You might also like
- Biophysical Properties in Glaucoma: Diagnostic TechnologiesFrom EverandBiophysical Properties in Glaucoma: Diagnostic TechnologiesIngrida JanulevicieneNo ratings yet
- Obat GlaukomaDocument8 pagesObat GlaukomaMuhammad Farrash HadyanNo ratings yet
- Comparison of IOP after water test in glaucoma patients on Latanoprost vs. trabeculectomyDocument7 pagesComparison of IOP after water test in glaucoma patients on Latanoprost vs. trabeculectomyDimas Djiwa DNo ratings yet
- 100157-Article Text-820-1-10-20210225Document7 pages100157-Article Text-820-1-10-20210225Dimas Djiwa DNo ratings yet
- Jurnal Netarsudil2Document12 pagesJurnal Netarsudil2ppds standartigaNo ratings yet
- Netarsudil A Novel Intra Ocular Pressure Lowering AgentDocument3 pagesNetarsudil A Novel Intra Ocular Pressure Lowering Agentalifah syarafinaNo ratings yet
- Intraocular Pressure-Lowering Efficacy and Safety of Bimatoprost 0.03% Therapy For Primary Open-Angle Glaucoma and Ocular Hypertension Patients in ChinaDocument9 pagesIntraocular Pressure-Lowering Efficacy and Safety of Bimatoprost 0.03% Therapy For Primary Open-Angle Glaucoma and Ocular Hypertension Patients in ChinaAyu Ersya WindiraNo ratings yet
- Jurnal NcankDocument6 pagesJurnal NcankGilang IrwansyahNo ratings yet
- Jurnal Mata 3Document4 pagesJurnal Mata 3Ami AntariksawatiNo ratings yet
- Dry Eye.Document9 pagesDry Eye.Kiky RatnaNo ratings yet
- Faculty Talk AIOS 2023Document15 pagesFaculty Talk AIOS 2023divya kesarwaniNo ratings yet
- IJG 0b013e3182595075Document5 pagesIJG 0b013e3182595075EmirgibraltarNo ratings yet
- OPTH 10337 Tolerability and Effectiveness of Preservative Free Dorzolam 061210Document10 pagesOPTH 10337 Tolerability and Effectiveness of Preservative Free Dorzolam 061210Pra BowoNo ratings yet
- IBEPE StudyDocument8 pagesIBEPE StudyKaran KumarswamyNo ratings yet
- Imp Landmark Glauc StudiesDocument100 pagesImp Landmark Glauc StudiesASHOK KUMAR SINGHNo ratings yet
- Intraocular Pressure After Phacoemulsification in Patients With Uncontrolled Primary Open Angle GlaucomaDocument6 pagesIntraocular Pressure After Phacoemulsification in Patients With Uncontrolled Primary Open Angle GlaucomaStevan Arta RisajayaNo ratings yet
- MainDocument7 pagesMainiSee ClinicNo ratings yet
- Opth 8 1311 PDFDocument6 pagesOpth 8 1311 PDFJocho NeavesNo ratings yet
- Cataract Surgery and Intraocular Pressure in Glaucoma: ReviewDocument8 pagesCataract Surgery and Intraocular Pressure in Glaucoma: ReviewJackNo ratings yet
- Ocular Hypertension after PRKDocument5 pagesOcular Hypertension after PRKMaria Angelina BunawanNo ratings yet
- 24-Hour IOP Control with BBFCDocument10 pages24-Hour IOP Control with BBFCsondiNo ratings yet
- Circadian Effect of LatanoprostDocument8 pagesCircadian Effect of LatanoprostTushar BatraNo ratings yet
- tmp1BE0 TMPDocument4 pagestmp1BE0 TMPFrontiersNo ratings yet
- Lerner SFDocument9 pagesLerner SFAdriana FallaNo ratings yet
- Latanoprostene Bunod 0.024% Versus Timolol Maleate 0.5% in Subjects With Open-Angle Glaucoma or Ocular Hypertension The APOLLO StudyDocument11 pagesLatanoprostene Bunod 0.024% Versus Timolol Maleate 0.5% in Subjects With Open-Angle Glaucoma or Ocular Hypertension The APOLLO StudybungagladysNo ratings yet
- ABSTRACT - BOOK - 10th IcgsDocument135 pagesABSTRACT - BOOK - 10th Icgsd_kourkoutasNo ratings yet
- Research ArticleDocument7 pagesResearch ArticleMarcella PolittonNo ratings yet
- American Journal of Ophthalmology Case Reports: Yael Sharon, David S. Chu TDocument5 pagesAmerican Journal of Ophthalmology Case Reports: Yael Sharon, David S. Chu TDaviel Quin DavNo ratings yet
- First Experience With BAK-free Travoprost 0.004% in Topical Glaucoma MedicationDocument4 pagesFirst Experience With BAK-free Travoprost 0.004% in Topical Glaucoma Medicationsetiahermawan99No ratings yet
- 15) Refractory Open-Angle Glaucoma After Neodymium - Yttrium-Aluminum-Garnet Laser Lysis of Vitreous FloatersDocument6 pages15) Refractory Open-Angle Glaucoma After Neodymium - Yttrium-Aluminum-Garnet Laser Lysis of Vitreous FloatershasdiniNo ratings yet
- Prospective Evaluation of Acupuncture As Treatment For GlaucomaDocument10 pagesProspective Evaluation of Acupuncture As Treatment For Glaucoma16.11Hz MusicNo ratings yet
- Modern Capabilities of Surgical Management of Patients With Open-Angle Glaucoma Combined With CataractDocument5 pagesModern Capabilities of Surgical Management of Patients With Open-Angle Glaucoma Combined With CataractTyasBanggaPribadieNo ratings yet
- 2015 Article 246Document15 pages2015 Article 246RinaWulandariDjajoesmanNo ratings yet
- Efficacy of Latanoprostene Bunod 0.024% Compared With Timolol 0.5% in Lowering Intraocular Pressure Over 24 HoursDocument9 pagesEfficacy of Latanoprostene Bunod 0.024% Compared With Timolol 0.5% in Lowering Intraocular Pressure Over 24 HoursAnnisa AuliaNo ratings yet
- Jurnal Mata InggrisDocument5 pagesJurnal Mata InggrisAnonymous HNGH1oNo ratings yet
- Ijo 07 05 832 (1) AsddsaDocument5 pagesIjo 07 05 832 (1) AsddsaDyera JessenskyNo ratings yet
- Anti-VEGF Treatment Is The Key Strategy For Neovascular Glaucoma Management in The Short TermDocument8 pagesAnti-VEGF Treatment Is The Key Strategy For Neovascular Glaucoma Management in The Short TermhellowNo ratings yet
- Management of GlaucomaDocument7 pagesManagement of GlaucomaAlbertus Bayu KristiantoNo ratings yet
- Tatalaksana Operatif Dan Pascaoperatif Pada Pasien Juvenile Open Angle Glaucoma JOAG - Andreas Lukita HalimDocument14 pagesTatalaksana Operatif Dan Pascaoperatif Pada Pasien Juvenile Open Angle Glaucoma JOAG - Andreas Lukita HalimINDRINo ratings yet
- Acute Orbital Compartment Syndrome (AOCSDocument3 pagesAcute Orbital Compartment Syndrome (AOCSFrancois Donatien De SadeNo ratings yet
- Revista Brasileira de AnestesiologiaDocument4 pagesRevista Brasileira de Anestesiologiafarid akbarNo ratings yet
- Jurnal Reading GlaucomaDocument6 pagesJurnal Reading GlaucomawidyawirapNo ratings yet
- Facoemulsifucacion + Stent TrabecularDocument8 pagesFacoemulsifucacion + Stent TrabecularCarlos VerdiNo ratings yet
- 10 1016@j Jcrs 2014 12 054-2Document5 pages10 1016@j Jcrs 2014 12 054-2VaniaNo ratings yet
- Vitrectomy Results in Proliferative Diabetic RetinopathyDocument3 pagesVitrectomy Results in Proliferative Diabetic RetinopathyRohamonangan TheresiaNo ratings yet
- Eye 1989109 ADocument7 pagesEye 1989109 APrasetya Rastra SewakottamaNo ratings yet
- Efficacy of Selective Laser Trabeculoplasty For Normal Tension Glaucoma: 1 Year ResultsDocument6 pagesEfficacy of Selective Laser Trabeculoplasty For Normal Tension Glaucoma: 1 Year ResultsdechastraNo ratings yet
- Lapkas Glaukoma Pemasangan Implan GDD Lapkas Glaukoma (AutoRecovered)Document14 pagesLapkas Glaukoma Pemasangan Implan GDD Lapkas Glaukoma (AutoRecovered)Vincent RoorohNo ratings yet
- Glaucoma Case ReportDocument9 pagesGlaucoma Case Reportsuci caraswatiNo ratings yet
- Innovations in Medical Management of GlaucomaDocument31 pagesInnovations in Medical Management of GlaucomaAnumeha Jindal100% (2)
- GLAUKOMA2Document12 pagesGLAUKOMA2NorytaWahyuniawatiAsfianaNo ratings yet
- Intraocular Pressure 1 Year After Vitrectomy in Eyes Without A History of Glaucoma or Ocular HypertensionDocument7 pagesIntraocular Pressure 1 Year After Vitrectomy in Eyes Without A History of Glaucoma or Ocular HypertensionSyifa NahdiyahNo ratings yet
- Tugas Akademik 13-Journal Reading 4-Glaukoma-Galuh Yulieta - 240215 - 072026Document8 pagesTugas Akademik 13-Journal Reading 4-Glaukoma-Galuh Yulieta - 240215 - 072026Arina SetyaningrumNo ratings yet
- Efikasi TX Gukoma 2016Document37 pagesEfikasi TX Gukoma 2016Al-Harits OctaNo ratings yet
- Long Term Outcome of Secondary Glaucoma Following Vitreoretinal SurgeryDocument3 pagesLong Term Outcome of Secondary Glaucoma Following Vitreoretinal SurgeryNur Camelia PragnandaNo ratings yet
- Glaukoma Case ReportDocument9 pagesGlaukoma Case ReportHIstoryNo ratings yet
- Menejemen Kronik Uveitis Anterior RekurenDocument6 pagesMenejemen Kronik Uveitis Anterior RekurenLuthfan HakimNo ratings yet
- MataDocument5 pagesMatavikrizkaNo ratings yet
- AVB Christakis2016Document10 pagesAVB Christakis2016Ahmed NahrawyNo ratings yet
- Research ArticleDocument7 pagesResearch ArticlePhei Qing TjangNo ratings yet
- Journal Reading - Dr. Monika AyuningrumDocument12 pagesJournal Reading - Dr. Monika Ayuningrumamka chanNo ratings yet
- Laporan Kasus - Dr. Annisa Putri SiregarDocument17 pagesLaporan Kasus - Dr. Annisa Putri Siregaramka chanNo ratings yet
- Journal Reading - DR Dwi Atikah SariDocument6 pagesJournal Reading - DR Dwi Atikah Sariamka chanNo ratings yet
- Journal Reading - Dr. Sri Rejeki SinagaDocument10 pagesJournal Reading - Dr. Sri Rejeki Sinagaamka chanNo ratings yet
- Journal Reading - Dr. Sri Rejeki SinagaDocument10 pagesJournal Reading - Dr. Sri Rejeki Sinagaamka chanNo ratings yet
- Journal Reading - Dr. Amanda RizkaDocument6 pagesJournal Reading - Dr. Amanda RizkaMohd. Ilham Fat-Thur Rahman MDNo ratings yet
- Preparation of Water For Injection For Injection Dosage FormDocument2 pagesPreparation of Water For Injection For Injection Dosage FormDonia GamalNo ratings yet
- Psoriatic Arthritis - StatPearls - NCBI BookshelfDocument14 pagesPsoriatic Arthritis - StatPearls - NCBI BookshelfDhany karubuyNo ratings yet
- Respiratory PharmacologyDocument26 pagesRespiratory PharmacologyShashanka PoudelNo ratings yet
- Psych Drugs Cheat SheetDocument4 pagesPsych Drugs Cheat SheetHJ G100% (3)
- Ceftriaxone SodiumDocument3 pagesCeftriaxone SodiumjohannakatebellyNo ratings yet
- Thyroid Disorders 1Document53 pagesThyroid Disorders 1Abdulrahman AlshehriNo ratings yet
- Gupta Kumar - Nano Meningkatkan BA DLLDocument40 pagesGupta Kumar - Nano Meningkatkan BA DLLHesti HariantiNo ratings yet
- Review On Spectroscopic Analytical Methods For Determination of Metformin HydrochlorideDocument5 pagesReview On Spectroscopic Analytical Methods For Determination of Metformin HydrochlorideIjrei JournalNo ratings yet
- 2.review of LiteratureDocument20 pages2.review of LiteratureMjd ObiedNo ratings yet
- Data Obat Apotek Okt2023Document26 pagesData Obat Apotek Okt2023apoteknyarosiNo ratings yet
- Assignment - Medicines Development Process and Good Clinical PracticeDocument2 pagesAssignment - Medicines Development Process and Good Clinical PracticeZornicaBorisovaNo ratings yet
- Case 3Document3 pagesCase 3Irish LigayaNo ratings yet
- Ambrisentan: Jamie D. Croxtall and Susan J. KeamDocument10 pagesAmbrisentan: Jamie D. Croxtall and Susan J. KeamElden Kyle BillonesNo ratings yet
- Pyq ToxicoDocument5 pagesPyq ToxicoLeeshaaLenee Paramanantha KumarNo ratings yet
- Mono Witch Hazel Buccal enDocument6 pagesMono Witch Hazel Buccal enTom DelongeNo ratings yet
- Comparison of A Preservative Free Nonsteroidal.Document7 pagesComparison of A Preservative Free Nonsteroidal.Danty IndriastutyNo ratings yet
- Festin - Drug Study 3Document22 pagesFestin - Drug Study 3Hazel Mae FestinNo ratings yet
- Parental DoseDocument51 pagesParental DoseSHIVAM SHARDANo ratings yet
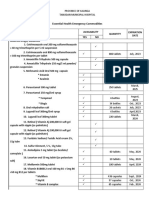
- DRRMH InventoryDocument4 pagesDRRMH InventoryJmdmdh Rizal KalingaNo ratings yet
- May 8-12, 2023 Deped, Lapu-Lapu City, CebuDocument40 pagesMay 8-12, 2023 Deped, Lapu-Lapu City, CebuRuth Carin - MalubayNo ratings yet
- Daftar Harga Erlimpex 2021Document1 pageDaftar Harga Erlimpex 2021Herman KisafNo ratings yet
- Sample: Reading Sub-Test - Question Paper: Part ADocument24 pagesSample: Reading Sub-Test - Question Paper: Part ADr. Emad Elbadawy د عماد البدويNo ratings yet
- Drug CompilationDocument39 pagesDrug CompilationANa AntonioNo ratings yet
- Managing Acute Pain After SurgeryDocument7 pagesManaging Acute Pain After SurgeryIsaac heinekenNo ratings yet
- Jose Luis Hernandez BSN Ii - 2Document1 pageJose Luis Hernandez BSN Ii - 2Jose Luis HernandezNo ratings yet
- Classification of Crude Drugs GuideDocument26 pagesClassification of Crude Drugs GuideDeepanshu 1459No ratings yet
- Drug ClassificationsDocument3 pagesDrug ClassificationsLaura Hernandez100% (3)
- E Cart DrugsDocument2 pagesE Cart DrugsxmitchxNo ratings yet
- Anesthesia For Elderly Patient With Hip Fracture Case FileDocument2 pagesAnesthesia For Elderly Patient With Hip Fracture Case Filehttps://medical-phd.blogspot.comNo ratings yet
- Rheumatoid ArthritisDocument45 pagesRheumatoid ArthritisThe AbyssinicansNo ratings yet
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (14)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 3.5 out of 5 stars3.5/5 (2)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (33)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (327)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (5)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisFrom EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (3)