You might also like
- Current Systems of Health CareDocument4 pagesCurrent Systems of Health Carekangna_sharma20No ratings yet
- Meeting the Needs of Older Adults with Serious Illness: Challenges and Opportunities in the Age of Health Care ReformFrom EverandMeeting the Needs of Older Adults with Serious Illness: Challenges and Opportunities in the Age of Health Care ReformAmy S. KelleyNo ratings yet
- What Is A Robust Health System?: FuturelearnDocument5 pagesWhat Is A Robust Health System?: FuturelearnChlodette Eizl M. LaurenteNo ratings yet
- HCM 340 7-2Document11 pagesHCM 340 7-2Robin McFaddenNo ratings yet
- Pa Issue Brief FinalDocument21 pagesPa Issue Brief FinalAsja AvdićNo ratings yet
- New Health Systems: Integrated Care and Health Inequalities ReductionFrom EverandNew Health Systems: Integrated Care and Health Inequalities ReductionNo ratings yet
- Introduction To Hospice and Palliative CareDocument16 pagesIntroduction To Hospice and Palliative Carepahat75252No ratings yet
- Universal health gaps for chronically ill older adultsDocument16 pagesUniversal health gaps for chronically ill older adultsThirza KapalNo ratings yet
- Medication Adherence in The Real WorldDocument13 pagesMedication Adherence in The Real WorldCognizantNo ratings yet
- Final Care Coordination Plan - EditedDocument9 pagesFinal Care Coordination Plan - EditedElizabeth GithinjiNo ratings yet
- Developing CountriesDocument6 pagesDeveloping CountriesShama KhanNo ratings yet
- Healthcare 3.0: How Technology Is Driving the Transition to Prosumers, Platforms and OutsuranceFrom EverandHealthcare 3.0: How Technology Is Driving the Transition to Prosumers, Platforms and OutsuranceNo ratings yet
- Comment: For Lancet On Universal Universal-Health-CoverageDocument2 pagesComment: For Lancet On Universal Universal-Health-Coverageapi-112905159No ratings yet
- FinalpaperDocument13 pagesFinalpaperapi-284899538No ratings yet
- Health Care Transition: Building a Program for Adolescents and Young Adults with Chronic Illness and DisabilityFrom EverandHealth Care Transition: Building a Program for Adolescents and Young Adults with Chronic Illness and DisabilityAlbert C. HergenroederNo ratings yet
- Treating Opioid Use Disorder in General Medical SettingsFrom EverandTreating Opioid Use Disorder in General Medical SettingsSarah E. WakemanNo ratings yet
- Early Cancer Detection in Primary Care: Are You Aware of New Blood-Based Multi-Cancer Screening ToolsFrom EverandEarly Cancer Detection in Primary Care: Are You Aware of New Blood-Based Multi-Cancer Screening ToolsNo ratings yet
- Humanising Healthcare: Patterns of Hope for a System Under StrainFrom EverandHumanising Healthcare: Patterns of Hope for a System Under StrainRating: 5 out of 5 stars5/5 (1)
- Futurescan 2021–2026: Health Care Trends and ImplicationsFrom EverandFuturescan 2021–2026: Health Care Trends and ImplicationsNo ratings yet
- The Digital Divide at An Urban Community Health CenterDocument12 pagesThe Digital Divide at An Urban Community Health CenterRizza DeaNo ratings yet
- Contemporary Community HealthDocument36 pagesContemporary Community HealthChe ThaqifNo ratings yet
- How Can HealthDocument43 pagesHow Can HealthMaria TricasNo ratings yet
- PALLIATIVE CAREDocument5 pagesPALLIATIVE CAREsanya tanejaNo ratings yet
- Bustreo F, Knaul FM, Bhadelia A, Et Al, Bull WHO, 2012Document3 pagesBustreo F, Knaul FM, Bhadelia A, Et Al, Bull WHO, 2012Sonia Xochitl Ortega AlanisNo ratings yet
- Integrative Medicine for Vulnerable Populations: A Clinical Guide to Working with Chronic and Comorbid Medical Disease, Mental Illness, and AddictionFrom EverandIntegrative Medicine for Vulnerable Populations: A Clinical Guide to Working with Chronic and Comorbid Medical Disease, Mental Illness, and AddictionNo ratings yet
- Data Makes the Difference: The Smart Nurse's Handbook for Using Data to Improve CareFrom EverandData Makes the Difference: The Smart Nurse's Handbook for Using Data to Improve CareNo ratings yet
- 1 s2.0 S2213076418300654 MainDocument5 pages1 s2.0 S2213076418300654 MaindaytdeenNo ratings yet
- Prognosis For Healthcare: The Future of Medicine: Bruce M. Cohen, M.D., PH.DDocument46 pagesPrognosis For Healthcare: The Future of Medicine: Bruce M. Cohen, M.D., PH.DSandeshGiriNo ratings yet
- Cardiovascular Nursing: Scope and Standards of PracticeFrom EverandCardiovascular Nursing: Scope and Standards of PracticeRating: 5 out of 5 stars5/5 (2)
- Policy Brief Student's Name: Institution: Course: Date of SubmissionDocument5 pagesPolicy Brief Student's Name: Institution: Course: Date of SubmissionMashNo ratings yet
- HipertensiDocument9 pagesHipertensinurmaliarizkyNo ratings yet
- Factors Affecting Medication Adherence: Patient Perspectives From Five Veterans Affairs FacilitiesDocument9 pagesFactors Affecting Medication Adherence: Patient Perspectives From Five Veterans Affairs FacilitiesErNo ratings yet
- NURS-FPX6026 - WhitneyPierre - Assessment 3-1docxDocument6 pagesNURS-FPX6026 - WhitneyPierre - Assessment 3-1docxCaroline AdhiamboNo ratings yet
- Beran & Higuchi 2013. Delivering Diabetes Care in PH & VietDocument10 pagesBeran & Higuchi 2013. Delivering Diabetes Care in PH & VietTony AbottNo ratings yet
- Health Impact Pyramid Framework Research PaperrDocument6 pagesHealth Impact Pyramid Framework Research Paperrapi-697064742No ratings yet
- Merging Current Health Care Trends: Innovative Perspective in Aging CareDocument57 pagesMerging Current Health Care Trends: Innovative Perspective in Aging CareInosha AberathneNo ratings yet
- Merging Current Health Care Trends: Innovative Perspective in Aging CareDocument75 pagesMerging Current Health Care Trends: Innovative Perspective in Aging CareInosha AberathneNo ratings yet
- HIV Prevention in Primary Care Practice: A PrEP PrimerFrom EverandHIV Prevention in Primary Care Practice: A PrEP PrimerNo ratings yet
- SummaryDocument1 pageSummaryVasquez MicoNo ratings yet
- Contemporary Community HealthDocument36 pagesContemporary Community HealthChe ThaqifNo ratings yet
- Integrating Palliative Care and Hospice Services in Long Term Care: An Eightfold Path Health Policy AnalysisDocument8 pagesIntegrating Palliative Care and Hospice Services in Long Term Care: An Eightfold Path Health Policy AnalysisIJPHSNo ratings yet
- Revitalizing the American Healthcare System: A Comprehensive Guide to Rebuilding, Reforming, and Reinventing Healthcare in the United States: Transforming the Future of Healthcare in America: A Practical and Inclusive ApproachFrom EverandRevitalizing the American Healthcare System: A Comprehensive Guide to Rebuilding, Reforming, and Reinventing Healthcare in the United States: Transforming the Future of Healthcare in America: A Practical and Inclusive ApproachNo ratings yet
- Utilizing Ehealth and Telemedicine Technologies To Enhance Access and Quality of Consultations: It'S Not What You Say, It'S The Way You Say ItDocument7 pagesUtilizing Ehealth and Telemedicine Technologies To Enhance Access and Quality of Consultations: It'S Not What You Say, It'S The Way You Say ItNoemi Salazar AbantoNo ratings yet
- 2024 APRU Case Comp Challenge Final2Document10 pages2024 APRU Case Comp Challenge Final2AnneAyushaNo ratings yet
- Chronic IllnessDocument2 pagesChronic IllnessAneelaMalikNo ratings yet
- Geissler 2015Document8 pagesGeissler 2015Jean M Huaman FiallegaNo ratings yet
- Where Are The Patients in Decision-Making About Their Own Care?Document26 pagesWhere Are The Patients in Decision-Making About Their Own Care?Nabilah TalibNo ratings yet
- Primary Health Care in USADocument4 pagesPrimary Health Care in USALoai ZabinNo ratings yet
- Research TitilDocument6 pagesResearch Titilhaimanotgedlu11No ratings yet
- Lva1 App6892Document62 pagesLva1 App6892Pallavi PalluNo ratings yet
- America's Healthcare Transformation: Strategies and InnovationsFrom EverandAmerica's Healthcare Transformation: Strategies and InnovationsNo ratings yet
- Common Health Issues: RationaleDocument7 pagesCommon Health Issues: RationaleClyde CapadnganNo ratings yet
- Global Health Initiatives 2007 enDocument32 pagesGlobal Health Initiatives 2007 enChristian Anthony CullarinNo ratings yet
- Significant Health Benefits: Global Study of Perceptions of Mobile Solutions For Healthcare in Chronic DiseaseDocument20 pagesSignificant Health Benefits: Global Study of Perceptions of Mobile Solutions For Healthcare in Chronic DiseaseSteveEpsteinNo ratings yet
- Trends Affecting NSG PracticeDocument22 pagesTrends Affecting NSG PracticeshaitabliganNo ratings yet
- RahmanDocument1 pageRahmanBM2062119PDPP Pang Kuok WeiNo ratings yet
- Product - Plan - People - 计划 - 人物Document29 pagesProduct - Plan - People - 计划 - 人物BM2062119PDPP Pang Kuok WeiNo ratings yet
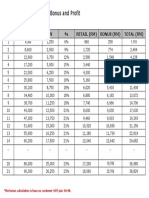
- Atmosphere Air Purifier, Bonus and Profit: QTY BV/RM PV % Retail (RM) Bonus (RM) Total (RM)Document1 pageAtmosphere Air Purifier, Bonus and Profit: QTY BV/RM PV % Retail (RM) Bonus (RM) Total (RM)BM2062119PDPP Pang Kuok WeiNo ratings yet
- Uk352481 Assiment AwsDocument3 pagesUk352481 Assiment AwsBM2062119PDPP Pang Kuok WeiNo ratings yet
- EQ and Job Satisfaction Among TeachersDocument10 pagesEQ and Job Satisfaction Among TeachersBM2062119PDPP Pang Kuok WeiNo ratings yet
- Occup Environ Med 2003Document16 pagesOccup Environ Med 2003BM2062119PDPP Pang Kuok WeiNo ratings yet
- Health Worker Motivation in Africa: The Role of Non-Financial Incentives and Human Resource Management ToolsDocument36 pagesHealth Worker Motivation in Africa: The Role of Non-Financial Incentives and Human Resource Management ToolsBM2062119PDPP Pang Kuok WeiNo ratings yet
- The Emergence of Community Health Worker Programmes in The Late Apartheid Era in South AfricaDocument29 pagesThe Emergence of Community Health Worker Programmes in The Late Apartheid Era in South AfricaBM2062119PDPP Pang Kuok WeiNo ratings yet
- Factors Underlying The Effect of Organisational Downsizing On Health of EmployeesDocument14 pagesFactors Underlying The Effect of Organisational Downsizing On Health of EmployeesBM2062119PDPP Pang Kuok WeiNo ratings yet
- Reducing Work Related Psychological Ill Health and Sickness AbsenceDocument15 pagesReducing Work Related Psychological Ill Health and Sickness AbsenceBM2062119PDPP Pang Kuok WeiNo ratings yet
- Qual Saf Health Care 2004Document19 pagesQual Saf Health Care 2004BM2062119PDPP Pang Kuok WeiNo ratings yet
- Designing and Evaluating Complex Interventions To Improve Health CareDocument11 pagesDesigning and Evaluating Complex Interventions To Improve Health CareBM2062119PDPP Pang Kuok WeiNo ratings yet
- Reducing Work Related Psychological Ill Health and Sickness AbsenceDocument15 pagesReducing Work Related Psychological Ill Health and Sickness AbsenceBM2062119PDPP Pang Kuok WeiNo ratings yet
- Factors Underlying The Effect of Organisational Downsizing On Health of EmployeesDocument14 pagesFactors Underlying The Effect of Organisational Downsizing On Health of EmployeesBM2062119PDPP Pang Kuok WeiNo ratings yet
- Occup Environ Med 2003Document16 pagesOccup Environ Med 2003BM2062119PDPP Pang Kuok WeiNo ratings yet
- Designing and Evaluating Complex Interventions To Improve Health CareDocument11 pagesDesigning and Evaluating Complex Interventions To Improve Health CareBM2062119PDPP Pang Kuok WeiNo ratings yet
- Hajipur Resume GVVDocument2 pagesHajipur Resume GVVRajnish JhaNo ratings yet
- Lesson 2 - Procedures in Cleaning Utensils and EquipmentDocument26 pagesLesson 2 - Procedures in Cleaning Utensils and EquipmentReizel TulauanNo ratings yet
- RSG 303Document196 pagesRSG 303Makinde TimiNo ratings yet
- 1605 HOBAS Jacking Pipes WebDocument16 pages1605 HOBAS Jacking Pipes Weballouche_abdNo ratings yet
- Report-Teaching English Ministery of EduDocument21 pagesReport-Teaching English Ministery of EduSohrab KhanNo ratings yet
- MJP Rate Schedule for Water Supply Pipeline ProjectDocument6 pagesMJP Rate Schedule for Water Supply Pipeline ProjectJalal TamboliNo ratings yet
- Linkstar RCST Installation Guide: Version DDocument56 pagesLinkstar RCST Installation Guide: Version Djorge_chavez01No ratings yet
- Weap - ModflowDocument20 pagesWeap - Modflowguive3No ratings yet
- INTELLISPEC SERIE V-Páginas-31-46Document16 pagesINTELLISPEC SERIE V-Páginas-31-46Antonio Valencia VillejoNo ratings yet
- 3M SS Filters Data SheetDocument4 pages3M SS Filters Data SheetbinnisfquoteNo ratings yet
- PIRA - 2022 - ESTIMATED FMV As of October 2022Document48 pagesPIRA - 2022 - ESTIMATED FMV As of October 2022Aggy ReynadoNo ratings yet
- Course Outline TP WindowsDocument6 pagesCourse Outline TP WindowsAnonymous PcPkRpAKD5No ratings yet
- CSE 323-Final-Summer 2021Document2 pagesCSE 323-Final-Summer 2021nahimur rahmanNo ratings yet
- Radiographic Examination Procedure For Asme CodeDocument33 pagesRadiographic Examination Procedure For Asme CodeEdAlmNo ratings yet
- Diosdado MacapagalDocument13 pagesDiosdado MacapagalMermie ArmentaNo ratings yet
- V200 User ManualDocument171 pagesV200 User ManualuriahskyNo ratings yet
- Data Sheet Ads1292rDocument69 pagesData Sheet Ads1292rKaha SyawalNo ratings yet
- Quickguide Students For CopyrightsDocument2 pagesQuickguide Students For Copyrightslordvorldomort100% (1)
- Asme B18.24-2020Document190 pagesAsme B18.24-2020윤규섭0% (1)
- Micro800 4-Channel and 8-Channel Analog Voltage/Current Input and Output ModulesDocument12 pagesMicro800 4-Channel and 8-Channel Analog Voltage/Current Input and Output ModulesSyarifudin WahidNo ratings yet
- Gujrat Newspaper IndustryDocument14 pagesGujrat Newspaper IndustryAlok MahajanNo ratings yet
- v16 n3Document219 pagesv16 n3Mark ReinhardtNo ratings yet
- 2020会社案内(英語版)Document18 pages2020会社案内(英語版)DAC ORGANIZERNo ratings yet
- Beef Steaks: MethodDocument2 pagesBeef Steaks: MethodGoshigoshi AkhtarNo ratings yet
- (MATH1013) (2016) (F) Midterm Wsuab 41338Document9 pages(MATH1013) (2016) (F) Midterm Wsuab 41338陳希程No ratings yet
- Pub1308 WebDocument193 pagesPub1308 WebyucemanNo ratings yet
- Historical Background of The SchoolDocument2 pagesHistorical Background of The SchoolJoel Daen50% (2)
- Company Electronics Appliances Semiconductors South Korea's: SamsungDocument61 pagesCompany Electronics Appliances Semiconductors South Korea's: Samsunghaseeb ahmedNo ratings yet
- KPW FSO Yetagun Presentation 250713Document36 pagesKPW FSO Yetagun Presentation 250713muhamadrafie1975No ratings yet
- Teachers' Notes: ©film Education 1Document20 pagesTeachers' Notes: ©film Education 1רז ברקוNo ratings yet