You might also like
- PHYSICAL EXAMINATION-Head To Toe ExaminationDocument4 pagesPHYSICAL EXAMINATION-Head To Toe Examinationsubi100% (1)
- 17.1 PN Ass-1 MCDocument11 pages17.1 PN Ass-1 MCvicky RoseNo ratings yet
- Identification Data of PatientDocument8 pagesIdentification Data of Patientanimesh panda50% (2)
- Physical Exxamination FormatDocument6 pagesPhysical Exxamination FormatElzi JonesNo ratings yet
- Case Study FormatDocument15 pagesCase Study FormatLavie GangwarNo ratings yet
- College of Nursing Theni Medical College Theni Child Health Nursing Health Assessment of Todder PlacementDocument16 pagesCollege of Nursing Theni Medical College Theni Child Health Nursing Health Assessment of Todder PlacementBasit RamzanNo ratings yet
- Nursing Care PlanDocument14 pagesNursing Care Plananimesh panda100% (3)
- LAPORAN KASUS Sol IntracranialDocument96 pagesLAPORAN KASUS Sol IntracranialJessica FilbertineNo ratings yet
- Case Presentation On CVTDocument32 pagesCase Presentation On CVTraman kumariNo ratings yet
- Cardiac System AssessmentDocument14 pagesCardiac System AssessmentValarmathi100% (1)
- Medical Certificate For Service at Sea: ConfidentialDocument4 pagesMedical Certificate For Service at Sea: ConfidentialADMIN MCU RSU SAHID SAHIRMAN100% (1)
- Case Presentation On Ischemic StrokeDocument55 pagesCase Presentation On Ischemic StrokeNisha GuptaNo ratings yet
- Bronchial Asthma Careplan BBDocument26 pagesBronchial Asthma Careplan BBKshayna 1234No ratings yet
- Running Head: NURSING CASE STUDY/BONE FRACTURE DIP/2017/00451 1Document22 pagesRunning Head: NURSING CASE STUDY/BONE FRACTURE DIP/2017/00451 1Mur DerNo ratings yet
- Acute CaseDocument20 pagesAcute CaseNarendran MuthusamyNo ratings yet
- Cheryztie Amythyst BenedictDocument4 pagesCheryztie Amythyst Benedictvincent SutejoNo ratings yet
- Care Plan FormatDocument14 pagesCare Plan FormatAndalNo ratings yet
- Careplan II Fundamentals III FinalDocument28 pagesCareplan II Fundamentals III FinalRebecca RathburnNo ratings yet
- Division For Foreign Students With Instructions Conducted in English LanguageDocument10 pagesDivision For Foreign Students With Instructions Conducted in English LanguagesharenNo ratings yet
- NC Khairunnisa - NeuroDocument18 pagesNC Khairunnisa - NeuroDodi DiNo ratings yet
- Physical Examination FormatDocument7 pagesPhysical Examination FormatHiba V.ANo ratings yet
- RoseaDocument41 pagesRoseaRupali ShaNo ratings yet
- Case StudyDocument32 pagesCase Studyanimesh pandaNo ratings yet
- Sevegan IIDocument14 pagesSevegan IIDwyane Tyrone CabrillosNo ratings yet
- Case Presentation: Aplastic AnemiaDocument19 pagesCase Presentation: Aplastic AnemiaIntanZanariahSharuddinNo ratings yet
- CASE Study ENCEPHALITISDocument29 pagesCASE Study ENCEPHALITISMeena Koushal67% (3)
- PMR emDocument20 pagesPMR emNabighah ZukriNo ratings yet
- Case Report CHFDocument25 pagesCase Report CHFevi septri andayaniNo ratings yet
- History CollectionDocument15 pagesHistory Collectionroseline vinodiNo ratings yet
- Care Plan of Asthma 1Document15 pagesCare Plan of Asthma 1chaudharitrushar007No ratings yet
- Medical Resume DanielleDocument3 pagesMedical Resume DanielleangelbertooNo ratings yet
- I. Patient Assessment Profile of PatientDocument11 pagesI. Patient Assessment Profile of PatientAnweshaNo ratings yet
- Nursing Care Plan.Document8 pagesNursing Care Plan.animesh panda100% (3)
- JJHJGKKJJDocument9 pagesJJHJGKKJJJohn SimsNo ratings yet
- Total Care Assessment Tool AdultsDocument11 pagesTotal Care Assessment Tool AdultsAnaleah MalayaoNo ratings yet
- High Risk Antenatal AssessmentDocument15 pagesHigh Risk Antenatal AssessmentAbishaNo ratings yet
- MG Case StudyDocument12 pagesMG Case StudyPiyali SahaNo ratings yet
- Responsi Kelompok 3 Stroke Non HemoragikDocument19 pagesResponsi Kelompok 3 Stroke Non HemoragikAnresangsya YasaNo ratings yet
- Post Natal AssessmentDocument8 pagesPost Natal Assessmentmohapatra devNo ratings yet
- Angina Pectoris Care PlanDocument18 pagesAngina Pectoris Care Planpslokesha84No ratings yet
- D CS Pneumonia BBDocument25 pagesD CS Pneumonia BBKshayna 1234No ratings yet
- CASE PresentationsDocument8 pagesCASE Presentationsanimesh pandaNo ratings yet
- PPCM TamiaDocument17 pagesPPCM TamiaFAIRUZ RIFANINo ratings yet
- 5.case Presentation On Puerperial SepsisDocument38 pages5.case Presentation On Puerperial SepsisAngela Jolhnem Langhu92% (24)
- Case Presentation On COPD FinalDocument26 pagesCase Presentation On COPD FinalShivani TiwariNo ratings yet
- An Easy Guide To Head To Toe Assessment Vrtis 2011-1 PDFDocument6 pagesAn Easy Guide To Head To Toe Assessment Vrtis 2011-1 PDFkatherine dayagNo ratings yet
- Pe FormatDocument12 pagesPe FormatsanthiyasandyNo ratings yet
- Manual of Clinical PharmacyDocument8 pagesManual of Clinical PharmacyMohsinRazaNo ratings yet
- Laporan Kasus Gizi BurukDocument20 pagesLaporan Kasus Gizi Burukwima_putraNo ratings yet
- Nursing Careplan For TofDocument17 pagesNursing Careplan For Tofanamika sharmaNo ratings yet
- Case Presentation: S. Suchitra 3 Year MBBS MVJ Medical College and Research HospitalDocument23 pagesCase Presentation: S. Suchitra 3 Year MBBS MVJ Medical College and Research Hospitalwarkhungam khumlo100% (1)
- Demam Tifoid: Case ReportDocument38 pagesDemam Tifoid: Case ReportMelita Aditya SariNo ratings yet
- Mid A AssignmentDocument24 pagesMid A AssignmentTHE HOWDAY COMPANYNo ratings yet
- Date and Time: June 23, 2018, 3PM Chief Complaint: Difficulty of Breathing History of Present IllnessDocument3 pagesDate and Time: June 23, 2018, 3PM Chief Complaint: Difficulty of Breathing History of Present IllnessConcepcion R. AquinoNo ratings yet
- Acs CASE STUDYDocument25 pagesAcs CASE STUDYarchana verma100% (3)
- MedSurg Careplan 041311 ReformattedDocument13 pagesMedSurg Careplan 041311 ReformattedCaleb LeGearNo ratings yet
- Patient Assessment 1 NSTEMIDocument7 pagesPatient Assessment 1 NSTEMInjoodNo ratings yet
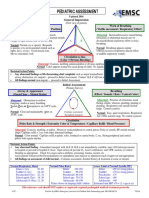
- Pediatric Assessment: General ImpressionDocument2 pagesPediatric Assessment: General ImpressionAghnia Nafila100% (1)
- Asma CaseDocument42 pagesAsma CasenadienNo ratings yet
- برزنتيشن القيادة في التمريضDocument19 pagesبرزنتيشن القيادة في التمريضSima SaeedNo ratings yet
- Seminar Information SimaDocument20 pagesSeminar Information SimaSima SaeedNo ratings yet
- Seminar Sima Saeed ابحاثDocument16 pagesSeminar Sima Saeed ابحاثSima SaeedNo ratings yet
- سيمينار بالغينDocument20 pagesسيمينار بالغينSima SaeedNo ratings yet
- Geriatric Nursing Care Plan Case DetailsDocument16 pagesGeriatric Nursing Care Plan Case DetailsSima SaeedNo ratings yet
- بعد التعديل 2Document16 pagesبعد التعديل 2Sima SaeedNo ratings yet
- Assignment Adults SimaDocument19 pagesAssignment Adults SimaSima SaeedNo ratings yet
- Seminar Sima Saeed ابحاثDocument16 pagesSeminar Sima Saeed ابحاثSima SaeedNo ratings yet
- Nursing Care Plan: STUDENT NAME Bisha UniversityDocument3 pagesNursing Care Plan: STUDENT NAME Bisha UniversitySima SaeedNo ratings yet
- Seminar Sima Saeed ابحاثDocument16 pagesSeminar Sima Saeed ابحاثSima SaeedNo ratings yet
- سيمينار مسنين 2Document18 pagesسيمينار مسنين 2Sima SaeedNo ratings yet
- سيمينار مسنين 2Document18 pagesسيمينار مسنين 2Sima SaeedNo ratings yet
- Assignment Adults SimaDocument19 pagesAssignment Adults SimaSima SaeedNo ratings yet
- Assignment Adults SimaDocument19 pagesAssignment Adults SimaSima SaeedNo ratings yet
- Seminar Sima Saeed ابحاثDocument16 pagesSeminar Sima Saeed ابحاثSima SaeedNo ratings yet
- blackboared activity عملى لبالغين اساسى - 2Document2 pages blackboared activity عملى لبالغين اساسى - 2Sima SaeedNo ratings yet
- سيمينار مسنين 2Document18 pagesسيمينار مسنين 2Sima SaeedNo ratings yet
- Case No:3:: Sima SaeedDocument7 pagesCase No:3:: Sima SaeedSima SaeedNo ratings yet
- Geriatric Nursing Care Plan Case DetailsDocument16 pagesGeriatric Nursing Care Plan Case DetailsSima SaeedNo ratings yet
- SENIOR FIRST BROCHURE - Draft v7 - ProductsDocument6 pagesSENIOR FIRST BROCHURE - Draft v7 - ProductsTrinetra AgarwalNo ratings yet
- Le Fort II Osteotomy and Modified Technique Presentation: Riginal RticleDocument6 pagesLe Fort II Osteotomy and Modified Technique Presentation: Riginal RticleSamuel SuazaNo ratings yet
- Measuring Basic Observations: OSCE ChecklistDocument2 pagesMeasuring Basic Observations: OSCE Checklistahmad50% (4)
- Sexual and Reproductive Health and RightsDocument21 pagesSexual and Reproductive Health and RightsEmmanuelNo ratings yet
- EWMA Endorsements of Wound Centres Non Hospital Based ApplicationForm WordDocument17 pagesEWMA Endorsements of Wound Centres Non Hospital Based ApplicationForm WordCarlo BalzereitNo ratings yet
- ER-1-94-Policy-Briefing PresentationDocument48 pagesER-1-94-Policy-Briefing PresentationJim Boy P RonquilloNo ratings yet
- Adrenal Glands: Crishkey Cuario Nathaniel Estipona Mario Revillosa Jopay ContrerasDocument8 pagesAdrenal Glands: Crishkey Cuario Nathaniel Estipona Mario Revillosa Jopay ContrerasKathlene BalicoNo ratings yet
- Dettmer & Boyer SuitDocument25 pagesDettmer & Boyer SuitBenjamin DuerNo ratings yet
- Plummer 2021Document6 pagesPlummer 2021Cristina CostaNo ratings yet
- The Bidirectional Movement of The Frontalis Muscle: Introducing The Line of Convergence and Its Potential Clinical RelevanceDocument8 pagesThe Bidirectional Movement of The Frontalis Muscle: Introducing The Line of Convergence and Its Potential Clinical RelevanceBruna RochaNo ratings yet
- About Palliative Care in India: Karunashraya - A Case StudyDocument4 pagesAbout Palliative Care in India: Karunashraya - A Case StudySayak ChakrabortyNo ratings yet
- Cigna Close Care Plan Sales Brochure DTC FinalDocument28 pagesCigna Close Care Plan Sales Brochure DTC FinalpriyankaNo ratings yet
- Kinder Endline 2019 2020 T.jen T. MarvinDocument17 pagesKinder Endline 2019 2020 T.jen T. MarvinJenRomarateCervantesNo ratings yet
- Acute Decompensated Heart Failure Topic Discussion HandoutDocument4 pagesAcute Decompensated Heart Failure Topic Discussion Handoutapi-641524095No ratings yet
- Secondary - Report Card Comment CodesDocument2 pagesSecondary - Report Card Comment CodesRICHARD SARDON LEONNo ratings yet
- Es Compleat Coolant Eg Premix - MSDS - Lt16587aDocument6 pagesEs Compleat Coolant Eg Premix - MSDS - Lt16587aCesar G.No ratings yet
- Miller Big Blue 400d and 500x Deutz Part ADocument98 pagesMiller Big Blue 400d and 500x Deutz Part ALUIS ALFREDO SIERRA JUAREZ0% (1)
- Admin,+8Document9 pagesAdmin,+8Dewi RatnasariNo ratings yet
- Impromptu SpeechesDocument3 pagesImpromptu SpeechesAyvie ChweNo ratings yet
- Form 23 - Motion To Lift Order of DefaultDocument2 pagesForm 23 - Motion To Lift Order of DefaultAnthony Karl FernandezNo ratings yet
- Glow Worm 30-40-50f Boiler InstructionsDocument40 pagesGlow Worm 30-40-50f Boiler InstructionsBandit195850% (2)
- Inclusive Teaching Reflection PaperDocument2 pagesInclusive Teaching Reflection Paperapi-35177809179% (19)
- GUIDELINES FOR INPATIENT DIABETES MANAGEMENT هااامDocument1 pageGUIDELINES FOR INPATIENT DIABETES MANAGEMENT هااامAbu HuzaifaNo ratings yet
- HbA1c CON H - EN - C PDFDocument2 pagesHbA1c CON H - EN - C PDFNonameNo ratings yet
- Comprehensive Barangay Youth Development Plan (Cbydp)Document7 pagesComprehensive Barangay Youth Development Plan (Cbydp)Drena DertoNo ratings yet
- Home Health Education Service: Image Title Description PriceDocument18 pagesHome Health Education Service: Image Title Description PriceK. Banteilang NonglangNo ratings yet
- Hyperthyroidism 1Document34 pagesHyperthyroidism 1mussavir100% (2)
- DUTIES AND FUNCTIONS OF EVERY DEPARTMENT in LguDocument3 pagesDUTIES AND FUNCTIONS OF EVERY DEPARTMENT in LguLgu San Juan Abra100% (3)
- Gastrointestinal System Review QuestionsDocument10 pagesGastrointestinal System Review QuestionsSiena PlacinoNo ratings yet
- Principles of Adult Learning DocumentDocument41 pagesPrinciples of Adult Learning Documentحشيمة الروحNo ratings yet