You might also like
- Cyanosis: Pathophysiology and Differential DiagnosisDocument11 pagesCyanosis: Pathophysiology and Differential DiagnosisFirah Triple'sNo ratings yet
- Approach To Cyanosis in A NeonateDocument8 pagesApproach To Cyanosis in A NeonateSujeetNo ratings yet
- Aproach To A Patient With CyanosisDocument18 pagesAproach To A Patient With CyanosisEsther AumaNo ratings yet
- 1 Sca PDFDocument29 pages1 Sca PDFJennyu YuNo ratings yet
- Congenital Blood DisordersDocument32 pagesCongenital Blood DisordersErika CadawanNo ratings yet
- 4 2Document39 pages4 2Anonymous GWPdocUtNo ratings yet
- Chap 184Document11 pagesChap 184Santoso 9JimmyNo ratings yet
- Practice Question Week 1Document9 pagesPractice Question Week 1Gps PandetteNo ratings yet
- Cyanosis - WikipediaDocument17 pagesCyanosis - WikipediaIhteshamNo ratings yet
- Destiny SeminarDocument35 pagesDestiny SeminarMbamalu FrancisNo ratings yet
- Robbins Basic Pathology 9th Edition QBankDocument4 pagesRobbins Basic Pathology 9th Edition QBankVarshini Tamil SelvanNo ratings yet
- ClubbingDocument44 pagesClubbingAkshat Srivastava100% (1)
- K-5 Pathophysiology of Cyanotic Congenital Heart DefectsDocument15 pagesK-5 Pathophysiology of Cyanotic Congenital Heart DefectsJessica GintingNo ratings yet
- Pathophysiology of Cyanotic Congenital Heart DefectsDocument16 pagesPathophysiology of Cyanotic Congenital Heart Defectsbonar46No ratings yet
- 8 HypoxemiaDocument5 pages8 HypoxemiaVictor PazNo ratings yet
- V.Sowndharya MeeraDocument22 pagesV.Sowndharya MeeraGopi NathNo ratings yet
- 2014 Kabir Et Al. - Chronic Eosinophilic Leukaemia Presenting With A CDocument4 pages2014 Kabir Et Al. - Chronic Eosinophilic Leukaemia Presenting With A CPratyay HasanNo ratings yet
- Running Head: Sickle Cell Anemia 1Document11 pagesRunning Head: Sickle Cell Anemia 1api-264952333No ratings yet
- Jamees - Cyanosis IntroductionDocument41 pagesJamees - Cyanosis IntroductionjameespkNo ratings yet
- Pathophysiology Review QuestionsDocument30 pagesPathophysiology Review QuestionsKhuzema SaeedNo ratings yet
- Nephrotic Syndrome Msn-3Document12 pagesNephrotic Syndrome Msn-3Bibi Renu100% (3)
- نسخة من HemoglobipathiesDocument63 pagesنسخة من Hemoglobipathiesnour khaleel Mohammad BojaNo ratings yet
- Hemolytic AnemiaDocument23 pagesHemolytic AnemiaRashed ShatnawiNo ratings yet
- Sickle Cell Anemia: Hba Α Β Hba …….. Α Δ Hb F ……… Α, ΓDocument29 pagesSickle Cell Anemia: Hba Α Β Hba …….. Α Δ Hb F ……… Α, ΓYolanda UriolNo ratings yet
- Group 1 SiadhDocument20 pagesGroup 1 SiadhArul MNo ratings yet
- Approach To Infants and Children With Cyanotic Congenital Heart DiseaseDocument9 pagesApproach To Infants and Children With Cyanotic Congenital Heart DiseaseAnonymous 46B3TtLYjNo ratings yet
- Hematology EMQDocument7 pagesHematology EMQfrabzi100% (1)
- Chapter 49Document6 pagesChapter 49Melissa Aina Mohd YusofNo ratings yet
- Anemi Aplastik Dan MielodisplasiaDocument34 pagesAnemi Aplastik Dan MielodisplasiaRoby KieranNo ratings yet
- Pathology McqsDocument40 pagesPathology Mcqspkpowerhouse100% (1)
- Medico QuierurgicoDocument12 pagesMedico QuierurgicojulialeoNo ratings yet
- MCQ PneuDocument60 pagesMCQ PneuYanesh Bishundat0% (1)
- CyanosisDocument58 pagesCyanosisCaroline Shira Deori100% (1)
- Haematology: Questions&AnswersDocument87 pagesHaematology: Questions&AnswersCielNo ratings yet
- Nephrotic Syndrome: BackgroundDocument25 pagesNephrotic Syndrome: BackgroundsDamnNo ratings yet
- Kumar: Robbins Basic Pathology, 9th EditionDocument4 pagesKumar: Robbins Basic Pathology, 9th EditionAmar AlkhafajiNo ratings yet
- Haemolysis i-WPS OfficeDocument69 pagesHaemolysis i-WPS OfficeIdrissa ContehNo ratings yet
- Practice Test QuestionsDocument19 pagesPractice Test QuestionsEman ArmadoNo ratings yet
- Hereditary SpherocytosisDocument23 pagesHereditary SpherocytosisKashan SiddiquiNo ratings yet
- Plabable 2020 Hematology MfaDocument87 pagesPlabable 2020 Hematology MfaDr. Saqib RazaNo ratings yet
- Bloodstream. Together, The Two Proteins Are Known As The Haptoglobin-Hemoglobin Complex. Your LiverDocument6 pagesBloodstream. Together, The Two Proteins Are Known As The Haptoglobin-Hemoglobin Complex. Your LiverMuhammad ArifNo ratings yet
- Seminar On Nephrotic Syndrome: Medical Surgical NursingDocument15 pagesSeminar On Nephrotic Syndrome: Medical Surgical NursingGargi MP100% (1)
- MS Practice Questions With RationaleDocument13 pagesMS Practice Questions With RationaleRey Gil Flee GabonadaNo ratings yet
- Innocent Heart MurmursDocument10 pagesInnocent Heart Murmurslindsay_weiss_6No ratings yet
- Nephrotic Syndrome-1Document21 pagesNephrotic Syndrome-1Wondimu EliasNo ratings yet
- The Correct Answer Is B. The Combination of Leg Edema and Pulmonary Edema (AsDocument13 pagesThe Correct Answer Is B. The Combination of Leg Edema and Pulmonary Edema (AsMitz JuneNo ratings yet
- Hematoloical Disorders in PregnancyDocument25 pagesHematoloical Disorders in PregnancyMonika shankarNo ratings yet
- Approach To Cyanosis in A NeonateDocument12 pagesApproach To Cyanosis in A NeonateXerxyllXyreaneLinaoNo ratings yet
- Sickle Cell AnemiaDocument7 pagesSickle Cell AnemiaJuma AwarNo ratings yet
- Haematology AnemiaDocument7 pagesHaematology AnemiaGayanNo ratings yet
- CK SamplesDocument63 pagesCK SamplesAppu ayyala100% (2)
- Anemia: Dr. Tanbira Alam MBBS, M.PhilDocument22 pagesAnemia: Dr. Tanbira Alam MBBS, M.Philsatvindar_muNo ratings yet
- A. Primary GlaucomaDocument5 pagesA. Primary GlaucomasekiannNo ratings yet
- Complete Blood Count: DR: Mona Wagdy Ayad Assist Prof of Clinical PathologyDocument28 pagesComplete Blood Count: DR: Mona Wagdy Ayad Assist Prof of Clinical Pathologymarwanelsaeed1981No ratings yet
- Clinical Approach To A Neonate With Cyanosis - Review - IJPDocument11 pagesClinical Approach To A Neonate With Cyanosis - Review - IJPSridhar KaushikNo ratings yet
- Sickle Cell Diseases and Thalasemia Asma2Document60 pagesSickle Cell Diseases and Thalasemia Asma2Female calmNo ratings yet
- Hematology QuestionsDocument171 pagesHematology QuestionsVikkineshwaran Siva SubramaniamNo ratings yet
- Clotting MechanismDocument14 pagesClotting MechanismUzma KhanNo ratings yet
- Aftab Ghouri: Shaheed Mohtarma Benazir Bhutto Medical University LarkanaDocument46 pagesAftab Ghouri: Shaheed Mohtarma Benazir Bhutto Medical University LarkanaUzma KhanNo ratings yet
- Cellular Injury Apoptosis and NecrosisDocument15 pagesCellular Injury Apoptosis and NecrosisUzma KhanNo ratings yet
- Subject: - Topics: Cholecystitis: Adult Health NursingDocument17 pagesSubject: - Topics: Cholecystitis: Adult Health NursingUzma KhanNo ratings yet
- Cystic Fibrosis2Document24 pagesCystic Fibrosis2Uzma KhanNo ratings yet
- Contra-Indications: NVQ Level 2 Beauty TherapyDocument24 pagesContra-Indications: NVQ Level 2 Beauty TherapyUzma Khan100% (1)
- Cardiovascular SystemDocument23 pagesCardiovascular SystemUzma KhanNo ratings yet
- Anatomy and Physiology For NursesDocument39 pagesAnatomy and Physiology For NursesUzma KhanNo ratings yet
- Cardiogenic ShockDocument3 pagesCardiogenic ShockUzma KhanNo ratings yet
- Chronic Dry CoughDocument119 pagesChronic Dry CoughUzma KhanNo ratings yet
- Anatomy of External EyeDocument39 pagesAnatomy of External EyeUzma KhanNo ratings yet
- Community Health Nursing 3 (Ansari Notes) - 1Document41 pagesCommunity Health Nursing 3 (Ansari Notes) - 1Uzma KhanNo ratings yet
- Cardiovascular System ,.Document50 pagesCardiovascular System ,.Uzma KhanNo ratings yet
- 2nd Year Nursing PharmacologyDocument50 pages2nd Year Nursing PharmacologyUzma KhanNo ratings yet
- Presenter: DR Edalia Facilitator: Prof AdamDocument35 pagesPresenter: DR Edalia Facilitator: Prof AdamUzma KhanNo ratings yet
- Communicable DiseasesDocument73 pagesCommunicable DiseasesUzma KhanNo ratings yet
- Chemicals, Cancer, and You FSDocument12 pagesChemicals, Cancer, and You FSEd DearNo ratings yet
- Cardiovascular System: Shoaib AlamDocument28 pagesCardiovascular System: Shoaib AlamUzma KhanNo ratings yet
- Physiology of Cardiac Conduction and Contractility: Shoaib AlamDocument16 pagesPhysiology of Cardiac Conduction and Contractility: Shoaib AlamUzma KhanNo ratings yet
- Cardiac Conduction: Shoiab AlamDocument26 pagesCardiac Conduction: Shoiab AlamUzma KhanNo ratings yet
- Detection of Cellular Changes After InjuryDocument18 pagesDetection of Cellular Changes After InjuryUzma KhanNo ratings yet
- CraniotomyDocument10 pagesCraniotomyUzma KhanNo ratings yet
- CVA (Dr. Kwasa)Document23 pagesCVA (Dr. Kwasa)Uzma KhanNo ratings yet
- Cyanosis: Epidemiology PathophysiologyDocument1 pageCyanosis: Epidemiology PathophysiologyUzma KhanNo ratings yet
- CHF UndergraduateDocument41 pagesCHF UndergraduateUzma KhanNo ratings yet
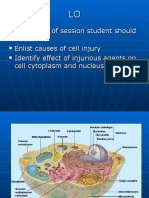
- At The End of Session Student Should Be Able To Enlist Causes of Cell Injury Identify Effect of Injurious Agents On Cell Cytoplasm and NucleusDocument29 pagesAt The End of Session Student Should Be Able To Enlist Causes of Cell Injury Identify Effect of Injurious Agents On Cell Cytoplasm and NucleusUzma KhanNo ratings yet
- The Cell Structure and FunctionDocument83 pagesThe Cell Structure and FunctiontrilucaNo ratings yet
- Bone SkullDocument80 pagesBone SkullKumarNo ratings yet
- Contra Indications To Electrical EpilationDocument30 pagesContra Indications To Electrical EpilationUzma KhanNo ratings yet
- Mechanical VentilationDocument12 pagesMechanical VentilationDoru VoicuNo ratings yet
- PHS 211 C4Document14 pagesPHS 211 C4metasynthronos748No ratings yet
- Sleep Deprivation Stem CaviteDocument57 pagesSleep Deprivation Stem CaviteLesley NaraNo ratings yet
- Systems-Heart Dissection Lab - Answer KeyDocument1 pageSystems-Heart Dissection Lab - Answer KeyGiorde PasambaNo ratings yet
- Respiratory Arrest Rescue BreathingDocument13 pagesRespiratory Arrest Rescue BreathingDJ Evan JulesNo ratings yet
- Anesthesia For Awake CraniotomyDocument13 pagesAnesthesia For Awake CraniotomyAhmad Naquiyuddin Bin ZakiNo ratings yet
- Pulmonary Function TestsDocument38 pagesPulmonary Function TestsMohamedSalahNo ratings yet
- Headache in ChildrenDocument34 pagesHeadache in Childrensai saiNo ratings yet
- Topic 6: Plant Structure & FunctionDocument36 pagesTopic 6: Plant Structure & FunctionChiangshiuan SooNo ratings yet
- ENA WB Worksheet 25 2Document4 pagesENA WB Worksheet 25 2Ng Li Xian50% (2)
- AmlodipineDocument9 pagesAmlodipineMA 09No ratings yet
- Human BIology PhysioEX Assignment 1Document2 pagesHuman BIology PhysioEX Assignment 1Peilu GanNo ratings yet
- American Thoracic Society: DyspneaDocument20 pagesAmerican Thoracic Society: DyspneaTrismegisteNo ratings yet
- Excitable Tissues: DR Joseph WabwireDocument38 pagesExcitable Tissues: DR Joseph WabwireJoseph WabwireNo ratings yet
- (MED1) 3.04 Approach To Hypertension (Dr. Bago-Azares)Document11 pages(MED1) 3.04 Approach To Hypertension (Dr. Bago-Azares)NoreenNo ratings yet
- Quiz 4Document6 pagesQuiz 4Andrew DarnelNo ratings yet
- Hemodynamic MonitoringDocument9 pagesHemodynamic MonitoringHernando CastrillónNo ratings yet
- NCP For HyperthermiaDocument3 pagesNCP For HyperthermiaNikael Patun-ogNo ratings yet
- Katzung - AutacoidsDocument23 pagesKatzung - AutacoidsKhairul AimanNo ratings yet
- AUTOPSY ReezuDocument16 pagesAUTOPSY ReezuBnB UsmleNo ratings yet
- Heartbeat Sequencing Colour by NumbersDocument5 pagesHeartbeat Sequencing Colour by NumbersKavs KitchensNo ratings yet
- CVPDocument33 pagesCVPbharti PatelNo ratings yet
- BplogDocument2 pagesBplogMonir AhamedNo ratings yet
- Anatomy and Physiology of The HeartDocument21 pagesAnatomy and Physiology of The HeartNina OaipNo ratings yet
- Neck Pain Exercises (Demonstration Presentation Assignment)Document5 pagesNeck Pain Exercises (Demonstration Presentation Assignment)Hardianty Andi Munawarah AbduhNo ratings yet
- Bioenergetics of Exercising HumansDocument26 pagesBioenergetics of Exercising HumansMasajes A DomicilioNo ratings yet
- A Soft Total Artificial Heart-First Concept Evaluation OnDocument11 pagesA Soft Total Artificial Heart-First Concept Evaluation OnSeyit Hamza ÇavgaNo ratings yet
- ARRHYTHMIADocument25 pagesARRHYTHMIAAsma MuhammadiNo ratings yet
- Acute Respiratory FailureDocument5 pagesAcute Respiratory FailureHoney Bee S. PlatolonNo ratings yet
- Gaseous Exchange: Short Question AnswersDocument5 pagesGaseous Exchange: Short Question AnswersNadeem ArainNo ratings yet