You might also like
- DepEd CI GuidebookDocument244 pagesDepEd CI Guidebookasdfg100% (4)
- Practice Exercise For Final Assessment 2221Document3 pagesPractice Exercise For Final Assessment 2221Guneet Singh ChawlaNo ratings yet
- Unit 3 Digital Documentation: Multiple Choice QuestionsDocument7 pagesUnit 3 Digital Documentation: Multiple Choice Questions07tp27652% (21)
- Supply Chain Management 5th Edition Chopra Solutions ManualDocument3 pagesSupply Chain Management 5th Edition Chopra Solutions Manualdammar.jealousgvg6100% (18)
- Guideline MD Listing and Authorization MDS-G5 PDFDocument153 pagesGuideline MD Listing and Authorization MDS-G5 PDFSyed SalmanNo ratings yet
- DLL in Science 5 Q1 W1Document3 pagesDLL in Science 5 Q1 W1Rhinalyn Andaya Barberan100% (2)
- X-Ray Pulsing Methods For Reduced-Dose Computed Tomography in PET/CT Attenuation CorrectionDocument15 pagesX-Ray Pulsing Methods For Reduced-Dose Computed Tomography in PET/CT Attenuation CorrectionsunlianzhuNo ratings yet
- Chapter 1: Introduction: 1.1 Background and MotivationDocument5 pagesChapter 1: Introduction: 1.1 Background and Motivationnirav34No ratings yet
- Radiol 2018172656Document20 pagesRadiol 2018172656rnjNo ratings yet
- Physics and Imaging in Radiation OncologyDocument6 pagesPhysics and Imaging in Radiation Oncologydarr artNo ratings yet
- CT Sim ParametersDocument11 pagesCT Sim ParametersEskadmas BelayNo ratings yet
- Photon Counting Spectral CT Versus Conventional CT: Comparative Evaluation For Breast Imaging ApplicationDocument27 pagesPhoton Counting Spectral CT Versus Conventional CT: Comparative Evaluation For Breast Imaging Applicationcarlos56dbNo ratings yet
- Strategies For Radiation Dose OptimizationDocument10 pagesStrategies For Radiation Dose OptimizationthutaNo ratings yet
- Computed TomographyDocument4 pagesComputed TomographyemilyNo ratings yet
- Characterization of A Novel Photon Counting DetectDocument10 pagesCharacterization of A Novel Photon Counting DetectMax dos santos ramosNo ratings yet
- Development and Validation of A Low Dose Simulation Algorithm For Computed TomographyDocument9 pagesDevelopment and Validation of A Low Dose Simulation Algorithm For Computed TomographyBrankica MitrovicNo ratings yet
- Treatment Planning in Proton TherapyDocument20 pagesTreatment Planning in Proton Therapyokolinta godwin100% (1)
- Medical Physics - 2018 - Ommen - Image Quality of Conventional Images of Dual Layer SPECTRAL CT A Phantom StudyDocument13 pagesMedical Physics - 2018 - Ommen - Image Quality of Conventional Images of Dual Layer SPECTRAL CT A Phantom StudyAmril MukminNo ratings yet
- MScThesis KareliotisDocument116 pagesMScThesis KareliotisAndrés ValdezNo ratings yet
- Geometrik Kedokteran2Document5 pagesGeometrik Kedokteran2tasyaNo ratings yet
- Sarti 2012Document12 pagesSarti 2012mariaNo ratings yet
- Wavelet Based Noise Reduction in CT-Images Using Correlation AnalysisDocument20 pagesWavelet Based Noise Reduction in CT-Images Using Correlation Analysisprashant jadhavNo ratings yet
- SPECT/CT Radiation DosimetryDocument13 pagesSPECT/CT Radiation DosimetryMohamed Abd ElazizNo ratings yet
- Improving Radiotherapy Planning in Patients With MDocument14 pagesImproving Radiotherapy Planning in Patients With MTaro TenriNo ratings yet
- Medical ImagingDocument9 pagesMedical ImagingRajes WariNo ratings yet
- CT Angiography: Current Technology and Clinical Use: Go ToDocument46 pagesCT Angiography: Current Technology and Clinical Use: Go ToEuis NurvikaNo ratings yet
- Dose Reduction With Iterative Reconstruction For Coronary CT Angiography: A Systematic Review and Meta-AnalysisDocument9 pagesDose Reduction With Iterative Reconstruction For Coronary CT Angiography: A Systematic Review and Meta-AnalysisHenry MruizNo ratings yet
- Medical Imaging Systems Example QuestionsDocument2 pagesMedical Imaging Systems Example QuestionsPika17No ratings yet
- Kim 2010Document13 pagesKim 2010face bookNo ratings yet
- Radiation Dose Modulation Techniques MDCTDocument10 pagesRadiation Dose Modulation Techniques MDCTFelipe Gustavo Tercero Vega AbantoNo ratings yet
- Gislason-Lee Et Al 2014 ADRC ECR EposterDocument12 pagesGislason-Lee Et Al 2014 ADRC ECR EposterAnders ErikssonNo ratings yet
- Principles of CT and CT Technology : P CT CTT - Goldman 115Document14 pagesPrinciples of CT and CT Technology : P CT CTT - Goldman 115Madalina ConstantinNo ratings yet
- Analysis of CT and MRI Image Fusion Using Wavelet TransformDocument5 pagesAnalysis of CT and MRI Image Fusion Using Wavelet Transform18onaldo20orresNo ratings yet
- Impact of Focal Spot Size On Radiologic Image Quality - A Visual Grading AnalysisDocument10 pagesImpact of Focal Spot Size On Radiologic Image Quality - A Visual Grading AnalysisNurulazirah SalihNo ratings yet
- BulganDocument10 pagesBulganIkh nahia Ikh Nakhia PharmNo ratings yet
- Utilization Patterns of Multidetector Computed Tomography in Elective and Emergency Conditions: Indications, Exposure Risk, and Diagnostic GainDocument4 pagesUtilization Patterns of Multidetector Computed Tomography in Elective and Emergency Conditions: Indications, Exposure Risk, and Diagnostic GainJorge RodriguezNo ratings yet
- Medical Physics - 2021 - Lee - Medical X Band Linear Accelerator For High Precision RadiotherapyDocument16 pagesMedical Physics - 2021 - Lee - Medical X Band Linear Accelerator For High Precision RadiotherapyNima SalianiNo ratings yet
- T/CT Physical Principles and Attenuation Correction Prepared By: Hala Rabee/ID: s1811023 Supervisor: Dr-Mohammed Al-HjoujDocument25 pagesT/CT Physical Principles and Attenuation Correction Prepared By: Hala Rabee/ID: s1811023 Supervisor: Dr-Mohammed Al-HjoujHala YousefNo ratings yet
- Optical Coherence TomographyDocument2,567 pagesOptical Coherence Tomographyप्रताप जय हिन्द100% (1)
- CancerDocument9 pagesCancerMARIA JOSE RIVERA AVILANo ratings yet
- SPECT Imaging TechniqueDocument15 pagesSPECT Imaging TechniqueChris HartoyoNo ratings yet
- Implications of CBCT in Pediatric Dentistry-A ReviewDocument8 pagesImplications of CBCT in Pediatric Dentistry-A ReviewIJAR JOURNALNo ratings yet
- Al-Sharify 2020 IOP Conf. Ser. Mater. Sci. Eng. 870 0120431Document11 pagesAl-Sharify 2020 IOP Conf. Ser. Mater. Sci. Eng. 870 0120431Hua Hidari YangNo ratings yet
- CT Physics for Quality and Dose OptimizationDocument75 pagesCT Physics for Quality and Dose OptimizationdanaNo ratings yet
- J. Nucl. Med. Technol. 2007 Goldman 115 28Document15 pagesJ. Nucl. Med. Technol. 2007 Goldman 115 28Ruxandra LúthienNo ratings yet
- The CT Handbook Optimizing Protocols For Today's Feature Rich Scanners Chapter 1Document35 pagesThe CT Handbook Optimizing Protocols For Today's Feature Rich Scanners Chapter 1Abdullah AliNo ratings yet
- Quantitative Cone-Beam CT Imaging in Radiotherapy Parallel Computation and Comprehensive Evaluation On The TrueBeam SystemDocument8 pagesQuantitative Cone-Beam CT Imaging in Radiotherapy Parallel Computation and Comprehensive Evaluation On The TrueBeam SystemKe LuNo ratings yet
- CT Radiation ProtectionDocument8 pagesCT Radiation ProtectionKhush JainNo ratings yet
- Principles of CT and CT TechnologyDocument15 pagesPrinciples of CT and CT TechnologyLida Velasquez SierraNo ratings yet
- Qims 12 01 766Document15 pagesQims 12 01 766Hamza ArjahNo ratings yet
- Computed TomographyDocument31 pagesComputed TomographyAvik Mukherjee100% (3)
- Contrast MediaDocument11 pagesContrast MediaDEVI ANDRIANINo ratings yet
- IW Yu Leng Image Reconstruction TechniquesDocument6 pagesIW Yu Leng Image Reconstruction TechniquesNurul Hazi putriNo ratings yet
- A Fast Iterative Reconstruction Algorithm For Sparse Angle CT Based On Compressed SensingDocument6 pagesA Fast Iterative Reconstruction Algorithm For Sparse Angle CT Based On Compressed Sensingfrima kurniawanNo ratings yet
- TM 10. CT CARDIAC Artikel 2 PCD-CTDocument13 pagesTM 10. CT CARDIAC Artikel 2 PCD-CTrellvandraaaNo ratings yet
- A Dose-Neutral Image Quality Comparison of Different CBCT and CT Systems Using Paranasal Sinus Imaging Protocols and PhantomsDocument8 pagesA Dose-Neutral Image Quality Comparison of Different CBCT and CT Systems Using Paranasal Sinus Imaging Protocols and Phantomsmarito’No ratings yet
- Nano Platform For Positron Emission TomographyDocument4 pagesNano Platform For Positron Emission Tomographygopikrrishna.jNo ratings yet
- Resume C-ArmDocument4 pagesResume C-Armp27838121011No ratings yet
- Matsumoto 2016Document7 pagesMatsumoto 2016A DNo ratings yet
- Dual Energy CTDocument11 pagesDual Energy CTdeadcorpsesNo ratings yet
- 2017 - Dictionary Learning Based Low Dose Helical CT Reconstruction With Longitudinal TV ConstraintDocument1 page2017 - Dictionary Learning Based Low Dose Helical CT Reconstruction With Longitudinal TV ConstraintL AndyNo ratings yet
- JXST 26 1 2018Document29 pagesJXST 26 1 2018nasywa rahmatullailyNo ratings yet
- 3D Dose Computation AlgorithmsDocument10 pages3D Dose Computation AlgorithmsHashir SaeedNo ratings yet
- Ciocca Et Al. - 2019 - Design and Commissioning of The Nondedicated Scanning Proton Beamline For Ocular Treatment at The SynchrotronDocument12 pagesCiocca Et Al. - 2019 - Design and Commissioning of The Nondedicated Scanning Proton Beamline For Ocular Treatment at The SynchrotronKanit TanthanawigraiNo ratings yet
- Iray Technoloty Detector (NDT0505J) - 20190422Document12 pagesIray Technoloty Detector (NDT0505J) - 20190422Hernan PerezNo ratings yet
- Drtech EVS 2430W / EVS 2430GW: Safety and Regulatory Information With User 'S ManualDocument102 pagesDrtech EVS 2430W / EVS 2430GW: Safety and Regulatory Information With User 'S ManualHernan PerezNo ratings yet
- Dpx-Iq: Operator's ManualDocument166 pagesDpx-Iq: Operator's ManualZak zsNo ratings yet
- Quality Control Manual MAMMOMAT Inspiration VA10. MAMMOMAT InspirationDocument56 pagesQuality Control Manual MAMMOMAT Inspiration VA10. MAMMOMAT InspirationHernan PerezNo ratings yet
- Somatom: Hiq/ Plus/ ArDocument18 pagesSomatom: Hiq/ Plus/ ArHernan PerezNo ratings yet
- AN1131 Application Note: MIGRATING APPLICATIONS FROM ST72511/311/314/124 TO ST72521/321/324Document17 pagesAN1131 Application Note: MIGRATING APPLICATIONS FROM ST72511/311/314/124 TO ST72521/321/324Hernan PerezNo ratings yet
- Upgrade Ar - HP To HP Spiral 0.4 SegDocument42 pagesUpgrade Ar - HP To HP Spiral 0.4 SegHernan PerezNo ratings yet
- Operator GuideDocument36 pagesOperator GuideHernan PerezNo ratings yet
- AN1131 Application Note: MIGRATING APPLICATIONS FROM ST72511/311/314/124 TO ST72521/321/324Document17 pagesAN1131 Application Note: MIGRATING APPLICATIONS FROM ST72511/311/314/124 TO ST72521/321/324Hernan PerezNo ratings yet
- ChelarDocument35 pagesChelarkhawar mukhtarNo ratings yet
- Iq-Ris 3.1.0 User Manual Int en - 004rDocument75 pagesIq-Ris 3.1.0 User Manual Int en - 004rHernan PerezNo ratings yet
- Operator's ManualDocument226 pagesOperator's ManualHernan PerezNo ratings yet
- AR Ageing FinalDocument13 pagesAR Ageing FinalHAbbunoNo ratings yet
- GCSE Combined Science PDFDocument198 pagesGCSE Combined Science PDFMpumelelo Langalethu MoyoNo ratings yet
- AN2061 Application Note: EEPROM Emulation With ST10F2xxDocument15 pagesAN2061 Application Note: EEPROM Emulation With ST10F2xxleuchimed mouhNo ratings yet
- KireraDocument3 pagesKireramurithiian6588No ratings yet
- Pragmatics: The Study of Its Historical Overview, Meanings, Scope and The Context in Language UseDocument7 pagesPragmatics: The Study of Its Historical Overview, Meanings, Scope and The Context in Language UseIHINOSEN IYOHANo ratings yet
- Galvanic CorrosionDocument5 pagesGalvanic Corrosionsatheez3251No ratings yet
- Module 1 Power PlantDocument158 pagesModule 1 Power PlantEzhilarasi NagarjanNo ratings yet
- Simha Lagna: First House Ruled by The Planet Sun (LEO) : The 1st House Known As The Ascendant orDocument3 pagesSimha Lagna: First House Ruled by The Planet Sun (LEO) : The 1st House Known As The Ascendant orRahulshah1984No ratings yet
- University of Delhi Third Admission List - Bachelor of Education (B.Ed.)-2021Document8 pagesUniversity of Delhi Third Admission List - Bachelor of Education (B.Ed.)-2021FERA Future electronics and research administrationNo ratings yet
- Physice 2013 Unsolved Paper Outside Delhi PDFDocument7 pagesPhysice 2013 Unsolved Paper Outside Delhi PDFAbhilashaNo ratings yet
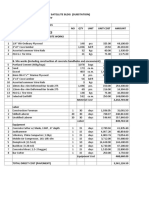
- PROPOSED ARFF BUILDINGDocument27 pagesPROPOSED ARFF BUILDINGDale Bryan S DalmacioNo ratings yet
- Speed, Velocity and FrictionDocument10 pagesSpeed, Velocity and FrictionCristie Ann GuiamNo ratings yet
- Is BN 9789526041957Document72 pagesIs BN 9789526041957supriya rakshitNo ratings yet
- PR1 Module 2Document12 pagesPR1 Module 2Ervin GonzalesNo ratings yet
- Dcs Ict2113 (Apr22) - LabDocument6 pagesDcs Ict2113 (Apr22) - LabMarwa NajemNo ratings yet
- Pressure Variation in Tunnels Sealed Trains PDFDocument258 pagesPressure Variation in Tunnels Sealed Trains PDFsivasankarNo ratings yet
- Module 5 Greek ArchDocument22 pagesModule 5 Greek ArchKyla A. EstoestaNo ratings yet
- BG BG 202102080912862 User Manual - File (Long) BG BG-8Document1 pageBG BG 202102080912862 User Manual - File (Long) BG BG-8hofolo39No ratings yet
- Jallikattu: Are Caste and Gender the Real Bulls to TameDocument67 pagesJallikattu: Are Caste and Gender the Real Bulls to TameMALLIKA NAGLENo ratings yet
- Short Time Fourier TransformDocument37 pagesShort Time Fourier TransformGopikaPrasadNo ratings yet
- Facts About SaturnDocument7 pagesFacts About SaturnGwyn CervantesNo ratings yet
- Questions Related To Open Channel Flow.Document3 pagesQuestions Related To Open Channel Flow.Mohd AmirNo ratings yet
- Ch1 - A Perspective On TestingDocument41 pagesCh1 - A Perspective On TestingcnshariffNo ratings yet
- 10.6 Heat Conduction Through Composite WallsDocument35 pages10.6 Heat Conduction Through Composite WallsEngr Muhammad AqibNo ratings yet