You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Counselors CompanionDocument866 pagesCounselors Companionkafi na100% (2)
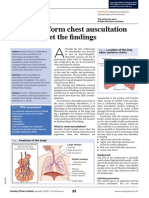
- Assessment On Respiratory ProblemsDocument7 pagesAssessment On Respiratory ProblemsSetiaty PandiaNo ratings yet
- 019 - Ulil Chiqmatuss'diah - KMB 1Document4 pages019 - Ulil Chiqmatuss'diah - KMB 1Setiaty PandiaNo ratings yet
- 019 - Ulil Chiqmatussa'diah - EPN 2 - Assessment On Respiratory Problems..Document7 pages019 - Ulil Chiqmatussa'diah - EPN 2 - Assessment On Respiratory Problems..Setiaty PandiaNo ratings yet
- Patient-Centered Collaborative Care: The Impact of A New Approach To Postpartum Rounds On Residents' Perception of Their Work EnvironmentDocument5 pagesPatient-Centered Collaborative Care: The Impact of A New Approach To Postpartum Rounds On Residents' Perception of Their Work EnvironmentSetiaty PandiaNo ratings yet
- Patient-Centered Collaborative Care: The Impact of A New Approach To Postpartum Rounds On Residents' Perception of Their Work EnvironmentDocument5 pagesPatient-Centered Collaborative Care: The Impact of A New Approach To Postpartum Rounds On Residents' Perception of Their Work EnvironmentSetiaty PandiaNo ratings yet
- Qi Muslimah Talk 1 Ivana FixDocument16 pagesQi Muslimah Talk 1 Ivana FixSetiaty PandiaNo ratings yet
- Jurnal KMB Diva - 015Document10 pagesJurnal KMB Diva - 015Setiaty PandiaNo ratings yet
- Impact of Osteoarthritis On Activities of Daily LiDocument9 pagesImpact of Osteoarthritis On Activities of Daily LiSetiaty PandiaNo ratings yet
- 4927 20042 1 PBDocument7 pages4927 20042 1 PBSetiaty PandiaNo ratings yet
- Hubungan Tingkat Kecemasan Dengan Tingkat Kemandirian Activities of Daily Living Pada LansiaDocument8 pagesHubungan Tingkat Kecemasan Dengan Tingkat Kemandirian Activities of Daily Living Pada LansiaSetiaty PandiaNo ratings yet
- Alat Ukur Untuk Menilai Kemampuan Fungsional Pasien Dengan Osteoartritis Lutut: Tinjauan PustakaDocument6 pagesAlat Ukur Untuk Menilai Kemampuan Fungsional Pasien Dengan Osteoartritis Lutut: Tinjauan PustakaSetiaty PandiaNo ratings yet
- 1385 FullDocument10 pages1385 FullSetiaty PandiaNo ratings yet
- Simple East Asian Landscape Campaign - by SlidesgoDocument54 pagesSimple East Asian Landscape Campaign - by SlidesgoSetiaty PandiaNo ratings yet
- JCM 10 00522 v2Document12 pagesJCM 10 00522 v2Setiaty PandiaNo ratings yet
- Faktor-Faktor Yang Berhubungan Dengan Terjadinya PreeklampsiaDocument13 pagesFaktor-Faktor Yang Berhubungan Dengan Terjadinya PreeklampsiaSetiaty PandiaNo ratings yet
- 116-Article Text-415-1-10-20190507Document8 pages116-Article Text-415-1-10-20190507Setiaty PandiaNo ratings yet
- Progress in Disaster Science: Jeremy Spoon, Drew Gerkey, Ram B. Chhetri, Alisa Rai, Umesh Basnet, Chelsea E. HunterDocument15 pagesProgress in Disaster Science: Jeremy Spoon, Drew Gerkey, Ram B. Chhetri, Alisa Rai, Umesh Basnet, Chelsea E. HunterSetiaty PandiaNo ratings yet
- Health and Quality of Life OutcomesDocument8 pagesHealth and Quality of Life OutcomesSetiaty PandiaNo ratings yet
- Alasan Dilakukannya 4 Kali Amandemen Uud 1945 Tujuan Dan Sejarah PerkembanganDocument11 pagesAlasan Dilakukannya 4 Kali Amandemen Uud 1945 Tujuan Dan Sejarah PerkembanganSetiaty PandiaNo ratings yet
- Material - Using Equipment For Patients' Examination - 019 - Ulil ChiqmatussadiahDocument2 pagesMaterial - Using Equipment For Patients' Examination - 019 - Ulil ChiqmatussadiahSetiaty PandiaNo ratings yet
- Reifika Arfaka Rizieq PSIKA 020Document1 pageReifika Arfaka Rizieq PSIKA 020Setiaty PandiaNo ratings yet
- Consulatation Liaison Psychiatry English Lecture 2012 10Document58 pagesConsulatation Liaison Psychiatry English Lecture 2012 10Setiaty PandiaNo ratings yet
- Reike DIyah Setiawati - 042 - PSIK ADocument28 pagesReike DIyah Setiawati - 042 - PSIK ASetiaty PandiaNo ratings yet
- Deteksi Mycobacterium Tuberculosis Pada Sampel Sputum Menggunakan Teknik Loop-Mediated Isothermal Amplification (LAMP-TB)Document7 pagesDeteksi Mycobacterium Tuberculosis Pada Sampel Sputum Menggunakan Teknik Loop-Mediated Isothermal Amplification (LAMP-TB)Setiaty PandiaNo ratings yet
- Vital Signs and Monitoring - Podcast - IntermediateDocument4 pagesVital Signs and Monitoring - Podcast - IntermediateSetiaty PandiaNo ratings yet
- Control of Nonconforming Work019 Af.r4Document6 pagesControl of Nonconforming Work019 Af.r4Massimiliano PorcelliNo ratings yet
- SITXWHS001 Student Assessment v2.1Document16 pagesSITXWHS001 Student Assessment v2.1Sukhpreet KaurNo ratings yet
- 12 HUMSS Chapter 1Document6 pages12 HUMSS Chapter 1Mayjoy SardallaNo ratings yet
- Psycho Social Theoretical FrameworkDocument14 pagesPsycho Social Theoretical FrameworkSieg AguillonNo ratings yet
- Domestic Violence Literature Review ExampleDocument5 pagesDomestic Violence Literature Review Examplefvdra0st100% (1)
- 02 - IRAOvulation Induction For TheDocument11 pages02 - IRAOvulation Induction For TheHartanto LieNo ratings yet
- Bazooka Monthly Current Affairs August 2023 CompressedDocument134 pagesBazooka Monthly Current Affairs August 2023 CompressedarjunNo ratings yet
- ASiT Conference Abstract Book, Cardiff 2012Document180 pagesASiT Conference Abstract Book, Cardiff 2012Ed Fitzgerald100% (1)
- Shweta Jain (42Y/F) Aarogyam C: Report For Tests AskedDocument14 pagesShweta Jain (42Y/F) Aarogyam C: Report For Tests Askednit2000_jainNo ratings yet
- Race Cadot RilDocument2 pagesRace Cadot RilFebson Lee MathewNo ratings yet
- Tepid-Sponge-Bath PRSDocument4 pagesTepid-Sponge-Bath PRSmaryNo ratings yet
- Nurshing English 1 S1 Keperawatan Tingkat 2 (40 Prosedur Keperawatan)Document361 pagesNurshing English 1 S1 Keperawatan Tingkat 2 (40 Prosedur Keperawatan)Jankrik BelalangNo ratings yet
- Basal Level of Anti-Müllerian Hormone Is Associated With Oocyte Quality in Stimulated CyclesDocument5 pagesBasal Level of Anti-Müllerian Hormone Is Associated With Oocyte Quality in Stimulated CyclesCherysaNo ratings yet
- Assignment: Diversity DilemmasDocument4 pagesAssignment: Diversity DilemmasJoan MendozaNo ratings yet
- ASTMH Exam Brochure 18 FNLDocument17 pagesASTMH Exam Brochure 18 FNLNgô Khánh HuyềnNo ratings yet
- HOPE 4 Module 8 Training PlanDocument10 pagesHOPE 4 Module 8 Training PlanAJ Bacarisas RochaNo ratings yet
- Presented By: Bhawna Joshi Msc. Nursing 1 YearDocument52 pagesPresented By: Bhawna Joshi Msc. Nursing 1 YearBhawna JoshiNo ratings yet
- Thapar, Cooper, Eyre y LangleyDocument15 pagesThapar, Cooper, Eyre y LangleyNicol Mariana V. FernándezNo ratings yet
- Q3 SHS HOPE 2 - Module 3Document12 pagesQ3 SHS HOPE 2 - Module 3Rica Labong100% (1)
- Political SelfDocument53 pagesPolitical SelfMelizza Fajardo BañanoNo ratings yet
- Msds Silicon (Fluid Funituter Polish)Document5 pagesMsds Silicon (Fluid Funituter Polish)ReniNo ratings yet
- BENNETT VS JAKUBOWSKI Et Al.Document43 pagesBENNETT VS JAKUBOWSKI Et Al.Andrew LiebichNo ratings yet
- Covid 19 TrialsDocument289 pagesCovid 19 TrialsPaulo GonzalezNo ratings yet
- Safety Tips: Restaurant and KitchenDocument2 pagesSafety Tips: Restaurant and KitchenYolanda Ivette Peña MoralesNo ratings yet
- Brocure About ExerciseDocument2 pagesBrocure About Exerciseapi-253215535No ratings yet
- Bfhi Implementation 2018 AppendixDocument7 pagesBfhi Implementation 2018 AppendixssNo ratings yet
- Superwarfarin:: A Wifes Means To An Evil EndDocument14 pagesSuperwarfarin:: A Wifes Means To An Evil EndgarciamattNo ratings yet
- Community Service Sites Fall 2023Document5 pagesCommunity Service Sites Fall 2023Nixon MarkNo ratings yet
- Article in Press: The Experience of Intensive Care Nurses Caring For Patients With Delirium: A Phenomenological StudyDocument7 pagesArticle in Press: The Experience of Intensive Care Nurses Caring For Patients With Delirium: A Phenomenological StudySimson TameonNo ratings yet