You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Effect of Lockdown On Health Profile of Medical Students of AssamDocument15 pagesEffect of Lockdown On Health Profile of Medical Students of AssamArpana HazarikaNo ratings yet
- Effect of Lockdown On Health Profile of Medical Students of AssamDocument18 pagesEffect of Lockdown On Health Profile of Medical Students of AssamArpana HazarikaNo ratings yet
- Aetcom: DR Arpana HazarikaDocument2 pagesAetcom: DR Arpana HazarikaArpana HazarikaNo ratings yet
- Posture and EquilibiriumDocument71 pagesPosture and EquilibiriumArpana HazarikaNo ratings yet
- Homeostasis: DR Arpana Hazarika Associate Prof Dept of PhysiologyDocument29 pagesHomeostasis: DR Arpana Hazarika Associate Prof Dept of PhysiologyArpana HazarikaNo ratings yet
- LockdownDocument5 pagesLockdownArpana HazarikaNo ratings yet
- Coronavirus Second WaveDocument3 pagesCoronavirus Second WaveArpana HazarikaNo ratings yet
- Perception and Knowledge of First Year MBBS Students Towards E Learning A Cross Sectional StudyDocument4 pagesPerception and Knowledge of First Year MBBS Students Towards E Learning A Cross Sectional StudyArpana HazarikaNo ratings yet
- 4956-Article Text-9519-1-10-20210105Document14 pages4956-Article Text-9519-1-10-20210105Arpana HazarikaNo ratings yet
- Association Between ABO Blood Groups and Susceptibility To COVID 19Document4 pagesAssociation Between ABO Blood Groups and Susceptibility To COVID 19Arpana HazarikaNo ratings yet
- DR - ShrutiNagar (IMDR)Document1 pageDR - ShrutiNagar (IMDR)Arpana HazarikaNo ratings yet
- DownloadDocument5 pagesDownloadArpana HazarikaNo ratings yet
- Religious Places of Assam: One Must SeeDocument3 pagesReligious Places of Assam: One Must SeeArpana HazarikaNo ratings yet
- Cardiac Muscle: Dr. Mohammed Abdul Hannan HazariDocument24 pagesCardiac Muscle: Dr. Mohammed Abdul Hannan HazariArpana HazarikaNo ratings yet
- A Trip To Dibru Saikhowa National ParkDocument2 pagesA Trip To Dibru Saikhowa National ParkArpana HazarikaNo ratings yet
- Glimpses of Assam The Land Od Red River and Blue HillsDocument7 pagesGlimpses of Assam The Land Od Red River and Blue HillsArpana HazarikaNo ratings yet
- Study Plan and Projects ManagementDocument9 pagesStudy Plan and Projects ManagementArpana HazarikaNo ratings yet
- A Comparative Study of Pulmonary Function Among TheDocument22 pagesA Comparative Study of Pulmonary Function Among TheArpana HazarikaNo ratings yet
- Qualitative Research Methods - An OverviewDocument9 pagesQualitative Research Methods - An OverviewArpana HazarikaNo ratings yet
- Preparing A Concept PaperDocument10 pagesPreparing A Concept PaperArpana HazarikaNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Why Small Retailers Endure in Latin AmericaDocument16 pagesWhy Small Retailers Endure in Latin AmericaAhmed SamirNo ratings yet
- Sarahdhobhany Resume PDFDocument1 pageSarahdhobhany Resume PDFAnonymous Uz535ScEMVNo ratings yet
- SBN 1188 - LPG BillDocument35 pagesSBN 1188 - LPG BillJoy AcostaNo ratings yet
- Development Plan: Jawaharlal Nehru Architecture and Fine Arts UniversityDocument13 pagesDevelopment Plan: Jawaharlal Nehru Architecture and Fine Arts Universityrenikunta varshiniNo ratings yet
- Dressmaking NC Ii (320 HRS)Document8 pagesDressmaking NC Ii (320 HRS)Amir Hasan Nicko BaidanNo ratings yet
- AT&T Case StudyDocument9 pagesAT&T Case StudyAdrian DsouzaNo ratings yet
- Identifying and Empowering Instructional Leaders - e JunkDocument6 pagesIdentifying and Empowering Instructional Leaders - e Junkapi-520247537No ratings yet
- Ogl 481 - Project Management Article - Ogl 320 Project Management Module 7 PaperDocument1 pageOgl 481 - Project Management Article - Ogl 320 Project Management Module 7 Paperapi-513938901No ratings yet
- Poverty ResearchDocument9 pagesPoverty ResearchBravo,Jessy Anne G.No ratings yet
- Terraplus Presentation For KSA My VersionDocument13 pagesTerraplus Presentation For KSA My VersionAbed Fattah MuribyNo ratings yet
- AOT Traffic Report-2018Document252 pagesAOT Traffic Report-2018Egsiam SaotonglangNo ratings yet
- ARTMATTERS at Art Center College of Design: Curricular Notes On Art Practice, Place, and Social EngagementDocument17 pagesARTMATTERS at Art Center College of Design: Curricular Notes On Art Practice, Place, and Social EngagementFelcina RayenNo ratings yet
- Advertisement For Apprenticeship 57th BatchDocument2 pagesAdvertisement For Apprenticeship 57th BatchTalha IshaqNo ratings yet
- Pass Format From Police StationDocument1 pagePass Format From Police StationThe Indian Express83% (6)
- Mistake and Non-Disclosure of Facts Models For English Contract Law (PDFDrive)Document172 pagesMistake and Non-Disclosure of Facts Models For English Contract Law (PDFDrive)Anonymous 94TBTBRksNo ratings yet
- Laws, Policies & Programs For Philippine WomenDocument38 pagesLaws, Policies & Programs For Philippine WomenAngel Marie Rule100% (1)
- Final 2019sqyfergusonresume 5Document2 pagesFinal 2019sqyfergusonresume 5api-357486179No ratings yet
- Passed CGPA-7.2: Rohit Kumar Singh At-Plot-28 Vasundhara Vihar Society Iit Gate Kalyanpur Kanpur PIN-208017 (U.P)Document2 pagesPassed CGPA-7.2: Rohit Kumar Singh At-Plot-28 Vasundhara Vihar Society Iit Gate Kalyanpur Kanpur PIN-208017 (U.P)Rohit Singh100% (1)
- DOT PuzzleDocument2 pagesDOT Puzzledesai628No ratings yet
- EXTAC - 1010 - Rev - NONCOMBATANT EVACUATION OPERATIONSDocument96 pagesEXTAC - 1010 - Rev - NONCOMBATANT EVACUATION OPERATIONSAbrarNo ratings yet
- Karte Za Crnu Goru (Eurocode)Document19 pagesKarte Za Crnu Goru (Eurocode)Vahid100% (1)
- Student - Marksheet - OpticsDocument7 pagesStudent - Marksheet - OpticsNguyệt PhươngNo ratings yet
- Group 4 Smith Speech Analysis Task 2-2Document4 pagesGroup 4 Smith Speech Analysis Task 2-2api-551088311No ratings yet
- MSC Circ 1111Document36 pagesMSC Circ 1111Vincent Paul SantosNo ratings yet
- First Division (G.R. No. 163504, August 05, 2015)Document12 pagesFirst Division (G.R. No. 163504, August 05, 2015)JB AndesNo ratings yet
- Crafting StrategyDocument16 pagesCrafting StrategyKathlynJoySalazarNo ratings yet
- Philosophy of CaringDocument8 pagesPhilosophy of CaringKaye Cor100% (1)
- Au 3Document138 pagesAu 3Alejandra CastilloNo ratings yet
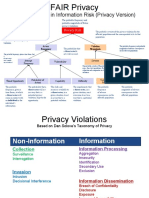
- Factor Analysis in Information Risk (Privacy Version)Document8 pagesFactor Analysis in Information Risk (Privacy Version)Otgonbayar TsengelNo ratings yet
- FMS Information Bulletin 2008Document52 pagesFMS Information Bulletin 2008meenana100% (2)