberto Conrado Guevara - Response From The Laity (Oct 2)Document29 pagesDr. Roberto Conrado Guevara - Response From The Laity (Oct 2)Joviner Yabres LactamNo ratings yet
- Arterial CatheterizationDocument5 pagesArterial CatheterizationSREEDEVI T SURESHNo ratings yet
- Optional 17 - DisplayDocument2 pagesOptional 17 - DisplayHà Ngọc ĐặngNo ratings yet
- Perceptions of Students RegardDocument6 pagesPerceptions of Students RegardLina Mahayaty SembiringNo ratings yet
- Indumax CLS54D EN - 0218Document12 pagesIndumax CLS54D EN - 0218Carlos LeonNo ratings yet
- Income Tax: Global Income TaxDocument4 pagesIncome Tax: Global Income TaxMichelle Muhrie TablizoNo ratings yet
- COMEDK UGET-2011 Medical Rank ListDocument147 pagesCOMEDK UGET-2011 Medical Rank ListiamvarkeyNo ratings yet
- Identify The Letter of The Choice That Best Completes The Statement or Answers The QuestionDocument18 pagesIdentify The Letter of The Choice That Best Completes The Statement or Answers The QuestionCeline YoonNo ratings yet
- Riding+out+the+storm+-+LatAm+2012 HSBC Dec2012Document98 pagesRiding+out+the+storm+-+LatAm+2012 HSBC Dec2012Sergio Gana GonzalezNo ratings yet
- MSDS Hemolok GelDocument5 pagesMSDS Hemolok GelReniNo ratings yet
- Reading Passage 2: HomeopathyDocument4 pagesReading Passage 2: HomeopathyNguyễn TịnhNo ratings yet
- Bonpak Catalogue 2011Document18 pagesBonpak Catalogue 2011George TowerNo ratings yet
- Pregnancy in Dental TreatmentDocument62 pagesPregnancy in Dental TreatmentChinar HawramyNo ratings yet
- Hosp DimDocument3 pagesHosp DimJoe ThesecondmonthNo ratings yet
- E25 - Lyn Joy v. Mendoza - Technical Assistance ContextualizationDocument3 pagesE25 - Lyn Joy v. Mendoza - Technical Assistance Contextualizationlyn joyNo ratings yet
- Chemistry Notes On The Periodic Table: Syllabus 5070 O' LevelDocument8 pagesChemistry Notes On The Periodic Table: Syllabus 5070 O' LevelNancy Mohamed100% (1)
- Daftar Pustaka PDFDocument7 pagesDaftar Pustaka PDFaulia rahmiNo ratings yet
- Three Things in Life Once Gone Never Come BackDocument27 pagesThree Things in Life Once Gone Never Come BackhemendreNo ratings yet
- Lovely LungsDocument6 pagesLovely Lungsapi-285970439No ratings yet
- Civic LeaguesDocument1 pageCivic LeaguesAnthony TriplinNo ratings yet
- Deltaweld 453 MilDocument40 pagesDeltaweld 453 MilHugo RodriguezNo ratings yet
- Waxman Et Al., 2004: AnalysisDocument2 pagesWaxman Et Al., 2004: AnalysisAmanodin E. TambakNo ratings yet