You might also like
- Diagrams of Acupuncture ManipulationsDocument226 pagesDiagrams of Acupuncture Manipulationsgamisemas100% (13)
- Role and Scope of Practice For The Personal TrainerDocument34 pagesRole and Scope of Practice For The Personal Trainerislam100% (1)
- Naturopathy DietDocument6 pagesNaturopathy DietdevssplNo ratings yet
- Dr. Mercola - Take Control of Your HealthDocument368 pagesDr. Mercola - Take Control of Your HealthAnonymous 3YNFShC100% (3)
- Validating The Children's Medicines Use Questionnaire (CMUQ) in AustraliaDocument9 pagesValidating The Children's Medicines Use Questionnaire (CMUQ) in AustraliadidiNo ratings yet
- Nonpharmacologic Intervention On The Prevention of Pain and Anxiety During Pediatric Dental Care: A Systematic ReviewDocument11 pagesNonpharmacologic Intervention On The Prevention of Pain and Anxiety During Pediatric Dental Care: A Systematic ReviewJorge Luis Ramos MaqueraNo ratings yet
- JournalDocument10 pagesJournalYudirk MaulanaNo ratings yet
- Discharge Communication Practices in Pediatric Emergency Care - A Systematic Review and Narrative SynthesisDocument28 pagesDischarge Communication Practices in Pediatric Emergency Care - A Systematic Review and Narrative Synthesisleivaherre10No ratings yet
- Kuhn 16 01Document5 pagesKuhn 16 01anaelisarbbNo ratings yet
- Assessing The Construct Validity and Reliability of The Parental Perception On Antibiotics (PAPA) ScalesDocument9 pagesAssessing The Construct Validity and Reliability of The Parental Perception On Antibiotics (PAPA) ScalesAl ANo ratings yet
- Clinicians' Attitudes Toward Standardized Assessment and Diagnosis Within Child and Adolescent PsychiatryDocument13 pagesClinicians' Attitudes Toward Standardized Assessment and Diagnosis Within Child and Adolescent PsychiatryNidhöggr DNo ratings yet
- BMC Pediatrics: Supporting Children To Adhere To Anti-Retroviral Therapy in Urban Malawi: Multi Method InsightsDocument9 pagesBMC Pediatrics: Supporting Children To Adhere To Anti-Retroviral Therapy in Urban Malawi: Multi Method InsightsLouinel JosephNo ratings yet
- Evidence, Theory and Context - Using Intervention Mapping To Develop A School-Based Intervention To Prevent Obesity in ChildrenDocument15 pagesEvidence, Theory and Context - Using Intervention Mapping To Develop A School-Based Intervention To Prevent Obesity in ChildrenAlinaNo ratings yet
- Aids 35 463Document13 pagesAids 35 463apatassiNo ratings yet
- University of Salford Evaluation of The Action For Children Uk Neglect Project Final Report 2012Document47 pagesUniversity of Salford Evaluation of The Action For Children Uk Neglect Project Final Report 2012dariayvonneNo ratings yet
- Effectiveness of Structured Teaching Program On Knowledge Regarding Home Care Management of Children With Hydrocephalus and Shunt Among Their ParentsDocument3 pagesEffectiveness of Structured Teaching Program On Knowledge Regarding Home Care Management of Children With Hydrocephalus and Shunt Among Their ParentsIrnayanti MamiDgSiameNo ratings yet
- 2017 - Alomari Et AlDocument18 pages2017 - Alomari Et AlazeemathmariyamNo ratings yet
- Selecting Developmental Surveillance and Screening ToolsDocument7 pagesSelecting Developmental Surveillance and Screening ToolsGerald Howard UntarioNo ratings yet
- Obat Off-LabelDocument7 pagesObat Off-LabelYulia AfrianiNo ratings yet
- Health Promotion Interventions To Improve Oral Health of Adolescents: A Systematic Review and Meta-AnalysisDocument12 pagesHealth Promotion Interventions To Improve Oral Health of Adolescents: A Systematic Review and Meta-AnalysisSarbu AndraNo ratings yet
- When Parents Won't Vaccinate Their Children: A Qualitative Investigation of Australian Primary Care Providers' ExperiencesDocument20 pagesWhen Parents Won't Vaccinate Their Children: A Qualitative Investigation of Australian Primary Care Providers' ExperiencesTimmy LarasatiNo ratings yet
- Allen 12 02Document4 pagesAllen 12 02Sarah_Zeitoun_792No ratings yet
- ArticuloDocument13 pagesArticuloCralosNo ratings yet
- Research ArticleDocument8 pagesResearch ArticleDennis MejiaNo ratings yet
- Summ 1619Document8 pagesSumm 1619novialbarNo ratings yet
- Parent's Views On Factors in Uencing The Dental Health of Trinidadian Preschool ChildrenDocument10 pagesParent's Views On Factors in Uencing The Dental Health of Trinidadian Preschool ChildrenElisabeth FransiskaNo ratings yet
- Prevención Primaria de La Obesidad Infantil A Través de Sesiones de Asesoramiento en Centros de SaludDocument13 pagesPrevención Primaria de La Obesidad Infantil A Través de Sesiones de Asesoramiento en Centros de SaludRoberto MartellNo ratings yet
- 2019 Article 305 PDFDocument3 pages2019 Article 305 PDFDipyanalarNo ratings yet
- Research Revised March 22 2024Document39 pagesResearch Revised March 22 2024amandigNo ratings yet
- 2015 Article 516Document12 pages2015 Article 516Mukhtar TarNo ratings yet
- Preprints202011 0468 v1Document32 pagesPreprints202011 0468 v1Cipariu AdinaNo ratings yet
- Develop Med Child Neuro - 2021 - Ogourtsova - Patient Engagement in An Online Coaching Intervention For Parents of ChildrenDocument8 pagesDevelop Med Child Neuro - 2021 - Ogourtsova - Patient Engagement in An Online Coaching Intervention For Parents of ChildrenpsicoterapiavaldiviaNo ratings yet
- J Jfludis 2021 105843Document21 pagesJ Jfludis 2021 105843ANDREA MIRANDA MEZA GARNICANo ratings yet
- Developing Delirium Best Practice: A Systematic Review of Education Interventions For Healthcare Professionals Working in Inpatient SettingsDocument32 pagesDeveloping Delirium Best Practice: A Systematic Review of Education Interventions For Healthcare Professionals Working in Inpatient Settingslinxiaofei2019No ratings yet
- Cognitive Behaviour Therapy For Anxious Paediatric Dental Patients: A Systematic ReviewDocument10 pagesCognitive Behaviour Therapy For Anxious Paediatric Dental Patients: A Systematic ReviewSung Soon ChangNo ratings yet
- Out 17Document10 pagesOut 17laodesyuhadarNo ratings yet
- Nutrients 07 05414 v3Document12 pagesNutrients 07 05414 v3BernaluttaaaNo ratings yet
- Factors Affecting Children's Adherence To Regular Dental AttendanceDocument12 pagesFactors Affecting Children's Adherence To Regular Dental AttendanceDuanne EdvirgeNo ratings yet
- Palliative CareDocument11 pagesPalliative CareCiocan AlexandraNo ratings yet
- An Overview of Systematic Reviews of ComplementaryDocument16 pagesAn Overview of Systematic Reviews of ComplementaryDanilo VasconcelosNo ratings yet
- Complementary Therapies in Clinical PracticeDocument7 pagesComplementary Therapies in Clinical Practiceapi-615757498No ratings yet
- Artikel PDP MTBSDocument9 pagesArtikel PDP MTBSRed 777No ratings yet
- Ijerph 16 03996Document11 pagesIjerph 16 03996Cristine ChubiboNo ratings yet
- LM RelDocument15 pagesLM RelingridspulerNo ratings yet
- Review 2008 enDocument6 pagesReview 2008 envimlenNo ratings yet
- Eating Disorder Among AdolescentsDocument12 pagesEating Disorder Among AdolescentsnurNo ratings yet
- UntitledDocument10 pagesUntitledWahidNo ratings yet
- 2016 Article 497Document11 pages2016 Article 497poeou sanNo ratings yet
- Non-pharmacological behaviour management - 副本Document37 pagesNon-pharmacological behaviour management - 副本刘雨樵No ratings yet
- Risk Factors For Early Childhood Caries: A Systematic Review and Meta-Analysis of Case Control and Cohort StudiesDocument18 pagesRisk Factors For Early Childhood Caries: A Systematic Review and Meta-Analysis of Case Control and Cohort StudiesNatalia DavilaNo ratings yet
- Use of Decision Support Tools To Empower Pregnant Women: Systematic ReviewDocument10 pagesUse of Decision Support Tools To Empower Pregnant Women: Systematic ReviewINA SAKTINo ratings yet
- A Case Study of Adolescent Substance MisuseDocument9 pagesA Case Study of Adolescent Substance MisuseRichelleNo ratings yet
- Jurnal Ikm 3Document10 pagesJurnal Ikm 3Rahmayuni FItriantiNo ratings yet
- Children 01 00424Document17 pagesChildren 01 00424netoginetaNo ratings yet
- Social Science & Medicine: Stephanie R. Smith, Jeroen Kroon, Ralf Schwarzer, Kyra HamiltonDocument12 pagesSocial Science & Medicine: Stephanie R. Smith, Jeroen Kroon, Ralf Schwarzer, Kyra Hamiltonjuan felipe castellanos arangoNo ratings yet
- Jcs 8 105Document6 pagesJcs 8 105nadia syestiNo ratings yet
- Families, Nurses and Organisations Contributing Factors To Medication Administration Error in Paediatrics: A Literature ReviewDocument15 pagesFamilies, Nurses and Organisations Contributing Factors To Medication Administration Error in Paediatrics: A Literature ReviewsabitaNo ratings yet
- PutriAnjeli Gizi2B JurnalthypoidDocument10 pagesPutriAnjeli Gizi2B JurnalthypoidPutri AnjeliNo ratings yet
- Prevention and Health Promotion 2023SSDocument39 pagesPrevention and Health Promotion 2023SSzeynepNo ratings yet
- 10 1111@cdoe 12578Document11 pages10 1111@cdoe 12578andres.ft12345No ratings yet
- Maternal Knowledge, Attitudes and Practices Towards Prevention and Management of Child Diarrhoea in Urban and Rural Maseru, LesothoDocument20 pagesMaternal Knowledge, Attitudes and Practices Towards Prevention and Management of Child Diarrhoea in Urban and Rural Maseru, LesothoAnisa SafutriNo ratings yet
- The Healthy Teen Project: Tools To Enhance Adolescent Health CounselingDocument4 pagesThe Healthy Teen Project: Tools To Enhance Adolescent Health CounselingFabio HimanNo ratings yet
- Homeopathic Preparations For Preventing and Treating Acute Upper Respiratory Tract Infections in Children: A Systematic Review and Meta-AnalysisDocument10 pagesHomeopathic Preparations For Preventing and Treating Acute Upper Respiratory Tract Infections in Children: A Systematic Review and Meta-AnalysisCarlos Arturo Vera VásquezNo ratings yet
- Relationship Between Health Literacy Scores and Patient Use of the iPET for Patient EducationFrom EverandRelationship Between Health Literacy Scores and Patient Use of the iPET for Patient EducationNo ratings yet
- The Effects of Eye Masks and Earplugs On The Sleep Quality and Anxiety of Hospitalized Patientsa Randomised Controlled TDocument9 pagesThe Effects of Eye Masks and Earplugs On The Sleep Quality and Anxiety of Hospitalized Patientsa Randomised Controlled TjayaNo ratings yet
- Kumpul PDF Kisah Untuk Geri by Erisca FebrianiDocument389 pagesKumpul PDF Kisah Untuk Geri by Erisca FebrianijayaNo ratings yet
- Acupuncture With Manual and Electrical Stimulation For Labour Pain: A Two Month Follow Up of Recollection of Pain and Birth ExperienceDocument9 pagesAcupuncture With Manual and Electrical Stimulation For Labour Pain: A Two Month Follow Up of Recollection of Pain and Birth ExperiencejayaNo ratings yet
- Jurnal Post PartumDocument11 pagesJurnal Post PartumjayaNo ratings yet
- Effect of Garlic and Aged Black Garlic On Hyperglycemia and Dyslipidemia in Animal Model of Type 2 Diabetes MellitusDocument7 pagesEffect of Garlic and Aged Black Garlic On Hyperglycemia and Dyslipidemia in Animal Model of Type 2 Diabetes MellitusjayaNo ratings yet
- Onsumer Ealth Ssues: One Part One Chapter OneDocument12 pagesOnsumer Ealth Ssues: One Part One Chapter OneIsaiah Gib BagaNo ratings yet
- Complementary and Alternative Medicine 2017Document87 pagesComplementary and Alternative Medicine 2017Hannah Jean Lapenid LemorenasNo ratings yet
- Kavya.r 15ar034 Topic SelectionDocument23 pagesKavya.r 15ar034 Topic SelectionJoseph KuruvilaNo ratings yet
- 2363 Materia Medica by KentDocument7 pages2363 Materia Medica by Kentgceramesh100% (1)
- Copia de Body CodeDocument305 pagesCopia de Body CodeMaynor DavidNo ratings yet
- Ruscus Aculeatus. Homeopathic Remedy - Remedia HomeopathyDocument5 pagesRuscus Aculeatus. Homeopathic Remedy - Remedia HomeopathyNawaz SfNo ratings yet
- Anderson R WtmsDocument224 pagesAnderson R WtmsSudhaNo ratings yet
- 1st BHMS Supplementary Result PDFDocument91 pages1st BHMS Supplementary Result PDFSushil RajbharNo ratings yet
- The Rational Basis of "Nature Cure" PDFDocument4 pagesThe Rational Basis of "Nature Cure" PDFkrishna2205No ratings yet
- Nature Cure Ashram Fact SheetDocument4 pagesNature Cure Ashram Fact SheetnisargopcharNo ratings yet
- Tratamiento Natural CancerDocument65 pagesTratamiento Natural CancerSaladeensayo Arriendo Ampli CorpsearicaNo ratings yet
- 14A REASON WE USE RGCC Cancer Test 2.13.14Document14 pages14A REASON WE USE RGCC Cancer Test 2.13.14Lee Ming HinNo ratings yet
- 1-S2.0-S2213398421001081-Main Science DirectDocument4 pages1-S2.0-S2213398421001081-Main Science Directaris dwiprasetyaNo ratings yet
- CME-Nathuropathy Day 2023Document2 pagesCME-Nathuropathy Day 2023dudekula salmaNo ratings yet
- Homoeopathy Whats The Harm in ItDocument34 pagesHomoeopathy Whats The Harm in ItFrancis Lobo100% (1)
- B1 1 HowIBeatEmphysemaandCOPDinSixWeeks PDFDocument130 pagesB1 1 HowIBeatEmphysemaandCOPDinSixWeeks PDFGreg DaymondNo ratings yet
- The Villager-E'ville: June 4-10, 2009Document12 pagesThe Villager-E'ville: June 4-10, 2009The Villager100% (2)
- Encyclopaedia of Homoeopathic Pharmacopoeia Edition 2002 P N Varma Indu Vaid.01807 - 1Document6 pagesEncyclopaedia of Homoeopathic Pharmacopoeia Edition 2002 P N Varma Indu Vaid.01807 - 1Sohail LatifNo ratings yet
- Alternative Medicine Prroposal2Document20 pagesAlternative Medicine Prroposal2Amina AbubakarNo ratings yet
- Naturopathic Medicine: By: Beverlyn C. Bagolos and Marianne MacanlayDocument19 pagesNaturopathic Medicine: By: Beverlyn C. Bagolos and Marianne Macanlaynicole cenaNo ratings yet
- NaturopathyDocument2 pagesNaturopathyregunathanNo ratings yet
- Workbook Exercises - Reiki Master CourseDocument28 pagesWorkbook Exercises - Reiki Master CourseValentina Angelini67% (3)
- NUHS Alumnus Vol. 50, Issue No. 2Document4 pagesNUHS Alumnus Vol. 50, Issue No. 2National University of Health SciencesNo ratings yet
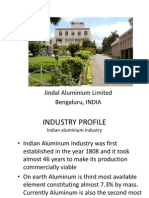
- Organization Study ReportDocument25 pagesOrganization Study Reporttharunarunnaik100% (1)
- NutritionalProducts082305 000Document12 pagesNutritionalProducts082305 000api-3757907No ratings yet
- State Complaint Against Dr. Bodo SchneiderDocument6 pagesState Complaint Against Dr. Bodo SchneiderDean OlsenNo ratings yet