You might also like
- A Study On Knowledge and Practice of Mothers of Under-Five ChildrenDocument6 pagesA Study On Knowledge and Practice of Mothers of Under-Five ChildrenRirin PurbaNo ratings yet
- RESEARCH-REVISED-MARCH-22-2024 (1)Document39 pagesRESEARCH-REVISED-MARCH-22-2024 (1)amandigNo ratings yet
- Knowledge, Attitude and Practice of MothersCaregivers Regarding Oral Rehydration Therapy at Ishaka Adventist Hospital Bushenyi District UgandaDocument12 pagesKnowledge, Attitude and Practice of MothersCaregivers Regarding Oral Rehydration Therapy at Ishaka Adventist Hospital Bushenyi District UgandaKIU PUBLICATION AND EXTENSIONNo ratings yet
- Mothers' Perception and Management Preference of Acute Diarrheal DiseaseDocument9 pagesMothers' Perception and Management Preference of Acute Diarrheal DiseaseIJPHSNo ratings yet
- Research ArticleDocument13 pagesResearch ArticleDENNYNo ratings yet
- Determinants of Mother's Preventive Practices Against Children's Acute Gastroenteritis: Basis For A Health Education ProgramDocument10 pagesDeterminants of Mother's Preventive Practices Against Children's Acute Gastroenteritis: Basis For A Health Education Programderma yahya wiharyoNo ratings yet
- Tina Joseph, Prakash Naregal: ISSN (Online) : 2319-7064 Impact Factor (2012) : 3.358Document6 pagesTina Joseph, Prakash Naregal: ISSN (Online) : 2319-7064 Impact Factor (2012) : 3.358asepNo ratings yet
- 1 s2.0 S2213398422000392 MainDocument9 pages1 s2.0 S2213398422000392 MainMoad RuzkiNo ratings yet
- Acute Malnutrition PDFDocument10 pagesAcute Malnutrition PDFDamesa MiesaNo ratings yet
- Article SssssssssssssssssssDocument7 pagesArticle SssssssssssssssssssBULAN IFTINAZHIFANo ratings yet
- Nursing Intervention in Children With Diarrhea: A Case StudyDocument6 pagesNursing Intervention in Children With Diarrhea: A Case StudyshekinahhuzsumangilNo ratings yet
- Rural-Urban Comparison On Mothers' Media Access and Information Needs On Dengue Prevention and ControlDocument83 pagesRural-Urban Comparison On Mothers' Media Access and Information Needs On Dengue Prevention and ControlBuen Josef Cainila AndradeNo ratings yet
- Jurnal KesehatanDocument10 pagesJurnal KesehatanFiqriNo ratings yet
- Dea 1Document11 pagesDea 1Dea Hadfina Kartika SariNo ratings yet
- Mothers KnowledgeDocument10 pagesMothers KnowledgeSaad aliraqiNo ratings yet
- Maternal Child Nutrition - 2021 - Thurstans - The Relationship Between Wasting and Stunting in Young Children ADocument25 pagesMaternal Child Nutrition - 2021 - Thurstans - The Relationship Between Wasting and Stunting in Young Children AUlin NikmatusNo ratings yet
- Causal Relationship Between Environmental Enteric Dysfunction - 2022 - ScientifDocument8 pagesCausal Relationship Between Environmental Enteric Dysfunction - 2022 - ScientifCawee CawNo ratings yet
- Volume 1. No.1 Tahun 2019, e-ISSNDocument7 pagesVolume 1. No.1 Tahun 2019, e-ISSNravenNo ratings yet
- Factors Contributing To Malnutrition Among HIV Positive Children Aged Between 6 and 60 MonthsDocument10 pagesFactors Contributing To Malnutrition Among HIV Positive Children Aged Between 6 and 60 MonthsInternational Organization of Scientific Research (IOSR)No ratings yet
- Indonesia Maternal Health Articles - Abstracts - NeonatalDocument92 pagesIndonesia Maternal Health Articles - Abstracts - Neonatalnova seftya aristadilaNo ratings yet
- Prevalence and Factors Associated With Intestinal Parasites Among Children of Age 6 To 59 Months In, Boricha District, South Ethiopia, in 2018Document7 pagesPrevalence and Factors Associated With Intestinal Parasites Among Children of Age 6 To 59 Months In, Boricha District, South Ethiopia, in 2018Mirtha AnggraeniNo ratings yet
- International Journal of Trend in Scientific Research and Development (IJTSRD)Document8 pagesInternational Journal of Trend in Scientific Research and Development (IJTSRD)Editor IJTSRDNo ratings yet
- Researh ProblemsDocument7 pagesResearh ProblemsPrincess Arah AquinoNo ratings yet
- ROL FinalDocument28 pagesROL FinalSiyona BansodeNo ratings yet
- Alalag, Elsie: "The Impact of Access To Immunization Information On Vaccine Acceptance in Three Countries"Document4 pagesAlalag, Elsie: "The Impact of Access To Immunization Information On Vaccine Acceptance in Three Countries"Basema HashhashNo ratings yet
- Exploring Women Knowledge of Newborn Danger Signs: A Case of Mothers With Under Five ChildrenDocument8 pagesExploring Women Knowledge of Newborn Danger Signs: A Case of Mothers With Under Five ChildrenJohnjohn MateoNo ratings yet
- Research Article Food and Personal Hygiene Perceptions and Practices Among Caregivers Whose Children Have Diarrhea: A Qualitative Study of Urban Mothers in Tangerang, IndonesiaDocument8 pagesResearch Article Food and Personal Hygiene Perceptions and Practices Among Caregivers Whose Children Have Diarrhea: A Qualitative Study of Urban Mothers in Tangerang, IndonesiaAndi UmmahNo ratings yet
- Knowledge, Attitude and Practice of Mothers With Children Less Than Five Years Toward Vaccination in Khartoum State-Ummbada Locality-Allbugaa-2017Document4 pagesKnowledge, Attitude and Practice of Mothers With Children Less Than Five Years Toward Vaccination in Khartoum State-Ummbada Locality-Allbugaa-2017krishnasree100% (1)
- Research ArticleDocument12 pagesResearch ArticleFanky RamadhanNo ratings yet
- Dietary Diversity Practice and Associated Factors Among Infants and Young Children in Haramaya Town, EthiopiaDocument8 pagesDietary Diversity Practice and Associated Factors Among Infants and Young Children in Haramaya Town, EthiopiaIJPHSNo ratings yet
- Predicting Relationship Between Food-Borne Disease Information-Adequacy and Food Handling Practices Among Food-Handlers in Selected Restaurants in Ggaba Kampala, Makindye Division UgandaDocument8 pagesPredicting Relationship Between Food-Borne Disease Information-Adequacy and Food Handling Practices Among Food-Handlers in Selected Restaurants in Ggaba Kampala, Makindye Division UgandaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Correlation of Nutritional Anemia and Blood Group Prevalence Among Adolescent Girls in Pudukkottai District of IndiaDocument4 pagesCorrelation of Nutritional Anemia and Blood Group Prevalence Among Adolescent Girls in Pudukkottai District of IndiaOmWawanNo ratings yet
- JMDH 15 1069Document14 pagesJMDH 15 1069AKIM WONGNo ratings yet
- Extent of Compliance and Perception of Mothers On Childhood Immunization in Barangay Ugac Sur, Tuguegarao City, Philippines: A Descriptive StudyDocument6 pagesExtent of Compliance and Perception of Mothers On Childhood Immunization in Barangay Ugac Sur, Tuguegarao City, Philippines: A Descriptive StudyMamta AgarwalNo ratings yet
- Associations Between Soft-Drink ConsumptionDocument9 pagesAssociations Between Soft-Drink ConsumptionkarinaNo ratings yet
- Knowledge Attitude and Practice Towards MalnutritierDocument6 pagesKnowledge Attitude and Practice Towards MalnutritierEmiru MerdassaNo ratings yet
- Medalion DOORTUA+2021 Bhs+InggDocument5 pagesMedalion DOORTUA+2021 Bhs+InggCindy SulistyowatiNo ratings yet
- Factors That Contribute To Occurrence of Malnutrition Among Children Below Five Years in Pediatric Ward Itojo Hospital, Ntungamo District Uganda.Document14 pagesFactors That Contribute To Occurrence of Malnutrition Among Children Below Five Years in Pediatric Ward Itojo Hospital, Ntungamo District Uganda.KIU PUBLICATION AND EXTENSIONNo ratings yet
- How Is The Effect of Health Services On Toddler Diarrhea?: Ecological Analysis in IndonesiaDocument11 pagesHow Is The Effect of Health Services On Toddler Diarrhea?: Ecological Analysis in IndonesiaomniyaNo ratings yet
- Abera2017 Prevalence of Malnutrition and Associated Factors in EthiopiaDocument8 pagesAbera2017 Prevalence of Malnutrition and Associated Factors in EthiopiaSHILPA PATILNo ratings yet
- Health CommunicationDocument17 pagesHealth CommunicationshuvoNo ratings yet
- Chapters 1 To 2. Incomplete. Please Double CheckDocument19 pagesChapters 1 To 2. Incomplete. Please Double CheckajdgafjsdgaNo ratings yet
- 08kharirohijphsjun16 Edit-With-Cover-Page-V2Document7 pages08kharirohijphsjun16 Edit-With-Cover-Page-V2Godeliva AdrianiNo ratings yet
- Effect of Health Teaching On Knowledge and Practice of Postnatal Mother Admitted in Selected Hospital Regarding Using Diaper in Children To Prevent Systemic Bacterial InfectionDocument7 pagesEffect of Health Teaching On Knowledge and Practice of Postnatal Mother Admitted in Selected Hospital Regarding Using Diaper in Children To Prevent Systemic Bacterial InfectionLovely SarangiNo ratings yet
- Assessment of Hand Washing Practice andDocument6 pagesAssessment of Hand Washing Practice andAbdirahman Yusuf AliNo ratings yet
- Knowledge, Attitude and Practices of Typhoid FeverDocument5 pagesKnowledge, Attitude and Practices of Typhoid FeverEddna SeharNo ratings yet
- Zubiaga, R-Jeane S. - BSN 3 - For PlagscanDocument41 pagesZubiaga, R-Jeane S. - BSN 3 - For PlagscanR-Jeane ZubiagaNo ratings yet
- Prevalence of Malnutrition Among Hospitalized Children: June 2014Document4 pagesPrevalence of Malnutrition Among Hospitalized Children: June 2014Imin BuntaraNo ratings yet
- Anwar 2192023 AJMAH100084Document8 pagesAnwar 2192023 AJMAH100084anggitasabila99No ratings yet
- 2020 Knowledge and Practice of Child Survival StrategiesDocument8 pages2020 Knowledge and Practice of Child Survival StrategiesResearch ArenaNo ratings yet
- Journal MesinaDocument4 pagesJournal MesinaKrizelle MesinaNo ratings yet
- Effects of Health Education On Leptospirosis Prevention Through DasawismaDocument6 pagesEffects of Health Education On Leptospirosis Prevention Through DasawismaJurnal Ners UNAIRNo ratings yet
- Article Print 4609Document9 pagesArticle Print 4609EMIRZA NUR WICAKSONONo ratings yet
- Upaya Penurunan Kasus Diare Dengan Meningkatkan Keterlibatan Ibu Dalam Gerakan PHBSDocument8 pagesUpaya Penurunan Kasus Diare Dengan Meningkatkan Keterlibatan Ibu Dalam Gerakan PHBSNidia Achirul tamaraNo ratings yet
- Water, Sanitation, and Hygiene: Linkages With Stunting in Rural EthiopiaDocument21 pagesWater, Sanitation, and Hygiene: Linkages With Stunting in Rural EthiopiaFariz HidayatNo ratings yet
- The Effect of Health Education On Gastritis Prevention Behavior Among High SchoolDocument4 pagesThe Effect of Health Education On Gastritis Prevention Behavior Among High SchoolLina RosianiNo ratings yet
- Appr MS Id 000563Document7 pagesAppr MS Id 000563LAWSON IYENE-EMINo ratings yet
- Nyarkoetal 2023Document16 pagesNyarkoetal 2023hafsatsaniibrahimmlfNo ratings yet
- Alcohol, Betel-Nut and Cigarette Consumption Are Negatively Associated With Health Promoting Behaviors in Taiwan: A Cross-Sectional StudyDocument8 pagesAlcohol, Betel-Nut and Cigarette Consumption Are Negatively Associated With Health Promoting Behaviors in Taiwan: A Cross-Sectional StudyJuita Auglina PasaribuNo ratings yet
- Pengaruh Range of Motion (ROM) Aktif Terhadap Fleksibilitas Sendi Lutut Pada Lanjut UsiaDocument4 pagesPengaruh Range of Motion (ROM) Aktif Terhadap Fleksibilitas Sendi Lutut Pada Lanjut UsiaAnisa SafutriNo ratings yet
- The Covid-19 Pandemic and The Incidence of Acute Myocardial InfarctionDocument3 pagesThe Covid-19 Pandemic and The Incidence of Acute Myocardial InfarctionAnisa SafutriNo ratings yet
- The COVID-19 Pandemic in The US A Clinical UpdateDocument2 pagesThe COVID-19 Pandemic in The US A Clinical UpdatexlhoakylxNo ratings yet
- MainDocument4 pagesMainAnisa SafutriNo ratings yet
- Daniel2020 Article EducationAndTheCOVID-19PandemiDocument6 pagesDaniel2020 Article EducationAndTheCOVID-19PandemihandokoNo ratings yet
- Jurnal FEMA, Volume 2, Nomor 1, Januari 2014: Bambang Sulaksana, Yanuar Burhanuddin Dan Ageng Sadnowo. RDocument7 pagesJurnal FEMA, Volume 2, Nomor 1, Januari 2014: Bambang Sulaksana, Yanuar Burhanuddin Dan Ageng Sadnowo. RAnisa SafutriNo ratings yet
- Jurnal 4Document5 pagesJurnal 4DwiKamaswariNo ratings yet
- Pengaruh Range of Motion (ROM) Aktif Terhadap Fleksibilitas Sendi Lutut Pada Lanjut UsiaDocument4 pagesPengaruh Range of Motion (ROM) Aktif Terhadap Fleksibilitas Sendi Lutut Pada Lanjut UsiaAnisa SafutriNo ratings yet
- 287 1095 3 PB PDFDocument9 pages287 1095 3 PB PDFAriefchsNo ratings yet
- Association of Recanalization of The Left UmbilicaDocument2 pagesAssociation of Recanalization of The Left UmbilicaAnisa SafutriNo ratings yet
- Jurnal FEMA, Volume 2, Nomor 1, Januari 2014: Yudhistyra Saputra, Muhammad Badaruddin Dan ZulhanifDocument7 pagesJurnal FEMA, Volume 2, Nomor 1, Januari 2014: Yudhistyra Saputra, Muhammad Badaruddin Dan ZulhanifAnisa SafutriNo ratings yet
- Jurnal FEMA, Volume 2, Nomor 2, April 2014: Andareas Wijaya Sitepu Jorfri B. Sinaga Dan Agus SugiriDocument7 pagesJurnal FEMA, Volume 2, Nomor 2, April 2014: Andareas Wijaya Sitepu Jorfri B. Sinaga Dan Agus SugiriAnisa SafutriNo ratings yet
- The Activities of Scirpophaga Incertulas Adult From Klaten RegencyDocument8 pagesThe Activities of Scirpophaga Incertulas Adult From Klaten RegencyAnisa SafutriNo ratings yet
- Break Even Point Analysis of LED Lamp Usage for LightingDocument8 pagesBreak Even Point Analysis of LED Lamp Usage for LightingAnisa SafutriNo ratings yet
- United States Patent: Swayze Et Al. Jun. 14, 2005Document32 pagesUnited States Patent: Swayze Et Al. Jun. 14, 2005Anisa SafutriNo ratings yet
- Perancangan Dan Realisasi Sistem Kendali Lampu, Air Conditionerer Berbasis AndroidDocument8 pagesPerancangan Dan Realisasi Sistem Kendali Lampu, Air Conditionerer Berbasis AndroidAnisa SafutriNo ratings yet
- Genetic of Indirect: Study Inguinal HerniaDocument6 pagesGenetic of Indirect: Study Inguinal HerniaAnisa SafutriNo ratings yet
- Diagnosis and Classification of Disorders Specifically Associated With Stress: Proposals For ICD-11Document9 pagesDiagnosis and Classification of Disorders Specifically Associated With Stress: Proposals For ICD-11Anisa SafutriNo ratings yet
- Familial Hiatal Hernia in A Large Five Generation Family Confirming True Autosomal Dominant InheritanceDocument4 pagesFamilial Hiatal Hernia in A Large Five Generation Family Confirming True Autosomal Dominant InheritanceAnisa SafutriNo ratings yet
- Proceedings ICoMP Vol1Document377 pagesProceedings ICoMP Vol1Anisa SafutriNo ratings yet
- Lesions Portal Gastritis Congestive Gastropathy?: Gastric in Hypertension: InflammatoryDocument7 pagesLesions Portal Gastritis Congestive Gastropathy?: Gastric in Hypertension: InflammatoryAnisa SafutriNo ratings yet
- Diagnosis Gastritis Fibreoptic Biopsy Specimens: The Histological inDocument11 pagesDiagnosis Gastritis Fibreoptic Biopsy Specimens: The Histological inAnisa SafutriNo ratings yet
- Hubungan Tingkat Depresi Dan Kualitas Hidup Pada Pasien Gagal Jantung Kronik Di Poliklinik Jantung RSUP Prof. Dr. R. D. Kandou ManadoDocument7 pagesHubungan Tingkat Depresi Dan Kualitas Hidup Pada Pasien Gagal Jantung Kronik Di Poliklinik Jantung RSUP Prof. Dr. R. D. Kandou ManadoayuwulandariNo ratings yet
- Auguste D and Alzheimer's Disease: Department of Medical HistoryDocument4 pagesAuguste D and Alzheimer's Disease: Department of Medical HistorySatyavrat WagleNo ratings yet
- Hubungan Antara Jarak Tempuh Tes Jalan 6 Menit Dan Fraksi Ejeksi Pada Pasien Gagal Jantung Kronik Terhadap Kejadian KardiovaskularDocument8 pagesHubungan Antara Jarak Tempuh Tes Jalan 6 Menit Dan Fraksi Ejeksi Pada Pasien Gagal Jantung Kronik Terhadap Kejadian KardiovaskularselvianaNo ratings yet
- Global Youth Tobacco Surveillance, 2000-2007: Morbidity and Mortality Weekly ReportDocument32 pagesGlobal Youth Tobacco Surveillance, 2000-2007: Morbidity and Mortality Weekly ReportAnisa SafutriNo ratings yet
- NYHA class and ejection fraction relationship in chronic heart failureDocument8 pagesNYHA class and ejection fraction relationship in chronic heart failureflying highNo ratings yet
- Epithelial Barrier Function by Proinflammatory Cytokines DisruptDocument10 pagesEpithelial Barrier Function by Proinflammatory Cytokines DisruptAnisa SafutriNo ratings yet
- Effect of An Intensive Exercise Intervention Strategy On Modifiable Cardiovascular Risk Factors in Subjects With Type 2 Diabetes MellitusDocument10 pagesEffect of An Intensive Exercise Intervention Strategy On Modifiable Cardiovascular Risk Factors in Subjects With Type 2 Diabetes MellitusAnisa SafutriNo ratings yet
- Cancer Disparities by Race/Ethnicity and Socioeconomic StatusDocument16 pagesCancer Disparities by Race/Ethnicity and Socioeconomic StatusAnisa SafutriNo ratings yet
- Catálogo de Dispositivos PQS 2014 PDFDocument318 pagesCatálogo de Dispositivos PQS 2014 PDFGestion Biomedica Prosalco IPSNo ratings yet
- Biomechanics of Edentulous StateDocument15 pagesBiomechanics of Edentulous StateNadeemNo ratings yet
- Medical Microbiology Examination (140 Questions) : First Aid For The Basic Sciences General PrinciplesDocument58 pagesMedical Microbiology Examination (140 Questions) : First Aid For The Basic Sciences General Principlesyashwanth88100% (1)
- Addressing Barriers, Stigma and Discrimination Surrounding HIV and Viral HepatitisDocument17 pagesAddressing Barriers, Stigma and Discrimination Surrounding HIV and Viral HepatitisAlemayehu KebedeNo ratings yet
- Child Health COURSE PLAN M.SC 2 YEARDocument49 pagesChild Health COURSE PLAN M.SC 2 YEARSanthosh.S.UNo ratings yet
- Baby Thesis RevisedDocument20 pagesBaby Thesis RevisedSanjoe Angelo ManaloNo ratings yet
- Khatib2017 PDFDocument14 pagesKhatib2017 PDFluxmansrikanthaNo ratings yet
- Nilufa Shariff - Pain Dissertation PresentationDocument31 pagesNilufa Shariff - Pain Dissertation PresentationNilufar JivrajNo ratings yet
- Nursing Care Plan For GlaucomaDocument3 pagesNursing Care Plan For Glaucomaderic79% (28)
- Provisional Admit Card Cum Call LetterDocument3 pagesProvisional Admit Card Cum Call Lettersravikumar sNo ratings yet
- M.Sc Psychology Syllabus Provides Comprehensive CoverageDocument55 pagesM.Sc Psychology Syllabus Provides Comprehensive CoverageRashmi NNo ratings yet
- Limited Uretheral Mobilization Procedure (Lump) For Distal Penile Hypospadias Repair, A Single Centre Retrospective AnalysisDocument9 pagesLimited Uretheral Mobilization Procedure (Lump) For Distal Penile Hypospadias Repair, A Single Centre Retrospective AnalysisIJAR JOURNALNo ratings yet
- The Psychodynamic Diagnostic Manual An Effort To Compensate For The Limitations of Descriptive Psychiatric Diagnosis (Mcwilliams2011)Document12 pagesThe Psychodynamic Diagnostic Manual An Effort To Compensate For The Limitations of Descriptive Psychiatric Diagnosis (Mcwilliams2011)Anastasiya PlohihNo ratings yet
- BOSH For SO1 Student Manual SampleDocument65 pagesBOSH For SO1 Student Manual SampleFroilan olazo100% (1)
- The Theorists' Holistic Nursing TheoryDocument2 pagesThe Theorists' Holistic Nursing TheoryMary Elijah Jane PopesNo ratings yet
- Heavenly Spa MenuDocument2 pagesHeavenly Spa MenuDeTaaliNo ratings yet
- Audit of Delivery of Treatment Services For Children With AutismDocument72 pagesAudit of Delivery of Treatment Services For Children With AutismMichelle RindelsNo ratings yet
- Misconceptions About The Use of Genetic Tests in PopulationsDocument4 pagesMisconceptions About The Use of Genetic Tests in PopulationsAneeshNo ratings yet
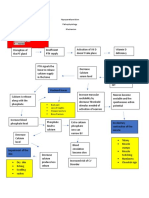
- Hypoparathyroidism PathophysiologyDocument1 pageHypoparathyroidism PathophysiologymaricarNo ratings yet
- Ovate PDFDocument11 pagesOvate PDFAriPratiwiNo ratings yet
- NCP Activity NavidasDocument2 pagesNCP Activity NavidasFran LanNo ratings yet
- Suicide Prevention and Intervention: HelplinesDocument1 pageSuicide Prevention and Intervention: Helplinesdesignbox91No ratings yet
- Viastar Blue Oral Dissolving Film 50 MG - Sildenafil Sitrat - DKI1953300196A1 - 2019Document17 pagesViastar Blue Oral Dissolving Film 50 MG - Sildenafil Sitrat - DKI1953300196A1 - 2019RIRINo ratings yet
- Nuclear Medicine Therapy: Side Effects and Complications Luca GiovanellaDocument124 pagesNuclear Medicine Therapy: Side Effects and Complications Luca GiovanellaWhite HeartNo ratings yet
- Module 2 - 1. Research Overview TranscriptDocument13 pagesModule 2 - 1. Research Overview TranscriptpatrickfvlboltNo ratings yet
- Cardiovascular SystemDocument26 pagesCardiovascular SystemRismawatiNo ratings yet
- Arthritis OsteoarthritisDocument43 pagesArthritis OsteoarthritisMYMANo ratings yet
- Transcultural Nursing Across The Life Span: Ma. Flossie L. TangpuzDocument23 pagesTranscultural Nursing Across The Life Span: Ma. Flossie L. TangpuzSheila VerbaNo ratings yet
- Sia DH FinalDocument26 pagesSia DH FinalJennifer DixonNo ratings yet
- Og - Applying To The Ndis v5.0 Approved - External 2023-09-28Document55 pagesOg - Applying To The Ndis v5.0 Approved - External 2023-09-28faithgaye432No ratings yet