You might also like
- Hirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Abdominal Trauma Signs, Symptoms and Nursing CareDocument24 pagesAbdominal Trauma Signs, Symptoms and Nursing CareSurgeryClassesNo ratings yet
- Anatomy and Physiology With Pathophysiology TransesDocument10 pagesAnatomy and Physiology With Pathophysiology Transeshezekiah minNo ratings yet
- Cestodes 2020Document10 pagesCestodes 2020CDNo ratings yet
- HistopathDocument7 pagesHistopathDixie DumagpiNo ratings yet
- Cranial NerveDocument4 pagesCranial NerveBrian OballoNo ratings yet
- Nursing Case Study Chronic CholecystitisDocument22 pagesNursing Case Study Chronic CholecystitisShairalyn Catada100% (1)
- Urinary SystemDocument9 pagesUrinary SystemCUESCANO, CRISTEL G. BSMT 2-ANo ratings yet
- The Endocrine System: Part BDocument38 pagesThe Endocrine System: Part BKaly Rie100% (1)
- REV Micro HSB RemedsDocument16 pagesREV Micro HSB RemedsPatricia HariramaniNo ratings yet
- Fundamentals of Nursing ReviewerDocument9 pagesFundamentals of Nursing Reviewerchie9268No ratings yet
- Fetal CirculationDocument20 pagesFetal CirculationMuhyeeSalaIdjadNo ratings yet
- Review of Cardiovascular SystemDocument20 pagesReview of Cardiovascular SystemVăn ĐứcNo ratings yet
- SASDocument4 pagesSASNicole Ken AgdanaNo ratings yet
- Physiology & Anatomy Nervous System: MuscleDocument2 pagesPhysiology & Anatomy Nervous System: MuscleEllah GutierrezNo ratings yet
- Breasts and AxillaeDocument10 pagesBreasts and Axillaedlneisha61100% (1)
- Immunologic Disorders ExplainedDocument73 pagesImmunologic Disorders ExplainedDjayNo ratings yet
- 7th-The Alimentary SystemDocument25 pages7th-The Alimentary Systemprasun_v100% (1)
- Physiology of Skeletal Muscle and Muscle FibreDocument7 pagesPhysiology of Skeletal Muscle and Muscle FibreNoor-E-Khadiza ShamaNo ratings yet
- Anatomy and Physiology of The BrainDocument15 pagesAnatomy and Physiology of The BrainFildehl Janice Bomediano CatipayNo ratings yet
- Urinary System Disorders Practice Quiz #1 (50 Questions)Document26 pagesUrinary System Disorders Practice Quiz #1 (50 Questions)Emy TandinganNo ratings yet
- Diseases of Urinary SystemDocument29 pagesDiseases of Urinary SystemHassan.shehri100% (9)
- Normal NewbornAssessmentDocument53 pagesNormal NewbornAssessmentMidori SanNo ratings yet
- QUIZ 8-Gen - PathDocument27 pagesQUIZ 8-Gen - PathDrbee10No ratings yet
- Lecture Outline: See Separate Powerpoint Slides For All Figures and Tables Pre-Inserted Into Powerpoint Without NotesDocument61 pagesLecture Outline: See Separate Powerpoint Slides For All Figures and Tables Pre-Inserted Into Powerpoint Without NotesJharaNo ratings yet
- Case Scenario 3 GerdDocument4 pagesCase Scenario 3 GerdPrincess Faniega SugatonNo ratings yet
- Pharma Unit 1-2 Anti - Adrenergic DrugsDocument21 pagesPharma Unit 1-2 Anti - Adrenergic DrugsMIbrahimNo ratings yet
- ANAPHY Lec Session #5 - SAS (Agdana, Nicole Ken)Document9 pagesANAPHY Lec Session #5 - SAS (Agdana, Nicole Ken)Nicole Ken AgdanaNo ratings yet
- Introduction To Anatomy and PhysiologyDocument36 pagesIntroduction To Anatomy and PhysiologyKenneth Reigne ArguidasNo ratings yet
- Reviewer Anaphy Lec Digestive System 2nd PartDocument6 pagesReviewer Anaphy Lec Digestive System 2nd PartAubrey Gale MendozaNo ratings yet
- Cranial NervesDocument2 pagesCranial Nervesmp_329100% (1)
- St. Luke's College of Medicine - William H. Quasha Memorial: AnatomyDocument4 pagesSt. Luke's College of Medicine - William H. Quasha Memorial: AnatomyMavic VillanuevaNo ratings yet
- Urinary SystemDocument10 pagesUrinary SystemElyka Alivan Valdez PolonioNo ratings yet
- Para Compre 2Document17 pagesPara Compre 2serainie maiNo ratings yet
- Smooth Muscle Contraction MechanismsDocument3 pagesSmooth Muscle Contraction MechanismsMavic VillanuevaNo ratings yet
- Trichuris Trichiura: Lecture By: Maha Gamal AldeinDocument20 pagesTrichuris Trichiura: Lecture By: Maha Gamal AldeinMohammad DweibNo ratings yet
- Study Guide 1 Assessment of Digestive and Gastrointestinal Function and Treatment ModalitiesDocument10 pagesStudy Guide 1 Assessment of Digestive and Gastrointestinal Function and Treatment ModalitiesKc Cabanilla LizardoNo ratings yet
- Seeley 6e 2004 CH 28 Reproductive SystemDocument4 pagesSeeley 6e 2004 CH 28 Reproductive SystemNinoamelia OrikkuNo ratings yet
- Human Skeleton-DlarsonDocument57 pagesHuman Skeleton-Dlarsonapi-308826929No ratings yet
- Understanding key parasitology termsDocument7 pagesUnderstanding key parasitology termsArlene DaroNo ratings yet
- Anatomy and Physiology ReviewerDocument52 pagesAnatomy and Physiology ReviewerCourtney Dela FierraNo ratings yet
- Biochemistry Quiz - Enzymes and Vitamins - Answer KeyDocument8 pagesBiochemistry Quiz - Enzymes and Vitamins - Answer KeyKennethNo ratings yet
- Osce Cranial Nerves PDFDocument42 pagesOsce Cranial Nerves PDFriczen vilaNo ratings yet
- Cell Injury, Inflammation, and Repair ProcessesDocument55 pagesCell Injury, Inflammation, and Repair Processesgabb bbNo ratings yet
- Anatomy of The Heart: Materials Pre-Lab QuizDocument14 pagesAnatomy of The Heart: Materials Pre-Lab QuizAnonymous dRAu54No ratings yet
- Pathophysiology MaiaDocument2 pagesPathophysiology Maiajia88No ratings yet
- Meningeal LayerDocument6 pagesMeningeal LayerKathrice PinedaNo ratings yet
- How the Alimentary Tract Digests and Absorbs NutrientsDocument6 pagesHow the Alimentary Tract Digests and Absorbs NutrientsKC White Dela Rosa100% (1)
- Circulatory SystemDocument4 pagesCirculatory SystemGennelle GabrielNo ratings yet
- DDocument5 pagesDDaeng Arya01No ratings yet
- 7 - Regulation and Functions of The Thyroid HormonesDocument31 pages7 - Regulation and Functions of The Thyroid HormonesVigneshwaran RavishankarNo ratings yet
- 1657541176980-Chpter 16 An Introduction To Management ScienceDocument47 pages1657541176980-Chpter 16 An Introduction To Management ScienceAnushka Kanaujia100% (1)
- Abdominal AbscessDocument3 pagesAbdominal AbscessIchalAzNo ratings yet
- Abdominal Trauma: Fatin Amirah KamaruddinDocument29 pagesAbdominal Trauma: Fatin Amirah Kamaruddinvirz23No ratings yet
- AnaPhy ReproductiveDocument34 pagesAnaPhy ReproductiveTom Sing100% (1)
- Fluids and Electrolytes Management in Surgical PatientsDocument4 pagesFluids and Electrolytes Management in Surgical PatientsJanine Maita BalicaoNo ratings yet
- SGD 4 - Skeletal Muscle PhysiologyDocument3 pagesSGD 4 - Skeletal Muscle PhysiologyKriska Noelle0% (1)
- Surface AnatomyDocument63 pagesSurface AnatomyCodie SimoneauxNo ratings yet
- Skeletal Effects Induced by Maxillary Skeletal Expander (MSE)Document140 pagesSkeletal Effects Induced by Maxillary Skeletal Expander (MSE)DONGXU LIUNo ratings yet
- ALL Ob-Gyn McqsDocument297 pagesALL Ob-Gyn McqsPreeti ChouhanNo ratings yet
- Thyroidectomy: Continuing Education ActivityDocument10 pagesThyroidectomy: Continuing Education Activitybo gum parkNo ratings yet
- Surgical Oncology and Breast BiopsyDocument12 pagesSurgical Oncology and Breast Biopsybo gum parkNo ratings yet
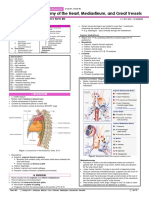
- Mediastinum, and Great VesselsDocument10 pagesMediastinum, and Great Vesselsbo gum parkNo ratings yet
- SGD: Breast Cancer: I. CaseDocument10 pagesSGD: Breast Cancer: I. Casebo gum parkNo ratings yet
- Authors: Section Editor: Deputy EditorDocument37 pagesAuthors: Section Editor: Deputy Editorbo gum parkNo ratings yet
- HyperthyroidismDocument2 pagesHyperthyroidismbo gum parkNo ratings yet
- COPD Diagnostic Criteria and ManagementDocument13 pagesCOPD Diagnostic Criteria and Managementbo gum parkNo ratings yet
- Drugs For COPD: PharmacologyDocument8 pagesDrugs For COPD: Pharmacologybo gum parkNo ratings yet
- Mediastinum, and Great VesselsDocument14 pagesMediastinum, and Great Vesselsbo gum parkNo ratings yet
- Clinical Approach To Patient in ShockDocument10 pagesClinical Approach To Patient in Shockbo gum parkNo ratings yet
- Overview of Hepatic Resection Techniques and IndicationsDocument30 pagesOverview of Hepatic Resection Techniques and Indicationsbo gum parkNo ratings yet
- Anti-TB Drug RegimensDocument8 pagesAnti-TB Drug Regimensbo gum parkNo ratings yet
- Local TreatmentDocument48 pagesLocal Treatmentbo gum parkNo ratings yet
- Surgical management of potentially resectable HCCDocument28 pagesSurgical management of potentially resectable HCCbo gum parkNo ratings yet
- Partial Gastrectomy and Gastrointestinal Reconstruction - UpToDateDocument59 pagesPartial Gastrectomy and Gastrointestinal Reconstruction - UpToDatebo gum parkNo ratings yet
- Surgical ResectionDocument43 pagesSurgical Resectionbo gum parkNo ratings yet
- Staging of Colorectal CancerDocument47 pagesStaging of Colorectal Cancerbo gum parkNo ratings yet
- Tyrosine Kinase Inhibitor Therapy For Advanced Gastrointestinal Stromal TumorsDocument46 pagesTyrosine Kinase Inhibitor Therapy For Advanced Gastrointestinal Stromal Tumorsbo gum parkNo ratings yet
- Right and Extended Right ColectomyDocument19 pagesRight and Extended Right Colectomybo gum parkNo ratings yet
- Colon ResectionDocument46 pagesColon Resectionbo gum parkNo ratings yet
- Imatinib For Gastrointestinal Stromal TumorsDocument46 pagesImatinib For Gastrointestinal Stromal Tumorsbo gum parkNo ratings yet
- SGD: Colorectal Cancer: I. CaseDocument7 pagesSGD: Colorectal Cancer: I. Casebo gum parkNo ratings yet
- Epidemiology, Risk Factors, and Protective FactorsDocument64 pagesEpidemiology, Risk Factors, and Protective Factorsbo gum parkNo ratings yet
- Colectomy: The ConditionDocument8 pagesColectomy: The Conditionbo gum parkNo ratings yet
- 09.16 - SGD 1 - Acute CholecystitisDocument5 pages09.16 - SGD 1 - Acute Cholecystitisbo gum parkNo ratings yet
- Gross Anatomy of The Appendix, Colon, Rectum, and AnusDocument8 pagesGross Anatomy of The Appendix, Colon, Rectum, and Anusbo gum parkNo ratings yet
- CPG - Colon Cancer (Ascrs, 2017)Document19 pagesCPG - Colon Cancer (Ascrs, 2017)bo gum parkNo ratings yet
- Thyroidectomy: Continuing Education ActivityDocument10 pagesThyroidectomy: Continuing Education Activitybo gum parkNo ratings yet
- 09.16 - SGD 1 - Acute CholecystitisDocument5 pages09.16 - SGD 1 - Acute Cholecystitisbo gum parkNo ratings yet
- Cat Muscles 2Document3 pagesCat Muscles 2nathan3602No ratings yet
- Xiphodynia - A Diagnostic ConundrumDocument6 pagesXiphodynia - A Diagnostic Conundrumweb3351No ratings yet
- Unit 2Document4 pagesUnit 2Cosmina CorbeanuNo ratings yet
- (CV) Conception Vessel MeridianDocument4 pages(CV) Conception Vessel MeridianWerner de WetNo ratings yet
- Thorax and Chest WallDocument6 pagesThorax and Chest WallDale P. PolvorosaNo ratings yet
- 8 Pieces of BrocadeDocument17 pages8 Pieces of BrocadeEdmundDante100% (2)
- Albert Gunther - Reptiles of IndiaDocument550 pagesAlbert Gunther - Reptiles of IndiaMaximiliano VillarrealNo ratings yet
- Teach Yourself ThoraxDocument29 pagesTeach Yourself ThoraxSambili Tonny100% (3)
- BLS Answer KeyDocument12 pagesBLS Answer Keysam_101100% (8)
- Anatomy Tables - Bones of The Thorax: Bone Structure Description Notes RibDocument3 pagesAnatomy Tables - Bones of The Thorax: Bone Structure Description Notes Ribyachiru121No ratings yet
- Bio CH 16Document2 pagesBio CH 16S PNo ratings yet
- The chicken skeleton: A detailed guideDocument20 pagesThe chicken skeleton: A detailed guideJoachimNo ratings yet
- Anatomy Quizbook Volume 2 Head and NeckDocument92 pagesAnatomy Quizbook Volume 2 Head and NeckSakhile NdlovuNo ratings yet
- OIA of Cat MusclesDocument8 pagesOIA of Cat Musclesksdfsd8903No ratings yet
- Belgian Carrier PigeonDocument145 pagesBelgian Carrier PigeonstepathcNo ratings yet
- Kobelco Epc 2015 Electronic Spare PartsDocument22 pagesKobelco Epc 2015 Electronic Spare Partsgeorgemartinez260788msa100% (102)
- Counterstrain - Approaches in Osteopathic Manipulative Medicine (Friedman)Document108 pagesCounterstrain - Approaches in Osteopathic Manipulative Medicine (Friedman)Alessandro100% (2)
- Test Bank Clinically Oriented Anatomy 6th Edition Moore Agur DalleyDocument19 pagesTest Bank Clinically Oriented Anatomy 6th Edition Moore Agur DalleyShirley Belisle100% (22)
- Lecture and Animation OutlineDocument80 pagesLecture and Animation OutlineAira GrandeNo ratings yet
- Skeletal System Bones and Joints PDFDocument91 pagesSkeletal System Bones and Joints PDFAiman Bañaga Arabain100% (1)
- Thorax and Lungs Assessment ChecklistDocument8 pagesThorax and Lungs Assessment ChecklistXing-Jin RomeroNo ratings yet
- At A Glance - Respiratory System TextDocument84 pagesAt A Glance - Respiratory System TextalimonyNo ratings yet
- Rabbit Anatomy Lab ReportDocument23 pagesRabbit Anatomy Lab ReportNorasyikin ZulkifliNo ratings yet
- Anatomy of Thoracic Wall: Disaripatikan Oleh Bagian Anatomi FK UnudDocument38 pagesAnatomy of Thoracic Wall: Disaripatikan Oleh Bagian Anatomi FK UnudCahyadi PermanaNo ratings yet
- Pet Size o Meter BirdsDocument2 pagesPet Size o Meter BirdsPalak AgarwalNo ratings yet
- The Respirator Y System: Mungcal, Dharlynette RTRPDocument158 pagesThe Respirator Y System: Mungcal, Dharlynette RTRPDharlyn MungcalNo ratings yet
- The Respiratory System: Supplement To Text, Chapter 9Document77 pagesThe Respiratory System: Supplement To Text, Chapter 9Christina GonezNo ratings yet
- Human Skeleton PartsDocument6 pagesHuman Skeleton PartsVeen Pascual100% (1)
- SternumDocument43 pagesSternumAnika MarshiaNo ratings yet
- Sistem RangkaDocument165 pagesSistem RangkaNadzirah ZukriNo ratings yet
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (15)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (33)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (5)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- The Tennis Partner: A Doctor's Story of Friendship and LossFrom EverandThe Tennis Partner: A Doctor's Story of Friendship and LossRating: 4.5 out of 5 stars4.5/5 (4)