You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Cause and Prevention of CancerDocument11 pagesThe Cause and Prevention of CancerJoseph SabidoNo ratings yet
- Type B Blood GroupDocument14 pagesType B Blood Groupv.daniel03111No ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Session11-Premalignant Lesions of The Cervix, CX CADocument68 pagesSession11-Premalignant Lesions of The Cervix, CX CACHALIE MEQU100% (2)
- MSM and DMSO Organic Sulphur As A Versatile HealerDocument8 pagesMSM and DMSO Organic Sulphur As A Versatile HealerKata KataNo ratings yet
- What Is Breast CancerDocument24 pagesWhat Is Breast CancerKheny Amira RisaNo ratings yet
- AAOS Oncology (50 Soal)Document18 pagesAAOS Oncology (50 Soal)Fasa RoshadaNo ratings yet
- Ecl Tételek B2 JavítottDocument18 pagesEcl Tételek B2 Javítottdobani100% (3)
- Nutrition Management CancerDocument5 pagesNutrition Management CancerkitsilcNo ratings yet
- How Much and What Type of Protein Should A Critically Ill Patient Receive?Document9 pagesHow Much and What Type of Protein Should A Critically Ill Patient Receive?Ayip Bahsan AlBantaniNo ratings yet
- Effect of Dietary Omega-3 Fatty Acid Supplementation On Frailty-Related Phenotypes in Older Adults: A Systematic Review and Meta-Analysis ProtocolDocument5 pagesEffect of Dietary Omega-3 Fatty Acid Supplementation On Frailty-Related Phenotypes in Older Adults: A Systematic Review and Meta-Analysis ProtocolAyip Bahsan AlBantaniNo ratings yet
- Curroncol 28 00293Document10 pagesCurroncol 28 00293Ayip Bahsan AlBantaniNo ratings yet
- en Papilla Vaters Tumor in Elderly An InterDocument5 pagesen Papilla Vaters Tumor in Elderly An InterAyip Bahsan AlBantaniNo ratings yet
- Pathophysiology Patient's DataDocument3 pagesPathophysiology Patient's DataKristian Karl Bautista Kiw-isNo ratings yet
- NCBP2 and TFRC Are Novel Prognostic Biomarkers in Oral Squamous Cell CarcinomaDocument14 pagesNCBP2 and TFRC Are Novel Prognostic Biomarkers in Oral Squamous Cell CarcinomaEtika SukmawatiNo ratings yet
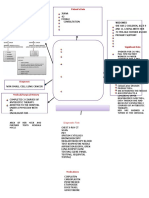
- Acute Renal Failure DiagramDocument3 pagesAcute Renal Failure DiagramMichelle BarojaNo ratings yet
- ThyroidDocument102 pagesThyroidfadoNo ratings yet
- Patients With Anaplastic Thyroid CancerDocument45 pagesPatients With Anaplastic Thyroid Cancerfanny_febrianiNo ratings yet
- Reports 1Document1 pageReports 1ziauddin2No ratings yet
- Case Series of Rare Breast Diseases and Their Unusual PresentationDocument36 pagesCase Series of Rare Breast Diseases and Their Unusual Presentationdodo1No ratings yet
- AutoGenomics Intl-AACC, LADocument63 pagesAutoGenomics Intl-AACC, LAmohdkhairNo ratings yet
- PDF 20220916 142849 0000-1Document20 pagesPDF 20220916 142849 0000-1Darman SyahNo ratings yet
- Category Specifics Comments: Bethesda Classification of Cervical CytologyDocument2 pagesCategory Specifics Comments: Bethesda Classification of Cervical Cytologysaad awanNo ratings yet
- Wilms TumourDocument3 pagesWilms TumourfifahcantikNo ratings yet
- Treatment of Iron Deficiency Anemia in Adults - UpToDateDocument82 pagesTreatment of Iron Deficiency Anemia in Adults - UpToDateSantiago MayorNo ratings yet
- NSTP 011 Module 7 - 12Document31 pagesNSTP 011 Module 7 - 12Michael Jack SalvadorNo ratings yet
- Taurox Anti Fatigue InformationDocument5 pagesTaurox Anti Fatigue Informationsyfi56No ratings yet
- Spirulina, Accepted ArticleDocument7 pagesSpirulina, Accepted Articlebbrabadiya6652No ratings yet
- PSA Level and Gleason Score in Predicting The Stage of Newly Diagnosed Prostat CancerDocument6 pagesPSA Level and Gleason Score in Predicting The Stage of Newly Diagnosed Prostat CancergumNo ratings yet
- Chapter 5 - Autosuggestion - Think and Grow Rich - The 21st-Century Edition (Workbook)Document33 pagesChapter 5 - Autosuggestion - Think and Grow Rich - The 21st-Century Edition (Workbook)Naveed AhmedNo ratings yet
- Uterine SarcomaDocument44 pagesUterine SarcomajojolilimomoNo ratings yet
- Paragraph Jumbles (40 Questions)Document11 pagesParagraph Jumbles (40 Questions)nishant410No ratings yet
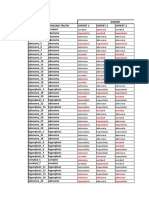
- Expert Lesion Ground Truth Expert 1 Expert 2 Expert 3Document10 pagesExpert Lesion Ground Truth Expert 1 Expert 2 Expert 3SSN VISHNUNo ratings yet
- Go Wyoming (Fall 2023)Document32 pagesGo Wyoming (Fall 2023)The Livingston County NewsNo ratings yet
- AdenomaDocument4 pagesAdenomaPark JiminNo ratings yet