You might also like
- Complementary and Alternative Medical Lab Testing Part 6: Liver and GallbladderFrom EverandComplementary and Alternative Medical Lab Testing Part 6: Liver and GallbladderNo ratings yet
- Jurnal NorvascDocument8 pagesJurnal NorvascYoung AjjaNo ratings yet
- 5 PharmacologyDocument4 pages5 Pharmacologyshiv_prhNo ratings yet
- Population Pharmacokinetics of Valproic Acid in Patients With Mania: Implication For Individualized Dosing RegimensDocument11 pagesPopulation Pharmacokinetics of Valproic Acid in Patients With Mania: Implication For Individualized Dosing RegimensKelletCadilloBarruetoNo ratings yet
- Asam ValproatDocument8 pagesAsam Valproatshellydooong193No ratings yet
- Valproic Acid in Epilepsy: Clinical and Pharmacological EffectsDocument6 pagesValproic Acid in Epilepsy: Clinical and Pharmacological EffectsadityaNo ratings yet
- TCI Propofol ClearanceDocument9 pagesTCI Propofol ClearanceJoanna GlezNo ratings yet
- 10.1515 - CCLM 2015 0591Document7 pages10.1515 - CCLM 2015 0591fsafNo ratings yet
- Carnahan2006 (ADS)Document7 pagesCarnahan2006 (ADS)arslaneNo ratings yet
- Non-Linear PharmacokineticsDocument6 pagesNon-Linear PharmacokineticsaristapasisingiNo ratings yet
- Jurnal LisinoprilDocument7 pagesJurnal LisinoprildidiisafitriNo ratings yet
- Population Pharmacokinetics of Cyclosporine in Chinese Cardiac Transplant RecipientsDocument8 pagesPopulation Pharmacokinetics of Cyclosporine in Chinese Cardiac Transplant RecipientsGifari Muhammad SyabaNo ratings yet
- Therapeutic Drug Monitoring of Levetiracetam in Daily Clinical Practice: High-Performance Liquid Chromatography Versus ImmunoassayDocument5 pagesTherapeutic Drug Monitoring of Levetiracetam in Daily Clinical Practice: High-Performance Liquid Chromatography Versus ImmunoassayMaria MendozaNo ratings yet
- Markovitz2002 Risp+Probenecid RCTDocument9 pagesMarkovitz2002 Risp+Probenecid RCTIulia CiocotisanNo ratings yet
- Lopinavir Ritonavir Pharmacokinetic Profile Impact of Sex and Other CovariatesDocument9 pagesLopinavir Ritonavir Pharmacokinetic Profile Impact of Sex and Other CovariatesLuciana OliveiraNo ratings yet
- Pec or I Giraldi 2011Document8 pagesPec or I Giraldi 2011Александр ОсобаNo ratings yet
- Cheung 1988Document3 pagesCheung 1988Vanessa S DanielNo ratings yet
- Avaliacao Doses FarmacoindutoresDocument7 pagesAvaliacao Doses FarmacoindutoresEnzoNo ratings yet
- Pharmacokinetics, Pharmacodynamics, and Safety of Apixaban in Subjects With End-Stage Renal Disease On HemodialysisDocument9 pagesPharmacokinetics, Pharmacodynamics, and Safety of Apixaban in Subjects With End-Stage Renal Disease On HemodialysisAnonymous S8bsuMNo ratings yet
- IJBMS Volume 12 Issue 3 Pages 146-149Document4 pagesIJBMS Volume 12 Issue 3 Pages 146-149TanveerNo ratings yet
- Accuracy of Calculated Free Valproate LevelsDocument9 pagesAccuracy of Calculated Free Valproate LevelskelracheltwrNo ratings yet
- 81635793Document13 pages81635793Brock TernovNo ratings yet
- Single-Dose and Multiple-Dose Pharmacokinetics of Zaltoprofen After Oral Administration in Healthy Chinese VolunteersDocument7 pagesSingle-Dose and Multiple-Dose Pharmacokinetics of Zaltoprofen After Oral Administration in Healthy Chinese VolunteersSonia BaruaNo ratings yet
- Choi2014 231128 194257Document13 pagesChoi2014 231128 194257TaraaNo ratings yet
- The Pharmacodynamics and Pharmacokinetics of Mivacurium in ChildrenDocument7 pagesThe Pharmacodynamics and Pharmacokinetics of Mivacurium in ChildrenluyawinNo ratings yet
- Comparative in Vitro Dissolution and in Vivo Bioequivalence of Two Diclofenac Enteric Coated FormulationsDocument5 pagesComparative in Vitro Dissolution and in Vivo Bioequivalence of Two Diclofenac Enteric Coated FormulationsgeoaislaNo ratings yet
- Arp2018 1486261Document5 pagesArp2018 1486261Sheren ElinNo ratings yet
- HindawiDocument6 pagesHindawiTaufiqo Nugraha SjachrilNo ratings yet
- Bauch-Atrial Natriuretic Peptide As A MarDocument6 pagesBauch-Atrial Natriuretic Peptide As A MarSzendeNo ratings yet
- In Uence of Cancer Cachexia On Drug Liver Metabolism and Renal Elimination in RatsDocument8 pagesIn Uence of Cancer Cachexia On Drug Liver Metabolism and Renal Elimination in RatsGregorius HocevarNo ratings yet
- Monitoring Unbound Valproic Acid Concentration in Patients With Hypoalbuminemia 2019 PDFDocument20 pagesMonitoring Unbound Valproic Acid Concentration in Patients With Hypoalbuminemia 2019 PDFCESAR AUGUSTO CARVAJAL RENDONNo ratings yet
- Metabolism, Excretion, and Pharmacokinetics of Selumetinib, An MEK1/2 Inhibitor, in Healthy Adult Male SubjectsDocument33 pagesMetabolism, Excretion, and Pharmacokinetics of Selumetinib, An MEK1/2 Inhibitor, in Healthy Adult Male SubjectsAndi wahyuniNo ratings yet
- Captopril: Determination in Blood and Pharmacokinetics After Single Oral DoseDocument6 pagesCaptopril: Determination in Blood and Pharmacokinetics After Single Oral DoseKhintan Risky FadhilaNo ratings yet
- Hemolysis of Blood Samples Has No Significant Impact On The Results of Pharmacokinetic DataDocument4 pagesHemolysis of Blood Samples Has No Significant Impact On The Results of Pharmacokinetic DataDiego OrtechoNo ratings yet
- RARE & Orphan Diseases - Clinical OutcomesDocument2 pagesRARE & Orphan Diseases - Clinical OutcomesMichael John AguilarNo ratings yet
- A Theoretical Method For Normalizing Total Serum Valproic Acid Concentration in Hypoalbuminemic PatientsDocument5 pagesA Theoretical Method For Normalizing Total Serum Valproic Acid Concentration in Hypoalbuminemic Patientsmarc daouNo ratings yet
- Reed 2006Document6 pagesReed 2006Nando EllaNo ratings yet
- Loop Diuretic Prescription and Long-Term Outcomes in Heart Failure: Association Modification by CongestionDocument8 pagesLoop Diuretic Prescription and Long-Term Outcomes in Heart Failure: Association Modification by CongestionfathiNo ratings yet
- 2006 Anaesth Intensive CareDocument5 pages2006 Anaesth Intensive CareAirwayNo ratings yet
- Caso Clinico 3Document10 pagesCaso Clinico 3Rosa ArrascueNo ratings yet
- Atrial Natriuretic Peptide For Management of Acute Kidney InjuryDocument12 pagesAtrial Natriuretic Peptide For Management of Acute Kidney InjuryHadsfrv KajdgygNo ratings yet
- Insulin Degludec - Pharmacokinetic Properties in Subjects With Hepatic ImpairmentDocument7 pagesInsulin Degludec - Pharmacokinetic Properties in Subjects With Hepatic ImpairmentThúy Trang PhanNo ratings yet
- 2 PDFDocument6 pages2 PDFLisa HikmawanNo ratings yet
- Ba StudyDocument13 pagesBa StudyDRx Sonali TareiNo ratings yet
- Pirhadi-Tavandashti 2020Document7 pagesPirhadi-Tavandashti 2020徳利雅No ratings yet
- ADN MitocondrialDocument13 pagesADN MitocondrialChristopher Ramos GuzmánNo ratings yet
- Does The Central Venous Pressure Predict Fluid Responsiveness? An Updated Meta-Analysis and A Plea For Some Common SenseDocument8 pagesDoes The Central Venous Pressure Predict Fluid Responsiveness? An Updated Meta-Analysis and A Plea For Some Common SenseCris TianNo ratings yet
- Antinuclear Antibodies by Indirect Immunofluorescence: Optimum Screening Dilution For Diagnosis of Systemic Lupus ErythematosusDocument5 pagesAntinuclear Antibodies by Indirect Immunofluorescence: Optimum Screening Dilution For Diagnosis of Systemic Lupus ErythematosusMargriet MayasinNo ratings yet
- Estudio Sobre DiabetesDocument5 pagesEstudio Sobre DiabetesGloria María De León MancillasNo ratings yet
- Research Paper: NeuropsychiatryDocument11 pagesResearch Paper: NeuropsychiatryveerrajuNo ratings yet
- Yerino 2011Document6 pagesYerino 2011Antonio SanchezNo ratings yet
- Chertow Et AlDocument12 pagesChertow Et AlsheharyarNo ratings yet
- Gauthier 1992Document6 pagesGauthier 1992hectorNo ratings yet
- Influence of Everolimus On Steady-State Pharmacokinetics of CyclosporineDocument12 pagesInfluence of Everolimus On Steady-State Pharmacokinetics of CyclosporineLuciana OliveiraNo ratings yet
- Caspofungin Population Pharmacokinetics in Critically Ill Patients Undergoing Continuous Veno-Venous Haemofiltration or HaemodiafiltrationDocument12 pagesCaspofungin Population Pharmacokinetics in Critically Ill Patients Undergoing Continuous Veno-Venous Haemofiltration or HaemodiafiltrationNguyễn LongNo ratings yet
- Nephrology: Edward F. Foote, Pharm.D., FCCP, BCPSDocument32 pagesNephrology: Edward F. Foote, Pharm.D., FCCP, BCPSandirio7486No ratings yet
- Revision CiticolinaDocument20 pagesRevision CiticolinaIhdhar NursNo ratings yet
- 1 s2.0 S0254627215300418 MainDocument11 pages1 s2.0 S0254627215300418 MainasdNo ratings yet
- Renal Pharmacotherapy: Dosage Adjustment of Medications Eliminated by the KidneysFrom EverandRenal Pharmacotherapy: Dosage Adjustment of Medications Eliminated by the KidneysNo ratings yet
- Approval Romania 2008Document27 pagesApproval Romania 2008Andrés Domínguez RuizNo ratings yet
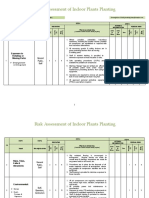
- Risk Assessment of Indoor Plants PlantingDocument5 pagesRisk Assessment of Indoor Plants Plantingطارق رضوانNo ratings yet
- Neurologic AssessmentDocument29 pagesNeurologic AssessmentJoessel_Marie__8991100% (1)
- Periodontal Accelerated Osteogenic OrthodonticsDocument6 pagesPeriodontal Accelerated Osteogenic Orthodonticsyui cherryNo ratings yet
- Feline Injection-Site Sarcoma - Todays Veterinary PracticeDocument12 pagesFeline Injection-Site Sarcoma - Todays Veterinary PracticeBla bla BlaNo ratings yet
- Persona Partial Knee Brochure PDFDocument12 pagesPersona Partial Knee Brochure PDF洪侊增No ratings yet
- Q - A Random 8Document5 pagesQ - A Random 8Yuuki Chitose (tai-kun)No ratings yet
- ZR53 MSDSDocument5 pagesZR53 MSDSAnonymous PinM7iNo ratings yet
- Short StoryDocument5 pagesShort Storyapi-376081909No ratings yet
- Winter Safety Toolbox TalkDocument18 pagesWinter Safety Toolbox TalkKristina100% (1)
- AntipyreticsDocument14 pagesAntipyreticsRadianty Haengbog Daeng FrederichaNo ratings yet
- EMP Procedure in MalaysiaDocument24 pagesEMP Procedure in Malaysialamkinpark3373No ratings yet
- Stacey Wilson-Web V-Sept 2014Document6 pagesStacey Wilson-Web V-Sept 2014api-247917310No ratings yet
- Postural DrainageDocument7 pagesPostural DrainagemohtishimNo ratings yet
- Tienchi Ginseng Panax Notoginseng San Qircljo PDFDocument4 pagesTienchi Ginseng Panax Notoginseng San Qircljo PDFTobiasenHolgersen89No ratings yet
- Unit 3Document15 pagesUnit 3Neenu RajputNo ratings yet
- Essential Nutrients - Minerals: 6.1 Introduction and ClassificationDocument15 pagesEssential Nutrients - Minerals: 6.1 Introduction and ClassificationRavinder RanaNo ratings yet
- Telescopic Handler Student ManualDocument41 pagesTelescopic Handler Student ManualingcalderonNo ratings yet
- SITHKOP005 - Written AssessmentDocument7 pagesSITHKOP005 - Written AssessmentTephieNo ratings yet
- BD Product ListDocument48 pagesBD Product Listanish_10677953100% (1)
- Alcohol Abuse Nicholas Black Professor Patton 7/6/2017Document9 pagesAlcohol Abuse Nicholas Black Professor Patton 7/6/2017iuibuibNo ratings yet
- The Legal Bases of Special EducationDocument14 pagesThe Legal Bases of Special EducationMaria Dulcinea Basbas86% (7)
- Surat Permintaan Obat Dinkes BaruDocument21 pagesSurat Permintaan Obat Dinkes BaruHafizh JhunkoNo ratings yet
- Hematoma: HaematomaDocument3 pagesHematoma: HaematomaBeeBeeSethNo ratings yet
- Test Bank For Mosbys Essentials For Nursing Assistants 4th Edition SorrentinoDocument24 pagesTest Bank For Mosbys Essentials For Nursing Assistants 4th Edition Sorrentinozacharymcleanpdqogjyfeb100% (47)
- WCLC2017 Abstract Book WebDocument700 pagesWCLC2017 Abstract Book Webdavid.yb.wangNo ratings yet
- 48069B - Ferrofos 5260 (GB-ENG)Document6 pages48069B - Ferrofos 5260 (GB-ENG)danielNo ratings yet
- Konsolidasi WelmiDocument72 pagesKonsolidasi WelmiWelmi Sulfatri IshakNo ratings yet
- BioassayDocument38 pagesBioassayMuhammad Masoom AkhtarNo ratings yet
- Internship PresentationDocument23 pagesInternship Presentationapi-556937362No ratings yet