You might also like
- Alim 3 Keracunan ParaquatDocument22 pagesAlim 3 Keracunan ParaquatMuhamad sairul azhar bin yaNo ratings yet
- Renal Function TestsDocument28 pagesRenal Function TestsdoctoroidNo ratings yet
- Commonly Used Chemotherapy Drugs: MedicationsDocument6 pagesCommonly Used Chemotherapy Drugs: MedicationsAndra Elena PricopNo ratings yet
- Ind. Sem. - ALL OncasparDocument40 pagesInd. Sem. - ALL OncasparBrianhernzNo ratings yet
- Dosis Obat LengkapDocument52 pagesDosis Obat LengkapropusanNo ratings yet
- Cattle Uterine ProlapseDocument3 pagesCattle Uterine ProlapseElena M. TilibaşaNo ratings yet
- Prog-Vak + BLSA B.100 JCI PBD Update 8 Juni 2023Document15 pagesProg-Vak + BLSA B.100 JCI PBD Update 8 Juni 2023Abdillah MuttaqiinNo ratings yet
- Drug ListDocument8 pagesDrug ListpeachandmintsNo ratings yet
- VMD-Livestock-pharma Product-List 140bx240mm EN July 2020 Web-VersionDocument14 pagesVMD-Livestock-pharma Product-List 140bx240mm EN July 2020 Web-VersionMas MeidiNo ratings yet
- Haemin Crystals LabDocument6 pagesHaemin Crystals LabNaiomiNo ratings yet
- 4 Diabetes MellitusDocument26 pages4 Diabetes MellitusnomiskemalNo ratings yet
- ELISA For Measuring Bovine PregnancyDocument5 pagesELISA For Measuring Bovine PregnancyMaría Alejandra Ayanegui AlcérrecaNo ratings yet
- Assay For Uronic Acid Carbazole Reaction PDFDocument3 pagesAssay For Uronic Acid Carbazole Reaction PDFph_swordman0% (1)
- Rangkuman ObatDocument8 pagesRangkuman ObatqlephonNo ratings yet
- 1st Lecture of Respiratory Histology by DR RoomiDocument24 pages1st Lecture of Respiratory Histology by DR RoomiMudassar Roomi100% (1)
- Weakness & Exercise Intolerance in A DogDocument4 pagesWeakness & Exercise Intolerance in A DogMonica CusniriucNo ratings yet
- Presented By-: Dr. Prabhata Kumar Parida ADM - No. 06ARGO/13Document19 pagesPresented By-: Dr. Prabhata Kumar Parida ADM - No. 06ARGO/13Krushna krupa PradhanNo ratings yet
- Pregnancy TestDocument10 pagesPregnancy TestquerokeropiNo ratings yet
- Vaccination: Dairy Hub Training Booklets TitlesDocument8 pagesVaccination: Dairy Hub Training Booklets TitlesQais KaisraniNo ratings yet
- Spintrol "H" CAL: Human Serum / Suero HumanoDocument4 pagesSpintrol "H" CAL: Human Serum / Suero HumanoMD ALAMINNo ratings yet
- Jeopardy Game NPB 101LDocument51 pagesJeopardy Game NPB 101Lkkk13whyNo ratings yet
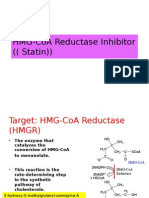
- HMG-CoA Reductase InhibitorDocument10 pagesHMG-CoA Reductase InhibitorGilang Sumiarsih PramanikNo ratings yet
- general systemic states د.عزيزةDocument75 pagesgeneral systemic states د.عزيزةAhmed Hamdy NaDa100% (2)
- Carnitine Shuttle: DR - Rijha AhmedDocument12 pagesCarnitine Shuttle: DR - Rijha AhmedSafura IjazNo ratings yet
- Lohmann Brown Classic Management Guide for Colony SystemsDocument25 pagesLohmann Brown Classic Management Guide for Colony Systemsionut2007No ratings yet
- Blood Collection in SwineDocument4 pagesBlood Collection in Swineelvhynd beiNo ratings yet
- 7.formulation and Evaluation of Lycopene Emulgel PDFDocument15 pages7.formulation and Evaluation of Lycopene Emulgel PDFYuppie RajNo ratings yet
- AtropineDocument4 pagesAtropinePark EyzNo ratings yet
- AOE - Hiral Labs LTD Company Brochure 20180416170521Document20 pagesAOE - Hiral Labs LTD Company Brochure 20180416170521Dr VENKAT1 LUNo ratings yet
- Public Health ImportanceDocument6 pagesPublic Health ImportanceHarshal SabaneNo ratings yet
- SPC SoludoxDocument19 pagesSPC SoludoxMihai BirsaNo ratings yet
- Pediatric DosesDocument20 pagesPediatric Doseshamadadodo550% (2)
- 2017 - Efficacy of Cysteamine Cream in The Treatment of Epidermal Melasma, Evaluating by Dermacatch As A New Measurement Method. A Randomized Double Blind Placebo Controlled Study.Document9 pages2017 - Efficacy of Cysteamine Cream in The Treatment of Epidermal Melasma, Evaluating by Dermacatch As A New Measurement Method. A Randomized Double Blind Placebo Controlled Study.Adriana GomesNo ratings yet
- Contraceptivemethods 150521003728 Lva1 App6892Document59 pagesContraceptivemethods 150521003728 Lva1 App6892Michael John Anicas LozanoNo ratings yet
- Drug Formulary For Primates and Primate SanctuariesDocument20 pagesDrug Formulary For Primates and Primate SanctuariesMel Cid IIINo ratings yet
- TerrexineDocument5 pagesTerrexineWakhidatus InryaNo ratings yet
- Immunolocalization of Aquaporin-5 Expression in Sweat Gland Cells From Normal and Anhidrotic Horses (Pages 17-23)Document7 pagesImmunolocalization of Aquaporin-5 Expression in Sweat Gland Cells From Normal and Anhidrotic Horses (Pages 17-23)jenNo ratings yet
- Causes of Bleeding in Cows After OvulationDocument10 pagesCauses of Bleeding in Cows After OvulationmortezahNo ratings yet
- AkiDocument13 pagesAkiharshe v100% (1)
- Product ListDocument33 pagesProduct ListMehul JaniNo ratings yet
- S.N o Name of Drug Recommended Paediatrics Dose Strength 1.: CPM - 2 mg/5mlDocument3 pagesS.N o Name of Drug Recommended Paediatrics Dose Strength 1.: CPM - 2 mg/5mlmrs raamNo ratings yet
- TOCOLYSIS IN VETERINARY REPRODUCTION-By:-Dr. DHIREN BHOIDocument47 pagesTOCOLYSIS IN VETERINARY REPRODUCTION-By:-Dr. DHIREN BHOIdrdhirenvet100% (2)
- Imidocarb Summary Report 2 Committee Veterinary Medicinal Products enDocument6 pagesImidocarb Summary Report 2 Committee Veterinary Medicinal Products enGilsson FigueroaNo ratings yet
- IMIDOCARPDocument3 pagesIMIDOCARPAna Paola ZFNo ratings yet
- Committee For Veterinary Medicinal ProductsDocument5 pagesCommittee For Veterinary Medicinal ProductswisievekNo ratings yet
- Avilamycin Summary Report Committee Veterinary Medicinal Products - enDocument9 pagesAvilamycin Summary Report Committee Veterinary Medicinal Products - enPiñita PillinaNo ratings yet
- Emea 2004Document7 pagesEmea 2004andreililioanceaNo ratings yet
- Metamizole Summary Report 2 Committee Veterinary Medicinal Products enDocument10 pagesMetamizole Summary Report 2 Committee Veterinary Medicinal Products enReni Ika CahyantiNo ratings yet
- Fenpipramide Hydrochloride Summary Report Committee Veterinary Medicinal Products - en PDFDocument2 pagesFenpipramide Hydrochloride Summary Report Committee Veterinary Medicinal Products - en PDFAdriana TrandafirNo ratings yet
- Aac00370 0083Document6 pagesAac00370 0083Caustic ToxicNo ratings yet
- TNMH42010 RFAntibioticresiduesDocument1 pageTNMH42010 RFAntibioticresiduesDiana CurchiNo ratings yet
- Capsici FructusDocument4 pagesCapsici FructusRiyas AfdalNo ratings yet
- Committee For Veterinary Medicinal Products: Summary ReportDocument9 pagesCommittee For Veterinary Medicinal Products: Summary ReportNatasha ImanuelleNo ratings yet
- Paracetamol Summary Report Committee Veterinary Medicinal Products - enDocument6 pagesParacetamol Summary Report Committee Veterinary Medicinal Products - entambreen18No ratings yet
- Ibuprofen Toxicosis in Dogs, Cats, and Ferrets: Toxicology BriefDocument4 pagesIbuprofen Toxicosis in Dogs, Cats, and Ferrets: Toxicology BriefChan TawasilNo ratings yet
- Committee For Veterinary Medicinal Products: (Extension To All Food Producing Species)Document2 pagesCommittee For Veterinary Medicinal Products: (Extension To All Food Producing Species)Gialuu NguyenNo ratings yet
- Estensuin To Eggs WC500015766Document3 pagesEstensuin To Eggs WC500015766papaindoNo ratings yet
- Eucalyptus Globulus (Eucalyptus) - Derived Ingredients: Safety Assessment of As Used in CosmeticsDocument49 pagesEucalyptus Globulus (Eucalyptus) - Derived Ingredients: Safety Assessment of As Used in CosmeticsNelson Carballo VelazquezNo ratings yet
- Baytril Safety and ToxicologyDocument6 pagesBaytril Safety and ToxicologymarcioNo ratings yet
- Committee For Veterinary Medicinal ProductsDocument7 pagesCommittee For Veterinary Medicinal Productsvetma1No ratings yet
- Rt-01-Iuran Bulanan Warga Aktif - 15-11-2023Document2 pagesRt-01-Iuran Bulanan Warga Aktif - 15-11-2023ilhamNo ratings yet
- Timing of InseminationDocument2 pagesTiming of InseminationilhamNo ratings yet
- Calf diarrhoea: focus on hydrationDocument2 pagesCalf diarrhoea: focus on hydrationilhamNo ratings yet
- Effects of Dexamethasone On Progesterone and Estrogen Profiles and Uterine Progesterone Receptor Localization During Pregnancy in Sahel Goat in Semi-Arid RegionDocument7 pagesEffects of Dexamethasone On Progesterone and Estrogen Profiles and Uterine Progesterone Receptor Localization During Pregnancy in Sahel Goat in Semi-Arid RegionilhamNo ratings yet
- Invoice Maxim-562Document1 pageInvoice Maxim-562ilhamNo ratings yet
- CR 296Document8 pagesCR 296Noora Ari Sandy AmbarwatiNo ratings yet
- Aphthae EpizooticaDocument29 pagesAphthae EpizooticaSitiNurmaYunita100% (1)
- Feline MegacolonDocument12 pagesFeline MegacolonilhamNo ratings yet
- PenelitianDocument9 pagesPenelitianilhamNo ratings yet
- PenelitianDocument9 pagesPenelitianilhamNo ratings yet
- Fixs LampDocument1 pageFixs LampilhamNo ratings yet
- Effect of prostaglandin hormone synchronization methods on estrus percentage and pregnancy rates in beef cattleDocument6 pagesEffect of prostaglandin hormone synchronization methods on estrus percentage and pregnancy rates in beef cattleilhamNo ratings yet
- 01.jurnal Acara 1Document5 pages01.jurnal Acara 1sarwiyahNo ratings yet
- Jurnal AyamsssDocument8 pagesJurnal AyamsssilhamNo ratings yet
- Daftar PustakaDocument1 pageDaftar PustakailhamNo ratings yet
- B 070203Document8 pagesB 070203Biodiversitas, etc100% (1)
- Josamycin Propionate and Kanamycin Monosulfate AntibioticsDocument471 pagesJosamycin Propionate and Kanamycin Monosulfate AntibioticsGopalaKrishnan SivaramanNo ratings yet
- Bio Lab Report 2Document4 pagesBio Lab Report 2api-253660813No ratings yet
- Mycobacterium Abscessus: A New Antibiotic NightmareDocument9 pagesMycobacterium Abscessus: A New Antibiotic NightmareHootNo ratings yet
- Aminoglycoside Antibiotics in Infectious Diseases. An Overview PDFDocument13 pagesAminoglycoside Antibiotics in Infectious Diseases. An Overview PDFjoadascouvesNo ratings yet
- Kanamycin Summary Report 2 Committee Veterinary Medicinal Products - enDocument9 pagesKanamycin Summary Report 2 Committee Veterinary Medicinal Products - enilhamNo ratings yet
- ATUM (Rhamnosa E.coli)Document4 pagesATUM (Rhamnosa E.coli)Ruth MichelleeNo ratings yet
- Answer Key For AP Biology Practice Exam, Section IDocument13 pagesAnswer Key For AP Biology Practice Exam, Section Ibao'E yourfatherNo ratings yet
- Classification of AntibioticsDocument4 pagesClassification of AntibioticsNico AvellanaNo ratings yet
- AminoglycosidesDocument28 pagesAminoglycosidesKhalid MehmoodNo ratings yet
- TerrexineDocument5 pagesTerrexineWakhidatus InryaNo ratings yet
- Assessment and Determination of Optimum Concentration of Streptomycin and Kanamycin As Selective Agents in Peppermint (MenthaDocument6 pagesAssessment and Determination of Optimum Concentration of Streptomycin and Kanamycin As Selective Agents in Peppermint (MenthaMonaia YehiaNo ratings yet
- Antibiotic Resistance Lab ConclusionDocument2 pagesAntibiotic Resistance Lab ConclusionNathan Hise100% (1)
- Freedom Cho S Kit ManDocument72 pagesFreedom Cho S Kit ManDhanya ValaveetilNo ratings yet
- AminoglycosidesDocument6 pagesAminoglycosidesLlosa JuneNo ratings yet
- Bio Lab Ex 10Document2 pagesBio Lab Ex 10juanNo ratings yet
- Oedogonium capillare alga reduces bacterial load of Tubifex tubifexDocument10 pagesOedogonium capillare alga reduces bacterial load of Tubifex tubifexAlvaro Diego CastilloNo ratings yet
- Medicinal Chemistry of Aminoglycoside AntibioticsDocument31 pagesMedicinal Chemistry of Aminoglycoside AntibioticsKevin Chapley100% (3)
- Lisozim Udang PDFDocument6 pagesLisozim Udang PDFDendi HidayatullahNo ratings yet
- Antibiotic working concentrations catalog numbersDocument1 pageAntibiotic working concentrations catalog numbersBodhi DharmaNo ratings yet
- CHN DrugstudyDocument2 pagesCHN DrugstudyNathalie OmalNo ratings yet
- What Are AntibioticsDocument31 pagesWhat Are Antibiotics1211988610No ratings yet
- An Efficient Agrobacterium-Mediated Transformation Protocol for Black PepperDocument8 pagesAn Efficient Agrobacterium-Mediated Transformation Protocol for Black PepperIman Fadhul HadiNo ratings yet