You might also like
- Principles of Measurement and Transduction of Biomedical VariablesFrom EverandPrinciples of Measurement and Transduction of Biomedical VariablesNo ratings yet
- Is 6665-1985Document33 pagesIs 6665-1985t_syamprasadNo ratings yet
- 100 Beded Hospital NormsDocument56 pages100 Beded Hospital NormsRAJU100% (1)
- Indian Standard For Hospital Building Part-1Document23 pagesIndian Standard For Hospital Building Part-1Raja Singh100% (1)
- IEC 61730 Part 2 PDFDocument41 pagesIEC 61730 Part 2 PDFJatinBatra0% (1)
- Assignment 2 (Lighting)Document26 pagesAssignment 2 (Lighting)Hari HaranNo ratings yet
- The Physics and Technology of Diagnostic Ultrasound: Study Guide (Second Edition)From EverandThe Physics and Technology of Diagnostic Ultrasound: Study Guide (Second Edition)No ratings yet
- Review Journal Articles FinalDocument6 pagesReview Journal Articles FinalLeo PilayanNo ratings yet
- Indian STDS!!Document36 pagesIndian STDS!!Rishi BalanNo ratings yet
- Is 16108 2012Document45 pagesIs 16108 2012Ajay SatputeNo ratings yet
- Energy Efficient Lighting System Design For Hospitals Diagnostic and Treatment Room - A Case StudyDocument9 pagesEnergy Efficient Lighting System Design For Hospitals Diagnostic and Treatment Room - A Case StudySafaa AlzubaidiNo ratings yet
- Disclosure To Promote The Right To InformationDocument58 pagesDisclosure To Promote The Right To InformationAnamika TiwaryNo ratings yet
- Is 16101 2012Document17 pagesIs 16101 2012gayathrikanduriNo ratings yet
- Is.3646.1.1992 PDF Knowledge Is Such A Treasure It Can Not Be StolenDocument38 pagesIs.3646.1.1992 PDF Knowledge Is Such A Treasure It Can Not Be StolensandeshsmsNo ratings yet
- IEC 60601-2-24 Ed. 1 (1998) (Indian Edition)Document67 pagesIEC 60601-2-24 Ed. 1 (1998) (Indian Edition)Matteo AgenoNo ratings yet
- Disclosure To Promote The Right To InformationDocument31 pagesDisclosure To Promote The Right To InformationEr Chandra BoseNo ratings yet
- GRDCF013013 PDFDocument2 pagesGRDCF013013 PDFGRD JournalsNo ratings yet
- Is.8913.1978 Lamp Cap Temperature RiseDocument16 pagesIs.8913.1978 Lamp Cap Temperature RiselightbulbdepotNo ratings yet
- Is 4758 1968Document19 pagesIs 4758 1968karthikraja21No ratings yet
- IISc ReportDocument37 pagesIISc ReportNita HarwediNo ratings yet
- Is Iec 62353 2007 PDFDocument55 pagesIs Iec 62353 2007 PDFSofroni CatalinNo ratings yet
- Effective Lighting Design Standards Impacting Pati00Document8 pagesEffective Lighting Design Standards Impacting Pati00KeerthiNo ratings yet
- 5th Sem Syllabus BMEDocument17 pages5th Sem Syllabus BMENuthal SrinivasanNo ratings yet
- Iec 60688 - 2002Document37 pagesIec 60688 - 2002bilgiislem773267% (3)
- Healthcare Interpretation of IEE Guidance Note 7 (Chapter 10) and IEC 60364-7-710 ForDocument31 pagesHealthcare Interpretation of IEE Guidance Note 7 (Chapter 10) and IEC 60364-7-710 Forjlruizmat8679100% (1)
- Is.13450.2.30.2008 - NIBPDocument46 pagesIs.13450.2.30.2008 - NIBPqvc.regulatory 2No ratings yet
- Is 6262 1971Document19 pagesIs 6262 1971just_4_u_dear_in9549No ratings yet
- Design of An Intelligent and Efficient Light Control SystemDocument4 pagesDesign of An Intelligent and Efficient Light Control SystemATSNo ratings yet
- Is 13585 3 2013Document14 pagesIs 13585 3 2013wfweggweNo ratings yet
- Is 1881 1998Document16 pagesIs 1881 1998Sunnil JhaNo ratings yet
- Format For 2page Report On OT LightDocument3 pagesFormat For 2page Report On OT LightSwati TiwariNo ratings yet
- Relevance of The Structure of Time Resolved Spectral Output To Light Tissue Interaction Using Intense Pulsed Light (IPL) - C Ash, G Town, P BjerringDocument10 pagesRelevance of The Structure of Time Resolved Spectral Output To Light Tissue Interaction Using Intense Pulsed Light (IPL) - C Ash, G Town, P BjerringCaerwyn AshNo ratings yet
- SPIE2022 SCalDocument24 pagesSPIE2022 SCalLucia SuarezNo ratings yet
- Is 3842 2 1966Document21 pagesIs 3842 2 1966Ramesh AnanthanarayananNo ratings yet
- Electrical in Medical LocationDocument32 pagesElectrical in Medical LocationengrrafNo ratings yet
- IS CODE Fire ResistantDocument25 pagesIS CODE Fire ResistantSunil KalwaniyaNo ratings yet
- Is Iso 14708 3 2008Document52 pagesIs Iso 14708 3 2008Hemant SharmaNo ratings yet
- Disclosure To Promote The Right To InformationDocument10 pagesDisclosure To Promote The Right To InformationduonzaNo ratings yet
- Is 9334 1986Document20 pagesIs 9334 1986rajpd28No ratings yet
- Is 1401 2008Document30 pagesIs 1401 2008Andrea B. OpazoNo ratings yet
- Brochure HyLED 7 Series-ESDocument7 pagesBrochure HyLED 7 Series-ESPablo RodriguezNo ratings yet
- Echelon SmartDocument5 pagesEchelon SmartTài NguyễnNo ratings yet
- LIFE DETECTION SYSTEM USING L AND S BAND MICROWAVE Final Seminar ReportDocument29 pagesLIFE DETECTION SYSTEM USING L AND S BAND MICROWAVE Final Seminar ReportRahul K100% (1)
- Is.11955.1987 Preferred Current Ratings PDFDocument8 pagesIs.11955.1987 Preferred Current Ratings PDFMukesh KumarNo ratings yet
- Iec 62233 2005Document47 pagesIec 62233 2005Andres RojasNo ratings yet
- Disclosure To Promote The Right To InformationDocument16 pagesDisclosure To Promote The Right To Informationrajpd28No ratings yet
- ICEL Design GuideDocument15 pagesICEL Design GuideAlbert TuazonNo ratings yet
- Base PaperDocument4 pagesBase PaperAayush AnshuNo ratings yet
- Is Iso 11979 2 1999Document29 pagesIs Iso 11979 2 1999Vinay PatelNo ratings yet
- Is Iec 61724 1998Document21 pagesIs Iec 61724 1998Tankut YolsalNo ratings yet
- Disclosure To Promote The Right To InformationDocument20 pagesDisclosure To Promote The Right To InformationAshish KambojNo ratings yet
- Icel 1006 Emergency Lighting Design Guide Hyp 10-1-2013 PDF 1360669544Document31 pagesIcel 1006 Emergency Lighting Design Guide Hyp 10-1-2013 PDF 1360669544felipegonzalezmarquezNo ratings yet
- Is/iec 60079.30.1.2007Document31 pagesIs/iec 60079.30.1.2007camspsNo ratings yet
- Is 10322-5-1 (Bis)Document8 pagesIs 10322-5-1 (Bis)Prabhat mani tripathiNo ratings yet
- Report DesignDocument81 pagesReport DesignMUHAMMAD MUNIR ASYRAF BIN AB RAZAK STUDENTNo ratings yet
- ASSIST LEDLife Revised2007 PDFDocument34 pagesASSIST LEDLife Revised2007 PDFAnonymous 8jFcogqgSlNo ratings yet
- Iso Iec-60793.1.40.2001Document29 pagesIso Iec-60793.1.40.2001Néstor PeñaNo ratings yet
- IEC 60793-1-52 (2001) Change of TemperatureDocument10 pagesIEC 60793-1-52 (2001) Change of TemperaturejudyyangchNo ratings yet
- Dosimetry in Brachytherapy – An International Code of Practice for Secondary Standards Dosimetry Laboratories and HospitalsFrom EverandDosimetry in Brachytherapy – An International Code of Practice for Secondary Standards Dosimetry Laboratories and HospitalsNo ratings yet
- Practical Power Electronics: Applications, Experiments and AnimationsFrom EverandPractical Power Electronics: Applications, Experiments and AnimationsNo ratings yet
- Power Electronics Applied to Industrial Systems and Transports, Volume 1: Synthetic Methodology to Converters and Components TechnologyFrom EverandPower Electronics Applied to Industrial Systems and Transports, Volume 1: Synthetic Methodology to Converters and Components TechnologyNo ratings yet
- Letter HeadDocument3 pagesLetter HeadAhmedBIowarNo ratings yet
- The Tamil Nadu Buildings (Lease and Rent Control) Act, 1960Document62 pagesThe Tamil Nadu Buildings (Lease and Rent Control) Act, 1960AhmedBIowarNo ratings yet
- House of Santa: Architecture CompetitionDocument10 pagesHouse of Santa: Architecture CompetitionAhmedBIowarNo ratings yet
- Detailed Cost Estimate: For Construction ofDocument8 pagesDetailed Cost Estimate: For Construction ofAhmedBIowarNo ratings yet
- Finals FDocument1 pageFinals FAhmedBIowarNo ratings yet
- FINALSEC1Document1 pageFINALSEC1AhmedBIowarNo ratings yet
- Final NorthDocument1 pageFinal NorthAhmedBIowarNo ratings yet
- LED Lighting Solutions Brochure PDFDocument7 pagesLED Lighting Solutions Brochure PDFAhmedBIowarNo ratings yet
- Final EastDocument1 pageFinal EastAhmedBIowarNo ratings yet
- Nabh Ac For Ot AbrigedDocument5 pagesNabh Ac For Ot AbrigedAhmedBIowarNo ratings yet
- FINALSEC2Document1 pageFINALSEC2AhmedBIowarNo ratings yet
- FINALg FHDocument1 pageFINALg FHAhmedBIowarNo ratings yet
- FINALg FHDocument1 pageFINALg FHAhmedBIowarNo ratings yet
- Murali Architects Application Form - AhamedmvDocument2 pagesMurali Architects Application Form - AhamedmvAhmedBIowarNo ratings yet
- Final FFDocument1 pageFinal FFAhmedBIowarNo ratings yet
- Barch BS Q&A Papers 4Document8 pagesBarch BS Q&A Papers 4AhmedBIowarNo ratings yet
- NOMOGRAMDocument6 pagesNOMOGRAMAhmedBIowarNo ratings yet
- Produced by An Autodesk Educational ProductDocument1 pageProduced by An Autodesk Educational ProductAhmedBIowarNo ratings yet
- New Doc 7Document4 pagesNew Doc 7AhmedBIowarNo ratings yet
- General NotesDocument19 pagesGeneral NotesAhmedBIowarNo ratings yet
- Produced by An Autodesk Educational ProductDocument1 pageProduced by An Autodesk Educational ProductAhmedBIowarNo ratings yet
- Produced by An Autodesk Educational ProductDocument1 pageProduced by An Autodesk Educational ProductAhmedBIowarNo ratings yet
- Detail 1: Frank Lloyd Wright'S ChairDocument1 pageDetail 1: Frank Lloyd Wright'S ChairAhmedBIowarNo ratings yet
- Produced by An Autodesk Educational ProductDocument1 pageProduced by An Autodesk Educational ProductAhmedBIowarNo ratings yet
- Produced by An Autodesk Educational ProductDocument1 pageProduced by An Autodesk Educational ProductAhmedBIowarNo ratings yet
- Produced by An Autodesk Educational ProductDocument1 pageProduced by An Autodesk Educational ProductAhmedBIowarNo ratings yet
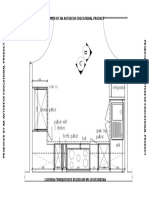
- Consultation Room Waiting AreaDocument4 pagesConsultation Room Waiting AreaAhmedBIowarNo ratings yet
- Flow Chart Process of Chicago PizzaDocument14 pagesFlow Chart Process of Chicago PizzaTanisha AgarwalNo ratings yet
- The Effect of Amendment of Fish Waste Fertilizer To Soil and Its Impact On The Growth and Nutritional Status of Trigonella Foenum-GraecumDocument5 pagesThe Effect of Amendment of Fish Waste Fertilizer To Soil and Its Impact On The Growth and Nutritional Status of Trigonella Foenum-GraecumInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Project Proposal ExampleDocument8 pagesProject Proposal ExampleplayerNo ratings yet
- 10 Distinctive Features of The Japanese Education System That Made This Nation The Envy of The WorldDocument6 pages10 Distinctive Features of The Japanese Education System That Made This Nation The Envy of The WorldHasniaty AbdullahNo ratings yet
- Iscar CatalogoDocument184 pagesIscar CatalogoJ Ferreyra LibanoNo ratings yet
- Community Based Disaster Management Training For Nursing StudentsDocument14 pagesCommunity Based Disaster Management Training For Nursing StudentsNeli HusniawatiNo ratings yet
- Week 11 - Transfer and TransportDocument28 pagesWeek 11 - Transfer and TransportHamza Noor100% (1)
- TantalumDocument16 pagesTantalumjosevitorromualdoNo ratings yet
- Semiconductor PhysicsDocument54 pagesSemiconductor PhysicsGod KillerNo ratings yet
- COO Retail Restaurant Hospitality in Dallas FT Worth TX Resume Randall McGeeDocument2 pagesCOO Retail Restaurant Hospitality in Dallas FT Worth TX Resume Randall McGeeRandallMcGee100% (1)
- Fluidized Bed SystemsDocument20 pagesFluidized Bed SystemsVaijayanti JoshiNo ratings yet
- 03 Basic Principles of Ion ChromatographyDocument3 pages03 Basic Principles of Ion ChromatographyImad AghilaNo ratings yet
- TDS Nitozinc Primer IndiaDocument3 pagesTDS Nitozinc Primer Indiasyed AffanNo ratings yet
- Mobilfluid 426Document2 pagesMobilfluid 426tribolasNo ratings yet
- Malaika Synopsis PresentationDocument23 pagesMalaika Synopsis PresentationSundas SaikhuNo ratings yet
- India Energy Week 2023 Call For Papers BrochureDocument12 pagesIndia Energy Week 2023 Call For Papers BrochureaharnishaNo ratings yet
- B1 Quiz 2Document2 pagesB1 Quiz 2Назар КуликNo ratings yet
- Triptico InglesDocument3 pagesTriptico InglesHelmer Álvaro Aguirre VillcaNo ratings yet
- Utkal University BA Hons. Psychology SyllabusDocument30 pagesUtkal University BA Hons. Psychology SyllabusSK Imdad100% (1)
- 13-02 - Sewage Disposal SystemDocument19 pages13-02 - Sewage Disposal SystemFolayemiNo ratings yet
- Permeability: Tri-Flex 2 Five-Cell Permeability Test System Tri-Flex 2 Three-Cell Permeability Test SystemDocument7 pagesPermeability: Tri-Flex 2 Five-Cell Permeability Test System Tri-Flex 2 Three-Cell Permeability Test SystemJorge SanchezNo ratings yet
- Angelina Hull Student - Heritagehs - Argumentative Essay - Student Name - Class Period - Spring 19 - H English 1Document5 pagesAngelina Hull Student - Heritagehs - Argumentative Essay - Student Name - Class Period - Spring 19 - H English 1api-461590822No ratings yet
- TRN1580530 7698837 Clinical Report 1666029364641932Document6 pagesTRN1580530 7698837 Clinical Report 1666029364641932pratimadeshlahreNo ratings yet
- Offshore Pre Asses FormDocument8 pagesOffshore Pre Asses Formwendyphan09No ratings yet
- Happiness Advantage - Achor.ebsDocument10 pagesHappiness Advantage - Achor.ebsanand100% (1)
- Synthetic DyesDocument12 pagesSynthetic DyesBhagyashree VoraNo ratings yet
- Mpac1000 SpecDocument6 pagesMpac1000 SpecalstomNo ratings yet
- HITACHI RAC Brochure Generic 08Document33 pagesHITACHI RAC Brochure Generic 08Charalampos KovrasNo ratings yet
- MN Nurse Practice ActsDocument7 pagesMN Nurse Practice Actsapi-390136268No ratings yet