You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Science 10 Quarter 3 Module 1 (Week 1-2)Document24 pagesA Science 10 Quarter 3 Module 1 (Week 1-2)Daisy Soriano Prestoza100% (3)
- Lesson 2 - Reproductive and Sexual HealthDocument3 pagesLesson 2 - Reproductive and Sexual HealthA CNo ratings yet
- UTS MKK Perpustakaan TI - Penelusuran Literatur - Theodore Gabriel (197041223)Document16 pagesUTS MKK Perpustakaan TI - Penelusuran Literatur - Theodore Gabriel (197041223)atikha apriliaNo ratings yet
- UTS MKK Perpustakaan TI - Penelusuran Literatur - Theodore Gabriel (197041223)Document16 pagesUTS MKK Perpustakaan TI - Penelusuran Literatur - Theodore Gabriel (197041223)atikha apriliaNo ratings yet
- ISUOG Practice Guidelines Intrapartum UltrasoundDocument13 pagesISUOG Practice Guidelines Intrapartum UltrasoundAmin-Florin El-KharoubiNo ratings yet
- Each Trimester Stratified Vitamin D SupplementationDocument17 pagesEach Trimester Stratified Vitamin D Supplementationatikha apriliaNo ratings yet
- Intrapartum Assesment BJADocument6 pagesIntrapartum Assesment BJAatikha apriliaNo ratings yet
- Interactions Between Human Plasma Sex Hormone-Binding Globulin and Xenobiotic LigandsDocument10 pagesInteractions Between Human Plasma Sex Hormone-Binding Globulin and Xenobiotic Ligandsatikha apriliaNo ratings yet
- Maternal Sleep PracticesDocument11 pagesMaternal Sleep Practicesatikha apriliaNo ratings yet
- MR 25Document13 pagesMR 25atikha apriliaNo ratings yet
- 13 2 261 PDFDocument16 pages13 2 261 PDFLuis YzerikNo ratings yet
- Maternal Vitamin D Supplementation During PregnancyDocument30 pagesMaternal Vitamin D Supplementation During Pregnancyatikha apriliaNo ratings yet
- Vitamin D Supplementation in PregnancyDocument5 pagesVitamin D Supplementation in Pregnancyatikha apriliaNo ratings yet
- Last Trimester Vitamin DDocument6 pagesLast Trimester Vitamin Datikha apriliaNo ratings yet
- Stuart 2011Document6 pagesStuart 2011atikha apriliaNo ratings yet
- Maternal and Perinatal Outcome in Vitamin D Status (Systematic Review)Document13 pagesMaternal and Perinatal Outcome in Vitamin D Status (Systematic Review)atikha apriliaNo ratings yet
- Ginek WARD 17 Februari 2020Document75 pagesGinek WARD 17 Februari 2020atikha apriliaNo ratings yet
- Bregar 1Document7 pagesBregar 1atikha apriliaNo ratings yet
- Selle2015 PDFDocument12 pagesSelle2015 PDFatikha apriliaNo ratings yet
- Ournal of Linical Ncology: Review ArticleDocument12 pagesOurnal of Linical Ncology: Review Articleatikha apriliaNo ratings yet
- Oup Accepted Manuscript 2017 PDFDocument8 pagesOup Accepted Manuscript 2017 PDFatikha apriliaNo ratings yet
- Germ Cell Tumors Ovarium: Poppy M. LintongDocument12 pagesGerm Cell Tumors Ovarium: Poppy M. Lintongvytania oktariNo ratings yet
- First-Line Gemcitabine and Carboplatin in Advanced Ovarian Carcinoma: A Phase II StudyDocument5 pagesFirst-Line Gemcitabine and Carboplatin in Advanced Ovarian Carcinoma: A Phase II Studyatikha apriliaNo ratings yet
- Cancers: Therapeutic Challenges For Cisplatin-Resistant Ovarian Germ Cell TumorsDocument14 pagesCancers: Therapeutic Challenges For Cisplatin-Resistant Ovarian Germ Cell Tumorsatikha apriliaNo ratings yet
- Vazquez2013 PDFDocument7 pagesVazquez2013 PDFatikha apriliaNo ratings yet
- Gynecologic Oncology Reports: Case ReportDocument3 pagesGynecologic Oncology Reports: Case Reportatikha apriliaNo ratings yet
- Newton 2019Document9 pagesNewton 2019atikha apriliaNo ratings yet
- Selle2015 PDFDocument12 pagesSelle2015 PDFatikha apriliaNo ratings yet
- Current Controversies in The Management of Germ Cell Ovarian TumoursDocument7 pagesCurrent Controversies in The Management of Germ Cell Ovarian Tumoursatikha apriliaNo ratings yet
- Lecture 3Document7 pagesLecture 3Helin BadikanlıNo ratings yet
- UntitledDocument8 pagesUntitledAman KhanNo ratings yet
- Normal Deliveries FormDocument15 pagesNormal Deliveries FormRona Mae PangilinanNo ratings yet
- DLL - Science 5 - Q2 - W3Document5 pagesDLL - Science 5 - Q2 - W3Mc Paul John LiberatoNo ratings yet
- Angie Writen ReportDocument3 pagesAngie Writen ReportJhunard Christian O. AsayasNo ratings yet
- PDF Character Achievements Guide - CompressDocument16 pagesPDF Character Achievements Guide - CompressKaiji KuroganeNo ratings yet
- V07ovq2lq3r31.jpg 922×1.344 PixelsDocument1 pageV07ovq2lq3r31.jpg 922×1.344 Pixelsილ იაNo ratings yet
- JDH Leonard Manso 416-1Document3 pagesJDH Leonard Manso 416-1Ramiro CarrilloNo ratings yet
- Infomercial Draft Script (Lapasaran, Norie Jean G.)Document5 pagesInfomercial Draft Script (Lapasaran, Norie Jean G.)xxxx100% (3)
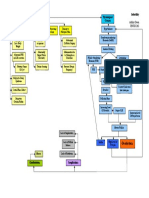
- Infertility Concept MapDocument1 pageInfertility Concept Mapashleydean0% (1)
- Anatomy Lab. (2) - WorksheetsDocument8 pagesAnatomy Lab. (2) - WorksheetsHamzeh SandoukaNo ratings yet
- OBGYN II Important QsDocument10 pagesOBGYN II Important QsDwivith ReddyNo ratings yet
- Hmole Case ReviewDocument5 pagesHmole Case ReviewJonalyn EtongNo ratings yet
- Constitution of An Individual's SexDocument41 pagesConstitution of An Individual's SexBench FuentesNo ratings yet
- In-Vitro Fertilisation: Shruti Samal ROLL NUMBER - 1120096 B.Sc. Life Science Second SemesterDocument20 pagesIn-Vitro Fertilisation: Shruti Samal ROLL NUMBER - 1120096 B.Sc. Life Science Second SemesterSHRUTI SAMALNo ratings yet
- Bad Obstetrical HistoryDocument34 pagesBad Obstetrical HistorySagung Ayuska GandhariNo ratings yet
- College Final Paper 2-6-1Document6 pagesCollege Final Paper 2-6-1Rita MoraaNo ratings yet
- Persuasive Speech PresentationDocument13 pagesPersuasive Speech Presentationapi-670902898No ratings yet
- Chapter 28 Paternity and Filiation On NonDocument4 pagesChapter 28 Paternity and Filiation On NonWang BeauNo ratings yet
- Abala Lab Ex 5Document6 pagesAbala Lab Ex 5a19-1-00227No ratings yet
- The Process of ConceptionDocument15 pagesThe Process of ConceptionJobelyn Dela CruzNo ratings yet
- SEX EDUCATIOscript UnfinishDocument11 pagesSEX EDUCATIOscript UnfinishSITI NURRAUDAH BINTI RAFIZ (BG)100% (1)
- Form 5 HSB Session 9-12Document83 pagesForm 5 HSB Session 9-12Alysha NeilsNo ratings yet
- Animal Science TermsDocument6 pagesAnimal Science Termsalexenneth canilaNo ratings yet
- Nightmaretaker GuideDocument12 pagesNightmaretaker Guidejese 08No ratings yet
- Gr5 Lp4 Reproduction English FinalDocument27 pagesGr5 Lp4 Reproduction English FinalDiana Minandig BalunoNo ratings yet
- BAB II SewaDocument33 pagesBAB II SewaShelina ANo ratings yet
- Family Planning For Clients With Special Needss BIDocument34 pagesFamily Planning For Clients With Special Needss BIBerhanu EjaraNo ratings yet