You might also like
- Maths - Stage 4 - 01 - 7RP - AFP - tcm142-639560Document14 pagesMaths - Stage 4 - 01 - 7RP - AFP - tcm142-639560Danquah Kumi100% (3)
- Rationalization of Shape and Related Stress Distribution in Posterior Teeth: A Finite Element Study Using Nonlinear Contact AnalysisDocument9 pagesRationalization of Shape and Related Stress Distribution in Posterior Teeth: A Finite Element Study Using Nonlinear Contact AnalysisAnderson ChamblasNo ratings yet
- Case Study# 1: Nothing Unique To OfferDocument2 pagesCase Study# 1: Nothing Unique To Offeranaliza CabilosNo ratings yet
- Rotary Gingival CurettageDocument27 pagesRotary Gingival CurettageSebastián BernalNo ratings yet
- Surgical Treatment of Periimplantitis With Non - Augmentative TechniquesDocument10 pagesSurgical Treatment of Periimplantitis With Non - Augmentative Techniquesmelissa.aa.melissaNo ratings yet
- Treatment of Fingertip Injuries 2020Document9 pagesTreatment of Fingertip Injuries 2020Oscar Cayetano Herrera RodríguezNo ratings yet
- Crown LengtheningDocument11 pagesCrown LengtheningVictoria ChenNo ratings yet
- JOP Case Report SampleDocument11 pagesJOP Case Report Samplekathryn ongNo ratings yet
- Master ArticleDocument8 pagesMaster ArticleDr. DeeptiNo ratings yet
- TLIF Approaches ExplainedDocument8 pagesTLIF Approaches ExplainedAlex Cortes100% (1)
- Case Series: Focus On Epithelialized Palatal Grafts. Part 2: Implant Site DevelopmentDocument10 pagesCase Series: Focus On Epithelialized Palatal Grafts. Part 2: Implant Site DevelopmentCristhian Condori SarmientoNo ratings yet
- Osseodensification in Implant Dentistry A.12Document7 pagesOsseodensification in Implant Dentistry A.12ASJADI SHEIKHNo ratings yet
- The International Journal of Periodontics & Restorative DentistryDocument8 pagesThe International Journal of Periodontics & Restorative DentistrySeptimiu TiplicaNo ratings yet
- Periosteum Classification and Flap AdvancementDocument9 pagesPeriosteum Classification and Flap AdvancementAlNo ratings yet
- Osseodensification in Implant Dentistry A.12Document7 pagesOsseodensification in Implant Dentistry A.12MilindNo ratings yet
- Root Reshaping: An Integral Component of Periodontal SurgeryDocument9 pagesRoot Reshaping: An Integral Component of Periodontal SurgeryANDREANo ratings yet
- Insight March 2016 Special EditionDocument15 pagesInsight March 2016 Special EditionbosanNo ratings yet
- Three Dimensional Evaluation On The Effect Of.7Document6 pagesThree Dimensional Evaluation On The Effect Of.7MariyamNo ratings yet
- Germline Modification and The Burden of Human ExistenceDocument13 pagesGermline Modification and The Burden of Human ExistencexdetNo ratings yet
- Ajr-Mucocele AppendixDocument4 pagesAjr-Mucocele AppendixOrlin Zlatarski100% (1)
- Influence of Implant Length and Associated Parameters Upon Biomechanical Forces in Finite Element Analyses - A Systematic Review. Implant Dent, 2019Document10 pagesInfluence of Implant Length and Associated Parameters Upon Biomechanical Forces in Finite Element Analyses - A Systematic Review. Implant Dent, 2019Marlene Kasumi Gantier TakanoNo ratings yet
- Metformin and The Risk of Dementia in Type 2 Diabetes PatientsDocument12 pagesMetformin and The Risk of Dementia in Type 2 Diabetes PatientsMorindaNo ratings yet
- NehruDocument16 pagesNehruAkanksha. KNo ratings yet
- Ahmed ENDO Vol6 Iss2Document18 pagesAhmed ENDO Vol6 Iss2Lupu SebastianNo ratings yet
- Esthetic Complications P2000Document13 pagesEsthetic Complications P2000Freddy BenalcázarNo ratings yet
- Worksheet in Media and Information Literacy Introduction To Media and Information LiteracyDocument2 pagesWorksheet in Media and Information Literacy Introduction To Media and Information LiteracyDJazel TolentinoNo ratings yet
- SJ BDJ 2014 354Document8 pagesSJ BDJ 2014 354aziz alsohailNo ratings yet
- Of A of of of A A of A: THE OF THE Project Chile NefDocument15 pagesOf A of of of A A of A: THE OF THE Project Chile NefEmilianoNo ratings yet
- 1 PDFDocument12 pages1 PDFEvelyn YGNo ratings yet
- Pilon Fractures Preventing ComplicationsDocument12 pagesPilon Fractures Preventing ComplicationsjojoNo ratings yet
- PRD 22 5 Magne1Document10 pagesPRD 22 5 Magne1sofa83No ratings yet
- Reviewer MILDocument2 pagesReviewer MILnaborcarleugeneNo ratings yet
- DT Asia Pacific No 5 2013 0513 (04 04)Document1 pageDT Asia Pacific No 5 2013 0513 (04 04)SkAliHassanNo ratings yet
- 10 11607@prd 00 0454Document8 pages10 11607@prd 00 0454Alejandro FereñoNo ratings yet
- Short Implants Versus Standard Implants Midterm.18Document6 pagesShort Implants Versus Standard Implants Midterm.18Almendra AliagaNo ratings yet
- Tile Internationai Journal of Periadantics & Restorative DentistryDocument13 pagesTile Internationai Journal of Periadantics & Restorative DentistryAna Maria Montoya GomezNo ratings yet
- Management of A Coronally Advanced Lingual Flap in Regenerative Osseous Surgery: A Case Series Introducing A Novel TechniqueDocument11 pagesManagement of A Coronally Advanced Lingual Flap in Regenerative Osseous Surgery: A Case Series Introducing A Novel TechniqueAnita PrastiwiNo ratings yet
- World Declaration On Dam Safety - ICOLD - A3Document2 pagesWorld Declaration On Dam Safety - ICOLD - A3cgloriaoNo ratings yet
- Intramedullary Nailing of Femoral Shaft Fractures .4Document10 pagesIntramedullary Nailing of Femoral Shaft Fractures .4DavidBeatonComuladaNo ratings yet
- Cell MigrationDocument3 pagesCell MigrationjackyxtremNo ratings yet
- Fingertip Injuries PDFDocument12 pagesFingertip Injuries PDFZóélkårnåín PhåntómhívéNo ratings yet
- Andrew 1994Document15 pagesAndrew 1994Néia CostaNo ratings yet
- PASS Principles For Predictable Bone.8Document10 pagesPASS Principles For Predictable Bone.8Alex Martins AlbaneseNo ratings yet
- Repair of Soft Tissue-Root Interfase by Stahl (1977)Document8 pagesRepair of Soft Tissue-Root Interfase by Stahl (1977)AndrésRodolfoLozanoLeivaNo ratings yet
- A Complete Subperichondrial Dissection Technique For Rhinoplasty With Management of The Nasal LigamentsDocument11 pagesA Complete Subperichondrial Dissection Technique For Rhinoplasty With Management of The Nasal LigamentsМаратNo ratings yet
- X.9. - A Contemporary ReviewDocument8 pagesX.9. - A Contemporary ReviewReine BritoNo ratings yet
- Nanomaterials 10 00016Document17 pagesNanomaterials 10 00016Brunna NobregaNo ratings yet
- How To Get The Most Out of Your Gastrocnemius And.3Document5 pagesHow To Get The Most Out of Your Gastrocnemius And.3Sisay GirmaNo ratings yet
- The Peri-Implant Zone - A Review of LiteratureDocument7 pagesThe Peri-Implant Zone - A Review of LiteratureJuanOso Gutierrez ArayaNo ratings yet
- Risk of Infection Is Associated More With Drain.81Document6 pagesRisk of Infection Is Associated More With Drain.81BABANG GAGAHNo ratings yet
- 1020 FullDocument11 pages1020 FullNatalija MinicNo ratings yet
- A - UPTON 1993 - The Tradition of ChangeDocument8 pagesA - UPTON 1993 - The Tradition of ChangeGiana Flores Das PedrasNo ratings yet
- Aslan 2017Document8 pagesAslan 2017Ana Maria Montoya GomezNo ratings yet
- Etm 2010 8 31 10Document1 pageEtm 2010 8 31 10Jess JoseNo ratings yet
- Transport in Plants - Micronotes by Seep PahujaDocument2 pagesTransport in Plants - Micronotes by Seep PahujamanojchodharyhathrasNo ratings yet
- Kilt University: Bhubaneswar, Odisha, IndiaDocument48 pagesKilt University: Bhubaneswar, Odisha, IndiaTesfaye Teferi ShoneNo ratings yet
- Subperiostial Minimally Invasive Aesthetic Ridge Augmentation Technique (SMART)Document10 pagesSubperiostial Minimally Invasive Aesthetic Ridge Augmentation Technique (SMART)Pat TellezNo ratings yet
- Prosthodontic Rehabilitation of Cleft Lip and Palate With Presurgical Nasoalveolar MoldingDocument3 pagesProsthodontic Rehabilitation of Cleft Lip and Palate With Presurgical Nasoalveolar MoldingVasantha RajanNo ratings yet
- Harvesting Rib Cartilage Grafts For Secondary Rhinoplasty: Background: MethodsDocument7 pagesHarvesting Rib Cartilage Grafts For Secondary Rhinoplasty: Background: MethodsLuiggi Fayad100% (1)
- Business CommDocument11 pagesBusiness CommMishri JoshiNo ratings yet
- Principles For Vertical Ridge Augmentation in The Atrophic Posterior Mandible - A Technical Review - Urban2017Document8 pagesPrinciples For Vertical Ridge Augmentation in The Atrophic Posterior Mandible - A Technical Review - Urban2017Claudio GuzmanNo ratings yet
- Chromosome identification: Medicine and Natural Sciences: Medicine and Natural SciencesFrom EverandChromosome identification: Medicine and Natural Sciences: Medicine and Natural SciencesTorbjoern CasperssonNo ratings yet
- Mtravers Resume 201820181104-1-1qhyuhjDocument1 pageMtravers Resume 201820181104-1-1qhyuhjapi-445643461No ratings yet
- Ratio DecidendiDocument12 pagesRatio DecidendiAbhidhaNo ratings yet
- MAE 4281 Homework #6: Xy X yDocument3 pagesMAE 4281 Homework #6: Xy X ydadaNo ratings yet
- MDVR-Ceiba Video Management Software User ManualDocument27 pagesMDVR-Ceiba Video Management Software User ManualTTB Vision0% (1)
- MAS-42F (Relevant Costing With Linear Programming)Document9 pagesMAS-42F (Relevant Costing With Linear Programming)Pearl Mae De VeasNo ratings yet
- ASTM D 1883-16 CBR California Bearing Ratio 6Document1 pageASTM D 1883-16 CBR California Bearing Ratio 6Candice PersadNo ratings yet
- The Cognitive Distortions of Child Sexual AbuserDocument16 pagesThe Cognitive Distortions of Child Sexual AbuserAngela Alejandra Castro HerreraNo ratings yet
- Allie Brown: Southern Paws Pet Grooming, Cordele, GA. - BatherDocument2 pagesAllie Brown: Southern Paws Pet Grooming, Cordele, GA. - Batherapi-548153301No ratings yet
- Assessment & AuditDocument24 pagesAssessment & Audit9punitagrawalNo ratings yet
- "Mental Fitness For Traders" by Norman HalletDocument35 pages"Mental Fitness For Traders" by Norman Halletapi-26247058100% (2)
- Theodore Roosevelt Imperialist or GlobalDocument20 pagesTheodore Roosevelt Imperialist or GlobalBojan BojićNo ratings yet
- Viktorijanska Književnost - SkriptaDocument53 pagesViktorijanska Književnost - SkriptagigaweaponNo ratings yet
- 1.-Apoyo Lectura - Introducción A La Programación - LISTODocument287 pages1.-Apoyo Lectura - Introducción A La Programación - LISTOmercedes claudia alberto ponceNo ratings yet
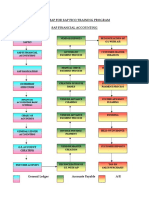
- Roadmap For SAP FICO Training ProgramDocument4 pagesRoadmap For SAP FICO Training ProgramCorpsalesNo ratings yet
- Design Report of Compound WallDocument30 pagesDesign Report of Compound WallSivamurugan SivanayagamNo ratings yet
- Engro FoodsDocument28 pagesEngro FoodshunzakhalidNo ratings yet
- FMFRP+6 90 1+Tow+Weapon+SystemDocument192 pagesFMFRP+6 90 1+Tow+Weapon+SystemTenshiJibrilNo ratings yet
- 16s - Wiring Diagram - Package Insert v16.1Document2 pages16s - Wiring Diagram - Package Insert v16.1Harold MontesNo ratings yet
- Ecological InventoryDocument3 pagesEcological InventoryStephanie Hanson100% (1)
- Approaches To Study Economic GeographyDocument5 pagesApproaches To Study Economic Geographyjainaastha28_1951858100% (3)
- The Impact of Social Media On College Mental Health During The COVID 19 Pandemic: A Multinational Review of The Existing LiteratureDocument12 pagesThe Impact of Social Media On College Mental Health During The COVID 19 Pandemic: A Multinational Review of The Existing LiteraturesittieraihanienNo ratings yet
- Basic Uses of English TensesDocument5 pagesBasic Uses of English TensesAjal PNo ratings yet
- Ethiopia - Addis Hiwot Center of The BlindDocument20 pagesEthiopia - Addis Hiwot Center of The BlindMike WalshNo ratings yet
- Chapter 14. Intestinal GasDocument19 pagesChapter 14. Intestinal GasMonica CiorneiNo ratings yet
- 12th April 2015 - Bulletin #164 - Second Sunday of Easter Divine Mercy SundayDocument8 pages12th April 2015 - Bulletin #164 - Second Sunday of Easter Divine Mercy SundaySanta Sophia Catholic ChurchNo ratings yet
- Bretton WoodsDocument3 pagesBretton Woodsdeepakchoubey90No ratings yet
- Iceberg Model of CultureDocument4 pagesIceberg Model of CultureafiqahNo ratings yet
- Ligia Dorina CREMENE: Associate ProfessorDocument3 pagesLigia Dorina CREMENE: Associate ProfessorEmoke SzekelyNo ratings yet