You might also like
- Amlodipine Byslate Drug StudyDocument1 pageAmlodipine Byslate Drug StudyWenalyn Grace Abella Llavan71% (7)
- Electricity From WalkingDocument8 pagesElectricity From WalkingSanthosh100% (6)
- Daño Hepatico Manejo DolorDocument6 pagesDaño Hepatico Manejo DolorAngélica Valenzuela AndrighiNo ratings yet
- The Practical Management of Gout: Lan X. Chen, MD, PHD H. Ralph Schumacher, JR, MDDocument4 pagesThe Practical Management of Gout: Lan X. Chen, MD, PHD H. Ralph Schumacher, JR, MDLydia Hapsari SudjonoNo ratings yet
- Toradol KetorolacDocument2 pagesToradol KetorolacE100% (4)
- 201803-04 - APC Memo Enclosure - Guidance For Safe and Effective Use of Proton Pump Inhibitors - March-April 2018Document4 pages201803-04 - APC Memo Enclosure - Guidance For Safe and Effective Use of Proton Pump Inhibitors - March-April 2018Ng ShNo ratings yet
- Proton Pump InhibitorDocument9 pagesProton Pump InhibitorAnkush BiswasNo ratings yet
- Care Plan:, Wrong, Wrong, Wrong, WrongDocument8 pagesCare Plan:, Wrong, Wrong, Wrong, Wronglovelylife theNo ratings yet
- Drug Study IbuprofenDocument3 pagesDrug Study IbuprofenblaireNo ratings yet
- Perioperative CVS MedicationDocument3 pagesPerioperative CVS MedicationAminn Alhassan ContehNo ratings yet
- Gastro RefluxDocument8 pagesGastro RefluxlestariNo ratings yet
- Analgesia in Patients With Impaired Renal Function PDFDocument4 pagesAnalgesia in Patients With Impaired Renal Function PDFAnonymous hF5zAdvwCC100% (1)
- Ther. Class. PO: (Adults) 5-10 MG Once Daily : AntihypertensivesDocument5 pagesTher. Class. PO: (Adults) 5-10 MG Once Daily : AntihypertensivesCliff by the seaNo ratings yet
- Non Steroidal Anti-Inflammatory Drugs (NSAIDs)Document16 pagesNon Steroidal Anti-Inflammatory Drugs (NSAIDs)Dilan GalaryNo ratings yet
- WHO Step Ladder For PainDocument5 pagesWHO Step Ladder For PainRizKyImanSariNo ratings yet
- DS (Ibuprofen)Document6 pagesDS (Ibuprofen)Mary April MendezNo ratings yet
- Generic Name Indication (S) Action Adverse Reaction Interaction Contraindication Patient Teaching Nursing ImplicationsDocument2 pagesGeneric Name Indication (S) Action Adverse Reaction Interaction Contraindication Patient Teaching Nursing ImplicationsJake Yvan DizonNo ratings yet
- Drug Prescribing in Renal Impairment Information. Patient PatientDocument13 pagesDrug Prescribing in Renal Impairment Information. Patient PatientEffy AngeLi LomocsoNo ratings yet
- Clinical Liver Disease - 2018 - Rakoski - Pain Management in Patients With CirrhosisDocument6 pagesClinical Liver Disease - 2018 - Rakoski - Pain Management in Patients With CirrhosisCika Zahrah DewisoniaNo ratings yet
- ToradolDocument2 pagesToradolAdrianne Bazo100% (1)
- Summary of Product Characteristics (SMPC)Document13 pagesSummary of Product Characteristics (SMPC)Asif ZamanNo ratings yet
- 776 NSAIDsguidelinesDraftV2Nov09Document3 pages776 NSAIDsguidelinesDraftV2Nov09KavirNivNo ratings yet
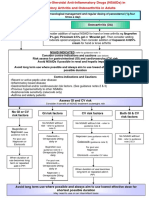
- Avoiding The "Triple Whammy" in Primary Care:: ACE inhibitor/ARB + Diuretic + NSAIDDocument5 pagesAvoiding The "Triple Whammy" in Primary Care:: ACE inhibitor/ARB + Diuretic + NSAIDSintaNo ratings yet
- Prudent Use of NSAIDs in Patients With COVID-19, Dengue, and ChikungunyaDocument2 pagesPrudent Use of NSAIDs in Patients With COVID-19, Dengue, and ChikungunyaA. K. MohiuddinNo ratings yet
- NSAID Prescribing Precautions: Amanda Risser, MD, MPH Deirdre Donovan, MD John Heintzman, MD and Tanya Page, MDDocument8 pagesNSAID Prescribing Precautions: Amanda Risser, MD, MPH Deirdre Donovan, MD John Heintzman, MD and Tanya Page, MDNavdeep RandhawaNo ratings yet
- Clinical Med CardsDocument26 pagesClinical Med CardsLila DanielsNo ratings yet
- Drug StudyDocument3 pagesDrug StudyKrishna Faith P. DelaraNo ratings yet
- TB Guideline RenalDocument12 pagesTB Guideline RenalLeniza SorianoNo ratings yet
- Woodell2018 (Jurnal Asli)Document13 pagesWoodell2018 (Jurnal Asli)Fatah Jati PNo ratings yet
- MA Drug StudyDocument2 pagesMA Drug StudyJane Decenine CativoNo ratings yet
- Gasto Protection With PPIDocument3 pagesGasto Protection With PPI4g5xwdvh9sNo ratings yet
- Drug Study (Uterine Atony)Document14 pagesDrug Study (Uterine Atony)Violy CabigatNo ratings yet
- Avapro (Irbesartan)Document2 pagesAvapro (Irbesartan)ENo ratings yet
- Antiepileptic Drugs and Liver Disease 2017Document14 pagesAntiepileptic Drugs and Liver Disease 2017Pablo Sebastián SaezNo ratings yet
- Drug StudyDocument7 pagesDrug StudyZhaira LilangNo ratings yet
- El Indice Predicto de Hemorragia DigestivaDocument1 pageEl Indice Predicto de Hemorragia DigestivaOlga SamameNo ratings yet
- 2018 Tto Del SN CorticoresistenteDocument11 pages2018 Tto Del SN CorticoresistenteJeff Daniel Landauro PanayNo ratings yet
- MEFTAL P Suspension PIDocument10 pagesMEFTAL P Suspension PIpiyush patelNo ratings yet
- Deep Vein ThrombosisDocument4 pagesDeep Vein ThrombosisStefania CristinaNo ratings yet
- Drug StudyDocument9 pagesDrug StudyComia AltheiaNo ratings yet
- Protocol 010Document12 pagesProtocol 010hatem newishyNo ratings yet
- AmlodipineDocument2 pagesAmlodipineAnonymous QqyLDoW1No ratings yet
- Prinivil LisinoprilDocument3 pagesPrinivil LisinoprilENo ratings yet
- Dos and Don'ts in The Management of Cirrhosis: A View From The 21st CenturyDocument5 pagesDos and Don'ts in The Management of Cirrhosis: A View From The 21st CenturySebastian BurgosNo ratings yet
- A Comprehensive Review of Non-Steroidal Anti-Inflammatory Drug Use in The ElderlyDocument8 pagesA Comprehensive Review of Non-Steroidal Anti-Inflammatory Drug Use in The ElderlyElfiyanti SeptianNo ratings yet
- Ibuprofen 150mg + Paracetamol 500mg (Combodex)Document15 pagesIbuprofen 150mg + Paracetamol 500mg (Combodex)ddandan_2No ratings yet
- Final Sup Bree AMDGPostop Pain 091318 WcoverDocument14 pagesFinal Sup Bree AMDGPostop Pain 091318 WcoveroNo ratings yet
- Summary of Product Characteristics: Apsifen-F Ibuprofen 600 MG Film-Coated TabletsDocument12 pagesSummary of Product Characteristics: Apsifen-F Ibuprofen 600 MG Film-Coated TabletsMeriam Gita Maulia SuhaidiNo ratings yet
- Drug Name Drug Interactions Nursing ConsiderationsDocument4 pagesDrug Name Drug Interactions Nursing ConsiderationsPagodNo ratings yet
- Ranitidine HCLDocument3 pagesRanitidine HCLdanny17phNo ratings yet
- Drug StudyDocument2 pagesDrug StudyTrexie ScattNo ratings yet
- KETOROLACDocument1 pageKETOROLACJugen Gumba Fuentes AlquizarNo ratings yet
- Folic CHNDocument3 pagesFolic CHNErica EbradaNo ratings yet
- SE - Brufen 800 - SMPCDocument12 pagesSE - Brufen 800 - SMPCSrechko MilichNo ratings yet
- Ibuprofen Arrow Care TabDocument9 pagesIbuprofen Arrow Care TabshajahanputhusseriNo ratings yet
- Drug Mechanism of Action Indication Contraindication Adverse Effect Nursing Considerations Generic NameDocument2 pagesDrug Mechanism of Action Indication Contraindication Adverse Effect Nursing Considerations Generic NameJohn Edward EscoteNo ratings yet
- Monograph MetronidazoleDocument4 pagesMonograph MetronidazoleAli MehdiNo ratings yet
- NCMB317: RupturedDocument12 pagesNCMB317: RupturedArmand Bong Santiago100% (1)
- CoversylDocument3 pagesCoversylianecunarNo ratings yet
- Infusion Therapy: For Pain, Headache and Related ConditionsFrom EverandInfusion Therapy: For Pain, Headache and Related ConditionsAlaa Abd-ElsayedNo ratings yet
- The Bleaching: Learning Objectives OutcomesDocument13 pagesThe Bleaching: Learning Objectives Outcomesالعمري العمريNo ratings yet
- Dental Implants: Maintenance, Care and Treatment of Peri-Implant InfectionDocument9 pagesDental Implants: Maintenance, Care and Treatment of Peri-Implant Infectionالعمري العمريNo ratings yet
- Final Senior Signature:: Student Name: Student NameDocument1 pageFinal Senior Signature:: Student Name: Student Nameالعمري العمريNo ratings yet
- Warning of use analgesic in dentistry دادعا يرمعلا رمع يرهزلا قراط هلمعش سنا:روكدلا فرشا تحتDocument8 pagesWarning of use analgesic in dentistry دادعا يرمعلا رمع يرهزلا قراط هلمعش سنا:روكدلا فرشا تحتالعمري العمريNo ratings yet
- UST DocumentDocument3 pagesUST Documentالعمري العمريNo ratings yet
- Warning of use analgesic in dentistry دادعا يرمعلا رمع يرهزلا قراط هلمعش سنا:روكدلا فرشا تحتDocument8 pagesWarning of use analgesic in dentistry دادعا يرمعلا رمع يرهزلا قراط هلمعش سنا:روكدلا فرشا تحتالعمري العمريNo ratings yet
- Dry Mouth English May2019 ١Document8 pagesDry Mouth English May2019 ١العمري العمريNo ratings yet
- Dry-Mouth English May2019Document8 pagesDry-Mouth English May2019العمري العمريNo ratings yet
- Symptom Management Guidelines: XEROSTOMIADocument9 pagesSymptom Management Guidelines: XEROSTOMIAالعمري العمريNo ratings yet
- What Is Dry MouthDocument1 pageWhat Is Dry Mouthالعمري العمريNo ratings yet
- Dry Mouth EnglishDocument1 pageDry Mouth Englishالعمري العمريNo ratings yet
- Othodontic Case ReportDocument3 pagesOthodontic Case Reportالعمري العمريNo ratings yet
- Types of Bleaching: A-Non-vital Bleaching Techniques (Internal Bleaching)Document4 pagesTypes of Bleaching: A-Non-vital Bleaching Techniques (Internal Bleaching)العمري العمريNo ratings yet
- Dry Mouth English May2019 ١Document8 pagesDry Mouth English May2019 ١العمري العمريNo ratings yet
- BleachingDocument7 pagesBleachingالعمري العمريNo ratings yet
- First Lecture Studying Notes - MFPDocument12 pagesFirst Lecture Studying Notes - MFPالعمري العمريNo ratings yet
- SensorsDocument69 pagesSensorsRiahi Rezeg100% (1)
- Daa Unit-1Document44 pagesDaa Unit-1passion jobNo ratings yet
- E18 RedoxDocument4 pagesE18 RedoxAnonymous 6kkvjfx3100% (1)
- List of Top Paid Keywords On Google AdsenseDocument4 pagesList of Top Paid Keywords On Google AdsenseRobert DurăNo ratings yet
- Arts 6 Module 1Document18 pagesArts 6 Module 1Elexthéo JoseNo ratings yet
- University of Mumbai: (Computer Systems and ApplicationsDocument21 pagesUniversity of Mumbai: (Computer Systems and ApplicationsManish YadavNo ratings yet
- FAQ Cork Fabric Folclore Crafts 2018Document7 pagesFAQ Cork Fabric Folclore Crafts 2018gabrielampNo ratings yet
- GECG Curriculum - Biomedical EngineeringDocument52 pagesGECG Curriculum - Biomedical Engineeringdhruv7887No ratings yet
- 2Document1 page2Dedes SahpitraNo ratings yet
- Tcs Eis Case Study BPCLDocument4 pagesTcs Eis Case Study BPCLsumitkr_20181No ratings yet
- Writing A Parable (Grade 8)Document16 pagesWriting A Parable (Grade 8)JON-VIC FIGUEROANo ratings yet
- V1 Exam 1 AfternoonDocument31 pagesV1 Exam 1 AfternoonajnigelNo ratings yet
- IJACSA - Volume 3 No. 6, June 2012Document151 pagesIJACSA - Volume 3 No. 6, June 2012Editor IJACSANo ratings yet
- Fat Loss Plan - Week 4Document2 pagesFat Loss Plan - Week 4John RohrerNo ratings yet
- Back To School WorksheetDocument8 pagesBack To School WorksheetВаняNo ratings yet
- Multiple Integrals: Example 3 SolutionDocument15 pagesMultiple Integrals: Example 3 SolutionshivanshNo ratings yet
- Tonepad Pedal RATDocument0 pagesTonepad Pedal RATJose David DíazNo ratings yet
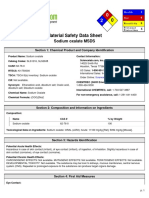
- Msds PDFDocument5 pagesMsds PDFkleaxeyaNo ratings yet
- 12th Sprint Reloaded-SolutionsDocument47 pages12th Sprint Reloaded-SolutionsMuhammad Anas BilalNo ratings yet
- The Emerging Field of Human Social GenomicsDocument18 pagesThe Emerging Field of Human Social GenomicsEdilson RodriguesNo ratings yet
- High Availability Cluster - Proxmox VEDocument4 pagesHigh Availability Cluster - Proxmox VEDhani MultisolutionNo ratings yet
- UntitledDocument336 pagesUntitledChristine CagunanNo ratings yet
- Unit 2Document7 pagesUnit 2Hind HindouNo ratings yet
- SET 1 - MOCK ALE Day 2 Design ProblemsDocument6 pagesSET 1 - MOCK ALE Day 2 Design Problemsallyssa monica duNo ratings yet
- Qualcast Trucks Catalog2015Document188 pagesQualcast Trucks Catalog2015Edwin Javier Garavito100% (2)
- DEVICE Exp 4 StudentDocument4 pagesDEVICE Exp 4 StudentTouhid AlamNo ratings yet
- Sf2460i Line 163Document123 pagesSf2460i Line 163Santiago SilvaNo ratings yet
- WA 05 Unit Test 01 Listening ScriptsDocument1 pageWA 05 Unit Test 01 Listening ScriptsEden GamaNo ratings yet
- EpicsDocument5 pagesEpicsLynette JavaNo ratings yet