You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- FREE 2022 ACLS Study Guide - ACLS Made Easy! PDFDocument18 pagesFREE 2022 ACLS Study Guide - ACLS Made Easy! PDFkumar23No ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
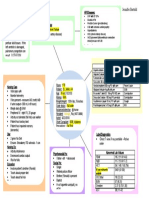
- STEMI Patho/Concept MapDocument1 pageSTEMI Patho/Concept Maplaylers_0767% (3)
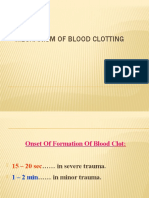
- Clotting MechanismDocument14 pagesClotting MechanismUzma KhanNo ratings yet
- Subject: - Topics: Cholecystitis: Adult Health NursingDocument17 pagesSubject: - Topics: Cholecystitis: Adult Health NursingUzma KhanNo ratings yet
- Aftab Ghouri: Shaheed Mohtarma Benazir Bhutto Medical University LarkanaDocument46 pagesAftab Ghouri: Shaheed Mohtarma Benazir Bhutto Medical University LarkanaUzma KhanNo ratings yet
- Chapter 11 - Cyanosis: Rosen'S Emergency Medicine 9Th EdDocument12 pagesChapter 11 - Cyanosis: Rosen'S Emergency Medicine 9Th EdUzma KhanNo ratings yet
- Cystic Fibrosis2Document24 pagesCystic Fibrosis2Uzma KhanNo ratings yet
- Anatomy of External EyeDocument39 pagesAnatomy of External EyeUzma KhanNo ratings yet
- Chronic Dry CoughDocument119 pagesChronic Dry CoughUzma KhanNo ratings yet
- Contra-Indications: NVQ Level 2 Beauty TherapyDocument24 pagesContra-Indications: NVQ Level 2 Beauty TherapyUzma Khan100% (1)
- Cyanosis: Epidemiology PathophysiologyDocument1 pageCyanosis: Epidemiology PathophysiologyUzma KhanNo ratings yet
- Presenter: DR Edalia Facilitator: Prof AdamDocument35 pagesPresenter: DR Edalia Facilitator: Prof AdamUzma KhanNo ratings yet
- Cardiogenic ShockDocument3 pagesCardiogenic ShockUzma KhanNo ratings yet
- Anatomy and Physiology For NursesDocument39 pagesAnatomy and Physiology For NursesUzma KhanNo ratings yet
- Cardiovascular SystemDocument23 pagesCardiovascular SystemUzma KhanNo ratings yet
- Cardiac Conduction: Shoiab AlamDocument26 pagesCardiac Conduction: Shoiab AlamUzma KhanNo ratings yet
- Communicable DiseasesDocument73 pagesCommunicable DiseasesUzma KhanNo ratings yet
- CVA (Dr. Kwasa)Document23 pagesCVA (Dr. Kwasa)Uzma KhanNo ratings yet
- Physiology of Cardiac Conduction and Contractility: Shoaib AlamDocument16 pagesPhysiology of Cardiac Conduction and Contractility: Shoaib AlamUzma KhanNo ratings yet
- Blood Grouping Experiment (Theory) - Immunology Virtual Lab I - Biotechnology and Biomedical Engineering - Amrita Vishwa Vidyapeetham Virtual LabDocument5 pagesBlood Grouping Experiment (Theory) - Immunology Virtual Lab I - Biotechnology and Biomedical Engineering - Amrita Vishwa Vidyapeetham Virtual LabUzma KhanNo ratings yet
- Detection of Cellular Changes After InjuryDocument18 pagesDetection of Cellular Changes After InjuryUzma KhanNo ratings yet
- Cardiovascular System: Shoaib AlamDocument28 pagesCardiovascular System: Shoaib AlamUzma KhanNo ratings yet
- CraniotomyDocument10 pagesCraniotomyUzma KhanNo ratings yet
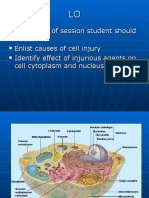
- At The End of Session Student Should Be Able To Enlist Causes of Cell Injury Identify Effect of Injurious Agents On Cell Cytoplasm and NucleusDocument29 pagesAt The End of Session Student Should Be Able To Enlist Causes of Cell Injury Identify Effect of Injurious Agents On Cell Cytoplasm and NucleusUzma KhanNo ratings yet
- Gram Negative BacteriaDocument6 pagesGram Negative BacteriaUzma KhanNo ratings yet
- HypertensionDocument46 pagesHypertensionUzma KhanNo ratings yet
- Contra Indications To Electrical EpilationDocument30 pagesContra Indications To Electrical EpilationUzma KhanNo ratings yet
- Anatomy & Physiology of Endocrine SystemDocument34 pagesAnatomy & Physiology of Endocrine SystemUzma Khan100% (1)
- BrainDocument23 pagesBrainUzma KhanNo ratings yet
- GI Bleed CaseDocument7 pagesGI Bleed CaseUzma KhanNo ratings yet
- Cardiovascular DisordersDocument83 pagesCardiovascular DisordersUzma KhanNo ratings yet
- CA CardiovascularDocument10 pagesCA CardiovascularNina OaipNo ratings yet
- Atheroma - Wikipedia, The Free EncyclopediaDocument9 pagesAtheroma - Wikipedia, The Free EncyclopediaBhadresh MangukiyaNo ratings yet
- Essentials of Diagnosis, Treatment, and Application of Cardiac and Peripheral Vascular DiseasesDocument295 pagesEssentials of Diagnosis, Treatment, and Application of Cardiac and Peripheral Vascular DiseasesMichael Brunet100% (1)
- Pre and Post Angiography and Angioplasty CareDocument34 pagesPre and Post Angiography and Angioplasty Carempimmi khanchannel50% (2)
- Cardiovascular Drugs XL ChartDocument4 pagesCardiovascular Drugs XL Chartcdp158767% (3)
- Cardiovascular Examination FinalDocument28 pagesCardiovascular Examination FinalAllen Caine Taabbil100% (1)
- Know About Pediatric Cardiac SurgeryDocument8 pagesKnow About Pediatric Cardiac SurgeryAshish DolasNo ratings yet
- DobutamineDocument2 pagesDobutamineJaessa FelicianoNo ratings yet
- Effect of Progressive Muscle Relaxation Combined With Deep Breathing Technique Immediately After Aerobic Exercises On Essential HypertensionDocument2 pagesEffect of Progressive Muscle Relaxation Combined With Deep Breathing Technique Immediately After Aerobic Exercises On Essential HypertensionNetraNo ratings yet
- Crs Peripheral Artery Disease - Billi Brian GeniroDocument21 pagesCrs Peripheral Artery Disease - Billi Brian Genirofathiya nurkhalisaNo ratings yet
- Cardiovascular Questions - LippincotDocument3 pagesCardiovascular Questions - LippincotRammy KhanNo ratings yet
- Pulmonary Valve StenosisDocument6 pagesPulmonary Valve StenosisKobby AmoahNo ratings yet
- Internal MedicineDocument161 pagesInternal Medicinemain.genevive.dilig100% (1)
- Critical Limb IschemiaDocument2 pagesCritical Limb IschemiaDorin DvornicNo ratings yet
- BMC - Hospital Development Plan - 2023-2028Document92 pagesBMC - Hospital Development Plan - 2023-2028Rainier VillanuevaNo ratings yet
- Ventricular Aneurysm: PathophysiologyDocument3 pagesVentricular Aneurysm: PathophysiologyMegan N. ReyesNo ratings yet
- Hypertensive CrisisDocument7 pagesHypertensive Crisisalul847474No ratings yet
- CHF Concept MapDocument1 pageCHF Concept MapChristy Wegner Cooper100% (4)
- Raksha Yadav B.SC Nursing 2 Year Aiims, JodhpurDocument22 pagesRaksha Yadav B.SC Nursing 2 Year Aiims, JodhpurrohitNo ratings yet
- ArtherosclerosisDocument23 pagesArtherosclerosistanyagargNo ratings yet
- Basic ECG Lecture - NewDocument148 pagesBasic ECG Lecture - NewAradhanaRamchandaniNo ratings yet
- Etiologji Dhe Epidemiologjia e StrokeDocument7 pagesEtiologji Dhe Epidemiologjia e StrokegranitNo ratings yet
- Congenital Heart Disease - ASDDocument36 pagesCongenital Heart Disease - ASDAuni Akif Aleesa100% (1)
- Congestive Heart FailureDocument13 pagesCongestive Heart Failureali alrashediNo ratings yet
- Neocordil CapsuleDocument3 pagesNeocordil Capsulehk_scribdNo ratings yet
- Drug Study - NitroglycerinDocument1 pageDrug Study - Nitroglycerinchriscustodio100% (1)
- Cardiology OSCEsDocument85 pagesCardiology OSCEsMed StudentNo ratings yet
- Cardiopatias CianoticasDocument9 pagesCardiopatias CianoticasAngie CalderónNo ratings yet