You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5807)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Hamlet TimelineDocument5 pagesHamlet TimelineYi-Fang Liu100% (1)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Wrap Book A4Document27 pagesWrap Book A4doscribe100% (1)
- Pediatrics - OrthopedicsDocument2 pagesPediatrics - OrthopedicsJasmine KangNo ratings yet
- Rheumatology - Other Connective TissueDocument1 pageRheumatology - Other Connective TissueJasmine Kang100% (2)
- Rheumatology - Approach To Joint PainDocument1 pageRheumatology - Approach To Joint PainJasmine KangNo ratings yet
- Pediatrics - Neonatal Jaundice PDFDocument2 pagesPediatrics - Neonatal Jaundice PDFJasmine KangNo ratings yet
- Pediatrics - Neonatal ICUDocument2 pagesPediatrics - Neonatal ICUJasmine KangNo ratings yet
- Pediatrics - ImmunodeficiencyDocument3 pagesPediatrics - ImmunodeficiencyJasmine KangNo ratings yet
- Quiz Answers Quiz2B KeyDocument3 pagesQuiz Answers Quiz2B KeyJasmine KangNo ratings yet
- Pediatrics - Failure To Pass Meconium PDFDocument2 pagesPediatrics - Failure To Pass Meconium PDFJasmine KangNo ratings yet
- Pediatrics - Lower AirwayDocument3 pagesPediatrics - Lower AirwayJasmine KangNo ratings yet
- Quiz Answers Quiz2A KeyDocument3 pagesQuiz Answers Quiz2A KeyJasmine KangNo ratings yet
- HydronephrosisDocument17 pagesHydronephrosisShradha Khurana100% (2)
- NFHS-5 Interviewer Manual - EngDocument182 pagesNFHS-5 Interviewer Manual - EngDisability Rights AllianceNo ratings yet
- PhenylketonuriaDocument1 pagePhenylketonuriaHolly SevillanoNo ratings yet
- 05 N026 31333Document13 pages05 N026 31333Ankur AggarwalNo ratings yet
- ObesityDocument1 pageObesitycaloy10No ratings yet
- HIV Infection and AIDS: Practice EssentialsDocument52 pagesHIV Infection and AIDS: Practice EssentialsRimaNo ratings yet
- Enrile vs. Sandiganbayan (Third Division), 767 SCRA 282, August 18, 2015Document10 pagesEnrile vs. Sandiganbayan (Third Division), 767 SCRA 282, August 18, 2015TNVTRLNo ratings yet
- Sample Chapter PDFDocument12 pagesSample Chapter PDFMini Bekti NingsihNo ratings yet
- Prueba de PromotoresDocument4 pagesPrueba de PromotoresDuxan Arancibia RadichNo ratings yet
- Original Video Atlas of Oculofacial Plastic and Reconstructive Surgery Full ChapterDocument41 pagesOriginal Video Atlas of Oculofacial Plastic and Reconstructive Surgery Full Chapteralton.hopper106100% (31)
- Disease Herbarium 3Document27 pagesDisease Herbarium 3Shahin Rahman 112700gmail.comNo ratings yet
- Feeding PDF Feeding History QuesDocument8 pagesFeeding PDF Feeding History QuesSophia DaniilNo ratings yet
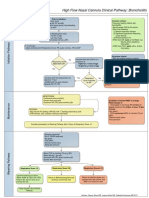
- High Flow Nasal Cannula Clinical Pathway: Bronchiolitis: Prior To Initiation: Inclusion CriteriaDocument1 pageHigh Flow Nasal Cannula Clinical Pathway: Bronchiolitis: Prior To Initiation: Inclusion Criteriad'Agung NugrohoNo ratings yet
- Health Benefits of Vegetables and FruitsDocument57 pagesHealth Benefits of Vegetables and FruitsJoseph KuriaNo ratings yet
- Apollo-Annual Report 2016 PDFDocument143 pagesApollo-Annual Report 2016 PDFShriniket PatilNo ratings yet
- Principles of Crop ProtectionDocument16 pagesPrinciples of Crop Protectionvjulieanne35No ratings yet
- Front of The ClassDocument1 pageFront of The ClassFatih AzzikraNo ratings yet
- Characteristic of Selected Soil Streptomycetes With Antimicrobial Potential Against Phytopathogenic MicroorganismsDocument21 pagesCharacteristic of Selected Soil Streptomycetes With Antimicrobial Potential Against Phytopathogenic Microorganismsvijayrasigan786No ratings yet
- Usana Essentials Dubai - Top of The Line, First Class SupplementsDocument2 pagesUsana Essentials Dubai - Top of The Line, First Class SupplementsdxbvvmNo ratings yet
- Thesis Statement Examples Cervical CancerDocument5 pagesThesis Statement Examples Cervical Cancerbrittanyjonescolumbia100% (1)
- BJH 12107Document12 pagesBJH 12107Bernard NazaraNo ratings yet
- Caregiver Benefits BrochureDocument8 pagesCaregiver Benefits BrochureNiña MoradaNo ratings yet
- June 2019 (IAL) QP - Unit 2 Edexcel Biology A-LevelDocument32 pagesJune 2019 (IAL) QP - Unit 2 Edexcel Biology A-LevelHadi El HadiNo ratings yet
- Fetal DistressDocument32 pagesFetal DistressMadhu Sudhan PandeyaNo ratings yet
- Researchassignment - Adultplayground FinalDocument13 pagesResearchassignment - Adultplayground Finalapi-276500446No ratings yet
- SINUSDocument16 pagesSINUSJune Suzete RubioNo ratings yet
- Septic Shock: Ask The ExpertDocument4 pagesSeptic Shock: Ask The ExpertIvy Dianne PascualNo ratings yet
- Industrialização TecnologicaDocument32 pagesIndustrialização TecnologicadanielreisNo ratings yet