You might also like
- Filariasis: Causes, Tests, and Treatment OptionsFrom EverandFilariasis: Causes, Tests, and Treatment OptionsRating: 5 out of 5 stars5/5 (2)
- Assingment of ParasateDocument36 pagesAssingment of ParasateHibaaq AxmedNo ratings yet
- المحاضرة 11 و 12 مادة الطفيلياتDocument18 pagesالمحاضرة 11 و 12 مادة الطفيلياتdyabw6430No ratings yet
- Parasitic Inclusions in ErythrocytesDocument27 pagesParasitic Inclusions in ErythrocytesLian Marie ViñasNo ratings yet
- Plasmodium: 25/02/2019 Ss NghoshiDocument31 pagesPlasmodium: 25/02/2019 Ss NghoshiJohanna HaludiluNo ratings yet
- Malaria ىواسكرك كرابم ةلئان .د دادعاDocument87 pagesMalaria ىواسكرك كرابم ةلئان .د دادعاkoncoerrorNo ratings yet
- BIO3242 - Lecture 3Document86 pagesBIO3242 - Lecture 3NGOGA NISINGIZWE NESTORNo ratings yet
- Phylum Sporozoa - Exercise No 4Document4 pagesPhylum Sporozoa - Exercise No 4Justin JannatiNo ratings yet
- Protozoa. Sporozoa. Haemosporidia (The Malaria Parasites)Document22 pagesProtozoa. Sporozoa. Haemosporidia (The Malaria Parasites)Sharan MurugaboopathyNo ratings yet
- Unit 11. Blood and Tissue Coccidian (Apicomplexa)Document40 pagesUnit 11. Blood and Tissue Coccidian (Apicomplexa)Michael DawitNo ratings yet
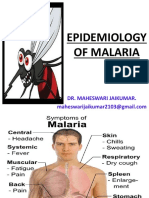
- Epidemiology of Malaria: Dr. Maheswari JaikumarDocument70 pagesEpidemiology of Malaria: Dr. Maheswari JaikumarBijay Kumar MahatoNo ratings yet
- MalariaDocument102 pagesMalariatummalapalli venkateswara rao100% (8)
- Lec 9 MalariaDocument42 pagesLec 9 MalariaMye AkmaNo ratings yet
- Lec 9 MalariaDocument42 pagesLec 9 MalariaMye AkmaNo ratings yet
- Protozoal Infections 29 April 2013Document87 pagesProtozoal Infections 29 April 2013Nive KojNo ratings yet
- Department of Zoology Govt. Degree College, Basohli: Plasmodium VivaxDocument16 pagesDepartment of Zoology Govt. Degree College, Basohli: Plasmodium VivaxRohon DasNo ratings yet
- Protozoal Infections: Immunity & InfectionDocument67 pagesProtozoal Infections: Immunity & InfectionalmiraerickaiNo ratings yet
- The Most Important Parasitic DiseaseDocument90 pagesThe Most Important Parasitic DiseaseAminath MeesanNo ratings yet
- Bio ProjectDocument13 pagesBio ProjectASAD RAHMANNo ratings yet
- Schistosoma LectureDocument10 pagesSchistosoma LectureSe YiNo ratings yet
- Blood Fluke Schistosoma HaematobiumDocument5 pagesBlood Fluke Schistosoma HaematobiumBuntukazi MapamelaNo ratings yet
- ParasiteDocument60 pagesParasiteJewan Ambadil SampulnaNo ratings yet
- MalariaDocument11 pagesMalariaHaritha ReddyNo ratings yet
- Introduction To: ParasitesDocument32 pagesIntroduction To: ParasitesJaznMonNo ratings yet
- MalariaDocument15 pagesMalariaEssa KhanNo ratings yet
- Major Bacteria Infecting The Hematology System 2. Major Parasites Infecting The Hematologic SystemDocument128 pagesMajor Bacteria Infecting The Hematology System 2. Major Parasites Infecting The Hematologic SystemƯớc Của BếttingNo ratings yet
- MalariaDocument28 pagesMalariaArie GradiyantoNo ratings yet
- Bone MarrowDocument72 pagesBone MarrowSumit PandyaNo ratings yet
- Malaria DiseaseDocument86 pagesMalaria DiseasevenusnurfatimahNo ratings yet
- 3rd Handout The Malarial ParasitesDocument4 pages3rd Handout The Malarial ParasitesPatrica Willyn B. DiosoNo ratings yet
- Major Bacteria Infecting The Hematology System 2. Major Parasites Infecting The Hematologic SystemDocument121 pagesMajor Bacteria Infecting The Hematology System 2. Major Parasites Infecting The Hematologic SystemƯớc Của BếttingNo ratings yet
- 5.1.3.2. Blood FlukesDocument43 pages5.1.3.2. Blood Flukestadele10100% (1)
- Plasm OdiumDocument23 pagesPlasm OdiumRabar Mohsin Abdulrahman MantikNo ratings yet
- Antimalarial DrugsDocument19 pagesAntimalarial Drugspallavi DiwareNo ratings yet
- The Trematodes (Flukes) Presented by Happy SimozuDocument93 pagesThe Trematodes (Flukes) Presented by Happy SimozuWilliam C ChishaNo ratings yet
- Malaria 141112210953 Conversion Gate02Document33 pagesMalaria 141112210953 Conversion Gate02shubham vermaNo ratings yet
- L09 MalariaDocument30 pagesL09 MalariaS sNo ratings yet
- Presentation 3Document19 pagesPresentation 3Gift Maganga100% (1)
- 417 PHL - 1st Lecture - 2021-StDocument32 pages417 PHL - 1st Lecture - 2021-StLama LNo ratings yet
- Jordan University Faculty of Dentistry DR Mohammad Al-Tamimi, MD, PHDDocument20 pagesJordan University Faculty of Dentistry DR Mohammad Al-Tamimi, MD, PHDDaniel AtiehNo ratings yet
- Presention On Trypanosoma Department of Zoology Sri Guru Granth Sahib World UniversityDocument22 pagesPresention On Trypanosoma Department of Zoology Sri Guru Granth Sahib World UniversityRamanpreet KaurNo ratings yet
- Parasitology - CestodesDocument23 pagesParasitology - CestodesJeth Roque GalleneroNo ratings yet
- Life Cycle, Pathogenicity, Causes, Symptoms and Control of LeishmaniaDocument24 pagesLife Cycle, Pathogenicity, Causes, Symptoms and Control of LeishmaniaAditi TanwarNo ratings yet
- Plasmodium Malariae Life CycleDocument33 pagesPlasmodium Malariae Life CycleNezly IderusNo ratings yet
- Izza Maryam 1910146066 Topic: Malaria Instructor Name: Dr. Ayesha AslamDocument12 pagesIzza Maryam 1910146066 Topic: Malaria Instructor Name: Dr. Ayesha AslamIzza MaryumNo ratings yet
- ParasitologyDocument15 pagesParasitologyVysakh P RNo ratings yet
- Parasites - SchistosomiasisDocument23 pagesParasites - SchistosomiasisSunil YadavNo ratings yet
- Schistosomes Parasite in HumanDocument27 pagesSchistosomes Parasite in HumanAnonymous HXLczq3No ratings yet
- Foundations in Microbiology: TalaroDocument74 pagesFoundations in Microbiology: Talaromertx013No ratings yet
- Vector Borne - PPTX 1Document140 pagesVector Borne - PPTX 1Nursing septemberNo ratings yet
- MalariaDocument38 pagesMalariaFamous manNo ratings yet
- MalariaDocument2 pagesMalariaROn ArellanoNo ratings yet
- 1 2lec General Amoebiasis 3Document11 pages1 2lec General Amoebiasis 3بلسم محمود شاكرNo ratings yet
- Blood & Tissue ProtozoaDocument81 pagesBlood & Tissue ProtozoaMoses Tamba MomohNo ratings yet
- Jordan University Faculty of Dentistry DR Mohammad Al-Tamimi, MD, PHDDocument20 pagesJordan University Faculty of Dentistry DR Mohammad Al-Tamimi, MD, PHDDaniel AtiehNo ratings yet
- Jordan University Faculty of Dentistry DR Mohammad Al-Tamimi, MD, PHDDocument20 pagesJordan University Faculty of Dentistry DR Mohammad Al-Tamimi, MD, PHDDaniel AtiehNo ratings yet
- MALARIA TEACHING BASICS by Dr.T.V.Rao MDDocument89 pagesMALARIA TEACHING BASICS by Dr.T.V.Rao MDtummalapalli venkateswara raoNo ratings yet
- Para Lec 3Document21 pagesPara Lec 3stpaulafamilyNo ratings yet
- Dr. Huda R. Sabbar Al-Anbar University College of Medicine: HaemoflagellatesDocument19 pagesDr. Huda R. Sabbar Al-Anbar University College of Medicine: HaemoflagellatesThunderNo ratings yet
- One Day Workshop Yums: - Tissue and Blood Protozoan DiseasesDocument47 pagesOne Day Workshop Yums: - Tissue and Blood Protozoan DiseasesAndre KerenNo ratings yet
- Previouses PharmaceuticsDocument6 pagesPreviouses PharmaceuticsMalkhatibNo ratings yet
- Emergency ChildbirthDocument8 pagesEmergency ChildbirthMalkhatibNo ratings yet
- Skeletal System InjuriesDocument24 pagesSkeletal System InjuriesMalkhatibNo ratings yet
- Clinical ChemistryDocument6 pagesClinical ChemistryMalkhatibNo ratings yet
- Metabolic BiochemistryDocument6 pagesMetabolic BiochemistryMalkhatibNo ratings yet
- Bites and StingsDocument14 pagesBites and StingsMalkhatibNo ratings yet
- Chest, Abdomen and Pelvis InjuriesDocument27 pagesChest, Abdomen and Pelvis InjuriesMalkhatibNo ratings yet
- Metabolic BiochemistryDocument6 pagesMetabolic BiochemistryMalkhatibNo ratings yet
- :خيراتلا 24 / 1 / 2018 لاالاا hghhgh لولاا: Unresponsive victim not breathingDocument7 pages:خيراتلا 24 / 1 / 2018 لاالاا hghhgh لولاا: Unresponsive victim not breathingMalkhatibNo ratings yet
- Test BankDocument10 pagesTest BankMalkhatibNo ratings yet
- n.Bioch.2009-B (2) - 1Document12 pagesn.Bioch.2009-B (2) - 1MalkhatibNo ratings yet
- If The Physician Diagnoses The Patient Wrongly He Would Get BeatenDocument4 pagesIf The Physician Diagnoses The Patient Wrongly He Would Get BeatenSheen GabatoNo ratings yet
- 2.2 First Aid - Basic First Aid and Resuscitation - Participant HandoutDocument3 pages2.2 First Aid - Basic First Aid and Resuscitation - Participant HandoutEva ChristinaNo ratings yet
- ADaM Public Exercises Answers 2018 04 05Document35 pagesADaM Public Exercises Answers 2018 04 05wei chiNo ratings yet
- Cellulitis: Definition, Etiology, and Clinical Features: ReviewDocument10 pagesCellulitis: Definition, Etiology, and Clinical Features: ReviewAnonymous 8k5cuCvOOYNo ratings yet
- Gerson - The Little Enema BookDocument36 pagesGerson - The Little Enema BookBruno GonçalvesNo ratings yet
- Acupuntura - Puntos ImportantesDocument14 pagesAcupuntura - Puntos ImportantessanthigiNo ratings yet
- Mobility and ImmobilityDocument37 pagesMobility and ImmobilityAndrea Huecas Tria100% (2)
- Retic MethodDocument18 pagesRetic MethodFaty DearNo ratings yet
- Dexmedetomidine - Drug Information - UpToDateDocument21 pagesDexmedetomidine - Drug Information - UpToDateRicardo Ortiz NovilloNo ratings yet
- Diane Kazer Loving On Our LymphDocument22 pagesDiane Kazer Loving On Our LymphKátia BárbaraNo ratings yet
- Bmi Lab Viva QuestionDocument7 pagesBmi Lab Viva QuestionnijafancyNo ratings yet
- A Sinister Cause For Recurrent Syncope: Metastatic Parapharyngeal Space TumorDocument4 pagesA Sinister Cause For Recurrent Syncope: Metastatic Parapharyngeal Space TumorasclepiuspdfsNo ratings yet
- Group Therapy.Document20 pagesGroup Therapy.aliatia751No ratings yet
- D - Guideline On Number of Embryos To Transfer During IVF ICSI - Stakeholder ReviewDocument135 pagesD - Guideline On Number of Embryos To Transfer During IVF ICSI - Stakeholder Reviewshobhitbhargava39No ratings yet
- Asge Primer 2017 Pgs117 125 Single PageDocument9 pagesAsge Primer 2017 Pgs117 125 Single PageMani KandanNo ratings yet
- AMG Curs 3Document2 pagesAMG Curs 3Maria PalNo ratings yet
- Body Fluids and Circulation Class 11 Study Notes: BloodDocument7 pagesBody Fluids and Circulation Class 11 Study Notes: BloodTUSHAR DASHNo ratings yet
- Part B - Health Facility Briefing & Design 55Document15 pagesPart B - Health Facility Briefing & Design 55Mudita PiseNo ratings yet
- Absen Edit 2019Document29 pagesAbsen Edit 2019Judika ThampNo ratings yet
- Inside The Human BodyDocument1 pageInside The Human BodyKaravanNo ratings yet
- 4333445492022-10-25T16 28 16.773Document6 pages4333445492022-10-25T16 28 16.773Nina JordanNo ratings yet
- Acute MedicineDocument5 pagesAcute MedicinesuggaplumNo ratings yet
- ECG Taking Checklist-Ez VersionDocument2 pagesECG Taking Checklist-Ez VersionKeisha Bartolata100% (1)
- The Spanish Flu Pandemic of 1918Document5 pagesThe Spanish Flu Pandemic of 1918jellNo ratings yet
- Threshold and RecruitmentDocument16 pagesThreshold and RecruitmentShamaine Anne SalvadorNo ratings yet
- PhysioEx Exercise 7 Activity 1Document6 pagesPhysioEx Exercise 7 Activity 1Jorge CuevaNo ratings yet
- SteatorrheaDocument43 pagesSteatorrheaJohnRobynDiezNo ratings yet
- Angels ResumeDocument4 pagesAngels Resumeapi-274792391No ratings yet
- Hypertensive Disorders in PregnancyDocument6 pagesHypertensive Disorders in PregnancyLuiciaNo ratings yet
- Reading The Brain by Caroline MarkolinDocument2 pagesReading The Brain by Caroline MarkolinCoraKiri100% (1)