You might also like
- Anatomy of Voice: How to Enhance and Project Your Best VoiceFrom EverandAnatomy of Voice: How to Enhance and Project Your Best VoiceRating: 4 out of 5 stars4/5 (3)
- Assessment On Respiratory ProblemsDocument7 pagesAssessment On Respiratory ProblemsSetiaty PandiaNo ratings yet
- High Resolution and High Definition Anorectal ManometryFrom EverandHigh Resolution and High Definition Anorectal ManometryMassimo BelliniNo ratings yet
- Defining CharacteristicsDocument2 pagesDefining CharacteristicsAngel MayNo ratings yet
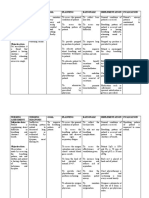
- NURSING CARE PLAN - JayDocument8 pagesNURSING CARE PLAN - JayJaylord VerazonNo ratings yet
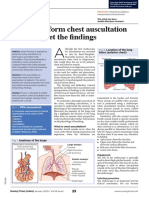
- Fundamentals of Lung Auscultation: New England Journal of Medicine February 2014Document9 pagesFundamentals of Lung Auscultation: New England Journal of Medicine February 2014ANTJE ORNELLA REYESNo ratings yet
- Fundamentals of Lung Auscultation: Review ArticleDocument8 pagesFundamentals of Lung Auscultation: Review ArticleGabriela LosadaNo ratings yet
- Nursing Care Plan: Cues Objectives Interventions Rationale EvaluationDocument2 pagesNursing Care Plan: Cues Objectives Interventions Rationale EvaluationBianca Mikaela DosdosNo ratings yet
- 06 Paediatric and Child Health June2009 PulmonologyDocument51 pages06 Paediatric and Child Health June2009 PulmonologyVivek Edamuriyil RamesanNo ratings yet
- Thoracic and Lung Assessment: College of Nursing and Allied Health Sciences Maasin City, Southern LeyteDocument4 pagesThoracic and Lung Assessment: College of Nursing and Allied Health Sciences Maasin City, Southern LeytePrincess Diana Jean ModesteNo ratings yet
- Pulmonary Auscultation PDFDocument5 pagesPulmonary Auscultation PDFThatikala AbhilashNo ratings yet
- Advanced Life Support: Siska Christianingsih, S.Kep.,Ns.M.KepDocument31 pagesAdvanced Life Support: Siska Christianingsih, S.Kep.,Ns.M.KepFlorenciaNo ratings yet
- Anatomy RespirationDocument29 pagesAnatomy RespirationPatricia Rosabelle RoñoNo ratings yet
- Assessment Nursing Diagnossis Scientific Basis Goal Nursing Intervention Rationale Evaluation IndependentDocument10 pagesAssessment Nursing Diagnossis Scientific Basis Goal Nursing Intervention Rationale Evaluation IndependentPamela laquindanumNo ratings yet
- Endotracheal Tubes: Early Detection of Oesophageal IntubationDocument5 pagesEndotracheal Tubes: Early Detection of Oesophageal IntubationIkea BalhonNo ratings yet
- RADIOLOGY 1.4 Abdominal and Pelvic SonographyDocument5 pagesRADIOLOGY 1.4 Abdominal and Pelvic SonographyZazaNo ratings yet
- Airway Management For Nurses PDFDocument6 pagesAirway Management For Nurses PDFarizza ramosNo ratings yet
- HA Finals ReviewerDocument15 pagesHA Finals ReviewerMichelle Rose RodaviaNo ratings yet
- Lungs and ThoracicDocument66 pagesLungs and ThoracicJoyce Jacobe0% (1)
- Nursing Assessment Nursing Diagnosis Goal Planning Rationale Implementation Evaluation Subjective DataDocument5 pagesNursing Assessment Nursing Diagnosis Goal Planning Rationale Implementation Evaluation Subjective DataDimpal Choudhary100% (1)
- A.) Signs and Symptoms/Assessment: B.) Diagnostic ProceduresDocument13 pagesA.) Signs and Symptoms/Assessment: B.) Diagnostic ProceduresJake Yvan DizonNo ratings yet
- 1 s2.0 S0964339799800743 Main PDFDocument10 pages1 s2.0 S0964339799800743 Main PDFROSANNA BUCAGNo ratings yet
- Mechanics of Circular Breathing in Wind MusiciansDocument8 pagesMechanics of Circular Breathing in Wind MusiciansjwmmdNo ratings yet
- RLE RequirementsDocument24 pagesRLE RequirementsNurhussien GalibNo ratings yet
- Respiratory Rate 4 Breathing Rhythm and Chest MovementDocument2 pagesRespiratory Rate 4 Breathing Rhythm and Chest MovementPriyankaNo ratings yet
- Equipment Used in Physical ExaminationDocument5 pagesEquipment Used in Physical ExaminationMary Kaye Silvestre0% (1)
- Small Animal Cardiology Auscultation - Vet VisionsDocument1 pageSmall Animal Cardiology Auscultation - Vet Visionsyuaifafa25No ratings yet
- Assessment Diagnosis Planning Intervention Rationale Evaluation SubjectiveDocument4 pagesAssessment Diagnosis Planning Intervention Rationale Evaluation Subjectivecammel ramos100% (1)
- Case Scenario 1 Pediatric-Community Acquired Pneumonia P-CapDocument19 pagesCase Scenario 1 Pediatric-Community Acquired Pneumonia P-CapJane LaquihonNo ratings yet
- ?1 - Chest X-Ray Interpretation - A Structured Approach - Radiology - OSCEDocument14 pages?1 - Chest X-Ray Interpretation - A Structured Approach - Radiology - OSCEVerónicaNo ratings yet
- Steps of CPR ProcedureDocument8 pagesSteps of CPR ProcedureKrupa Jyothi PerumallaNo ratings yet
- 44 CPR PDFDocument14 pages44 CPR PDFBramantyo NugrosNo ratings yet
- Difficulty of BreathingDocument4 pagesDifficulty of BreathingNur SetsuNo ratings yet
- 175 Ultrasound in Pregnancy PDFDocument16 pages175 Ultrasound in Pregnancy PDFNestor FerrerNo ratings yet
- NPR Ineffective Airway ClearanceDocument3 pagesNPR Ineffective Airway ClearanceDj KurtNo ratings yet
- Ineffective Breathing PatternDocument3 pagesIneffective Breathing PatternReichelle Perlas62% (13)
- Pi Is 0960982216310557Document2 pagesPi Is 0960982216310557Ridski D. MiruNo ratings yet
- NCP For Scenario BreathingDocument4 pagesNCP For Scenario Breathingmy moznNo ratings yet
- Anatomy and Physiology of The Larynx and Hypopharynx: January 2010Document13 pagesAnatomy and Physiology of The Larynx and Hypopharynx: January 2010Listya ParamitaNo ratings yet
- NCP On Ineffective Airway Clearance Nursing Diagnosi S Planning Nursing Interventions Implementatio N Evaluation Subjective: IndependentDocument10 pagesNCP On Ineffective Airway Clearance Nursing Diagnosi S Planning Nursing Interventions Implementatio N Evaluation Subjective: IndependentSheryhan Tahir BayleNo ratings yet
- Cardio Pulmonary Resuscitation (CPR) : Tracey Gibson, Elaine Cole & Anne McleodDocument6 pagesCardio Pulmonary Resuscitation (CPR) : Tracey Gibson, Elaine Cole & Anne McleodRETINA CREATIONSNo ratings yet
- How To Auscultate For Heart Sounds in Adults: Evidence & PracticeDocument3 pagesHow To Auscultate For Heart Sounds in Adults: Evidence & Practiceangela mamauagNo ratings yet
- Bronkoskopi PediatrikDocument4 pagesBronkoskopi PediatrikAnonymous lSWQIQNo ratings yet
- Ultrasound of The Pediatric Chest2019Document13 pagesUltrasound of The Pediatric Chest2019JHONATAN MATA ARANDANo ratings yet
- F.1 - Respiratory Physio (For Quiz Muna)Document7 pagesF.1 - Respiratory Physio (For Quiz Muna)Mac Vince HipolitoNo ratings yet
- NCP Ineffective Breathing ActualDocument3 pagesNCP Ineffective Breathing ActualArian May Marcos100% (1)
- NCP For PneumoniaDocument3 pagesNCP For PneumoniaLeogalvez BedanoNo ratings yet
- Assignment On Chest PhysiotherapyDocument15 pagesAssignment On Chest PhysiotherapyAxsa AlexNo ratings yet
- Your Airway and Breathing During AnaesthesiaDocument7 pagesYour Airway and Breathing During AnaesthesiagshjfkNo ratings yet
- ABADINGO-Pedia Nursing Care PlanDocument3 pagesABADINGO-Pedia Nursing Care PlanAndrea Abadingo100% (1)
- Acute Respiratory FailureDocument28 pagesAcute Respiratory FailureMohamed Na3eemNo ratings yet
- Session 4 - Performing Respiratory System ExaminationDocument26 pagesSession 4 - Performing Respiratory System ExaminationOtsward OwdenNo ratings yet
- Health AssessmentDocument35 pagesHealth AssessmentKm GaputanNo ratings yet
- Plan of Care Patient Independent-2 PDFDocument1 pagePlan of Care Patient Independent-2 PDFHilary AlvaradoNo ratings yet
- Resp Assessment 2 PDFDocument5 pagesResp Assessment 2 PDFsista mulyaniNo ratings yet
- A Cog Practice Bulletin 175 Ultrasound in PregnancyDocument16 pagesA Cog Practice Bulletin 175 Ultrasound in Pregnancyansel7No ratings yet
- 3-Column Notes 1. What? 2. So What? 3. Now What?: Respiratory SystemDocument1 page3-Column Notes 1. What? 2. So What? 3. Now What?: Respiratory SystemalyssaNo ratings yet
- Seminars in Fetal & Neonatal Medicine: Steven M. Donn, Sunil K. SinhaDocument6 pagesSeminars in Fetal & Neonatal Medicine: Steven M. Donn, Sunil K. SinhadeniNo ratings yet
- NCP NurseryDocument4 pagesNCP NurseryDharwin Nhicko FriasNo ratings yet
- 019 - Ulil Chiqmatuss'diah - KMB 1Document4 pages019 - Ulil Chiqmatuss'diah - KMB 1Setiaty PandiaNo ratings yet
- Simple East Asian Landscape Campaign - by SlidesgoDocument54 pagesSimple East Asian Landscape Campaign - by SlidesgoSetiaty PandiaNo ratings yet
- Patient-Centered Collaborative Care: The Impact of A New Approach To Postpartum Rounds On Residents' Perception of Their Work EnvironmentDocument5 pagesPatient-Centered Collaborative Care: The Impact of A New Approach To Postpartum Rounds On Residents' Perception of Their Work EnvironmentSetiaty PandiaNo ratings yet
- Patient-Centered Collaborative Care: The Impact of A New Approach To Postpartum Rounds On Residents' Perception of Their Work EnvironmentDocument5 pagesPatient-Centered Collaborative Care: The Impact of A New Approach To Postpartum Rounds On Residents' Perception of Their Work EnvironmentSetiaty PandiaNo ratings yet
- Qi Muslimah Talk 1 Ivana FixDocument16 pagesQi Muslimah Talk 1 Ivana FixSetiaty PandiaNo ratings yet
- Jurnal KMB Diva - 015Document10 pagesJurnal KMB Diva - 015Setiaty PandiaNo ratings yet
- 4927 20042 1 PBDocument7 pages4927 20042 1 PBSetiaty PandiaNo ratings yet
- 1385 FullDocument10 pages1385 FullSetiaty PandiaNo ratings yet
- Hubungan Tingkat Kecemasan Dengan Tingkat Kemandirian Activities of Daily Living Pada LansiaDocument8 pagesHubungan Tingkat Kecemasan Dengan Tingkat Kemandirian Activities of Daily Living Pada LansiaSetiaty PandiaNo ratings yet
- JCM 10 00522 v2Document12 pagesJCM 10 00522 v2Setiaty PandiaNo ratings yet
- Health and Quality of Life OutcomesDocument8 pagesHealth and Quality of Life OutcomesSetiaty PandiaNo ratings yet
- Impact of Osteoarthritis On Activities of Daily LiDocument9 pagesImpact of Osteoarthritis On Activities of Daily LiSetiaty PandiaNo ratings yet
- Material - Using Equipment For Patients' Examination - 019 - Ulil ChiqmatussadiahDocument2 pagesMaterial - Using Equipment For Patients' Examination - 019 - Ulil ChiqmatussadiahSetiaty PandiaNo ratings yet
- Alat Ukur Untuk Menilai Kemampuan Fungsional Pasien Dengan Osteoartritis Lutut: Tinjauan PustakaDocument6 pagesAlat Ukur Untuk Menilai Kemampuan Fungsional Pasien Dengan Osteoartritis Lutut: Tinjauan PustakaSetiaty PandiaNo ratings yet
- 116-Article Text-415-1-10-20190507Document8 pages116-Article Text-415-1-10-20190507Setiaty PandiaNo ratings yet
- Faktor-Faktor Yang Berhubungan Dengan Terjadinya PreeklampsiaDocument13 pagesFaktor-Faktor Yang Berhubungan Dengan Terjadinya PreeklampsiaSetiaty PandiaNo ratings yet
- Consulatation Liaison Psychiatry English Lecture 2012 10Document58 pagesConsulatation Liaison Psychiatry English Lecture 2012 10Setiaty PandiaNo ratings yet
- Progress in Disaster Science: Jeremy Spoon, Drew Gerkey, Ram B. Chhetri, Alisa Rai, Umesh Basnet, Chelsea E. HunterDocument15 pagesProgress in Disaster Science: Jeremy Spoon, Drew Gerkey, Ram B. Chhetri, Alisa Rai, Umesh Basnet, Chelsea E. HunterSetiaty PandiaNo ratings yet
- Vital Signs and Monitoring - Podcast - IntermediateDocument4 pagesVital Signs and Monitoring - Podcast - IntermediateSetiaty PandiaNo ratings yet
- Alasan Dilakukannya 4 Kali Amandemen Uud 1945 Tujuan Dan Sejarah PerkembanganDocument11 pagesAlasan Dilakukannya 4 Kali Amandemen Uud 1945 Tujuan Dan Sejarah PerkembanganSetiaty PandiaNo ratings yet
- Deteksi Mycobacterium Tuberculosis Pada Sampel Sputum Menggunakan Teknik Loop-Mediated Isothermal Amplification (LAMP-TB)Document7 pagesDeteksi Mycobacterium Tuberculosis Pada Sampel Sputum Menggunakan Teknik Loop-Mediated Isothermal Amplification (LAMP-TB)Setiaty PandiaNo ratings yet
- Reifika Arfaka Rizieq PSIKA 020Document1 pageReifika Arfaka Rizieq PSIKA 020Setiaty PandiaNo ratings yet
- Reike DIyah Setiawati - 042 - PSIK ADocument28 pagesReike DIyah Setiawati - 042 - PSIK ASetiaty PandiaNo ratings yet
- Assignment (201640031)Document5 pagesAssignment (201640031)Iqtidar KhanNo ratings yet
- Guidelines For Diagnostic Imaging During Pregnancy and Lactation PDFDocument7 pagesGuidelines For Diagnostic Imaging During Pregnancy and Lactation PDFMuhammad nafisNo ratings yet
- Ehs Hospitals All StatesDocument85 pagesEhs Hospitals All Statesnaiduu497No ratings yet
- Goldfarb2020 PDFDocument15 pagesGoldfarb2020 PDFJulia Mar Antonete Tamayo AcedoNo ratings yet
- Jurnal 1Document20 pagesJurnal 1Duvi Ahmad Duvi DekanNo ratings yet
- Physiotherapy For Patients With Sciatica Awaiting Lumbar Micro-Discectomy Surgery - A Nested, Qualitative Study of Patients' Views and ExperiencesDocument10 pagesPhysiotherapy For Patients With Sciatica Awaiting Lumbar Micro-Discectomy Surgery - A Nested, Qualitative Study of Patients' Views and ExperiencesLindapratama SaifuddinNo ratings yet
- MD Radio Diagnosis - Plan of Thesis (Year 2015)Document2 pagesMD Radio Diagnosis - Plan of Thesis (Year 2015)Muhammad UmarNo ratings yet
- Ice Chips GiDocument2 pagesIce Chips GiJANELLE GIFT SENARLONo ratings yet
- Lecture 3 RS12015 PDFDocument136 pagesLecture 3 RS12015 PDFDaniel AshooriNo ratings yet
- Teaching Anxiety Amongst Hong Kong and Shanghai In-Service Teachers: The Impact of Trait Anxiety and Self-EsteemDocument15 pagesTeaching Anxiety Amongst Hong Kong and Shanghai In-Service Teachers: The Impact of Trait Anxiety and Self-Esteemluiza bndlnNo ratings yet
- M. Hill Physiology (16) Regulation of Arterial PressureDocument28 pagesM. Hill Physiology (16) Regulation of Arterial PressureEfrain AnayaNo ratings yet
- What I Know: Quarter 4 - Week No. 5 - 8Document6 pagesWhat I Know: Quarter 4 - Week No. 5 - 8Dianne GarciaNo ratings yet
- Om 1531026 0102Document270 pagesOm 1531026 0102chinh nguyenNo ratings yet
- Bahasa InggrisDocument4 pagesBahasa InggrisKimiaDinaa Ulayaa Aqilatun NajlaaNo ratings yet
- Jupiter Plus: Anaesthesia WorkstationDocument4 pagesJupiter Plus: Anaesthesia WorkstationXavier Med Pvt. LtdNo ratings yet
- Starting The ResearchDocument39 pagesStarting The ResearchMargaux LucasNo ratings yet
- El Salvador Conference Gang Prevention in USDocument22 pagesEl Salvador Conference Gang Prevention in USjosetanoNo ratings yet
- An Investigation Into The Barriers To and Priorities For Research Engagement in Health LibrarianshipDocument22 pagesAn Investigation Into The Barriers To and Priorities For Research Engagement in Health LibrarianshipKrisha FernandezNo ratings yet
- SS3 Scheme of WorkDocument136 pagesSS3 Scheme of WorkVictory OjugbaNo ratings yet
- A Coaches ResponsibilityDocument10 pagesA Coaches ResponsibilityCorteza, Ricardo Danilo E. UnknownNo ratings yet
- Quick Glance: Deciding Which Teletherapy Model Is Appropriate Related Services (SLP, OT, PT, AT, Behavior)Document2 pagesQuick Glance: Deciding Which Teletherapy Model Is Appropriate Related Services (SLP, OT, PT, AT, Behavior)Madhu sudarshan ReddyNo ratings yet
- Per Dev Module 4Document8 pagesPer Dev Module 4Marciana JulianNo ratings yet
- Personal Stress Management Surviving To Thriving 1st Edition Ebook PDF VersionDocument58 pagesPersonal Stress Management Surviving To Thriving 1st Edition Ebook PDF Versionronald.robotham75498% (41)
- Barry, M. (2010) Summary and Note Taking (Pp.8-11) Revised Edition Cambridge-University-PressDocument6 pagesBarry, M. (2010) Summary and Note Taking (Pp.8-11) Revised Edition Cambridge-University-Presshochjon60% (5)
- Jha Rig Up Hwu Equipment & Surface Line N-U and N-D BopDocument7 pagesJha Rig Up Hwu Equipment & Surface Line N-U and N-D BopHSE PULAI A100% (1)
- Mapeh 6 Week 8.....Document4 pagesMapeh 6 Week 8.....Edmar MejiaNo ratings yet
- Volunteer HandbookDocument23 pagesVolunteer HandbookTom HallNo ratings yet
- Code of Ethics For UIPE MembersDocument53 pagesCode of Ethics For UIPE Membersultra engineeringltdNo ratings yet
- Practical Research 2: Quarter 1 Module 1 (Week 1) : Performing Hair and Scalp TreatmentDocument19 pagesPractical Research 2: Quarter 1 Module 1 (Week 1) : Performing Hair and Scalp TreatmentAnalie CabanlitNo ratings yet
- Use of Oral Sucrose 08Document16 pagesUse of Oral Sucrose 08madimadi11No ratings yet
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (5)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (39)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 4 out of 5 stars4/5 (5)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 4.5 out of 5 stars4.5/5 (84)
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)From EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Rating: 3 out of 5 stars3/5 (1)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (404)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeRating: 2 out of 5 stars2/5 (1)
- The Twentysomething Treatment: A Revolutionary Remedy for an Uncertain AgeFrom EverandThe Twentysomething Treatment: A Revolutionary Remedy for an Uncertain AgeRating: 4.5 out of 5 stars4.5/5 (3)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (44)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (267)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (170)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- I Shouldn't Feel This Way: Name What’s Hard, Tame Your Guilt, and Transform Self-Sabotage into Brave ActionFrom EverandI Shouldn't Feel This Way: Name What’s Hard, Tame Your Guilt, and Transform Self-Sabotage into Brave ActionNo ratings yet
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (46)
- Critical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsFrom EverandCritical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsRating: 4.5 out of 5 stars4.5/5 (39)
- The Fun Habit: How the Pursuit of Joy and Wonder Can Change Your LifeFrom EverandThe Fun Habit: How the Pursuit of Joy and Wonder Can Change Your LifeRating: 4.5 out of 5 stars4.5/5 (19)
- Manipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesFrom EverandManipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesRating: 4.5 out of 5 stars4.5/5 (1412)
- Summary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedRating: 4 out of 5 stars4/5 (11)
- Dark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingFrom EverandDark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingRating: 4 out of 5 stars4/5 (1138)
- The Story of Philosophy: The Lives and Opinions of the Greater PhilosophersFrom EverandThe Story of Philosophy: The Lives and Opinions of the Greater PhilosophersNo ratings yet