You might also like
- Psychological ResilienceDocument37 pagesPsychological Resiliencedgavrile100% (3)
- Aaq - Adolescent Attachment QuestionnaireDocument8 pagesAaq - Adolescent Attachment QuestionnaireDesi Phyki100% (2)
- Causes of Academic Stress On Students by HassanDocument16 pagesCauses of Academic Stress On Students by HassanM Hassan Tunio100% (1)
- Child Marriage PresentationDocument26 pagesChild Marriage Presentationditha puspitaNo ratings yet
- Medical Surgical NursingDocument6 pagesMedical Surgical NursingzemmiphobiaNo ratings yet
- Nursing Practice IDocument69 pagesNursing Practice IDon MarcusNo ratings yet
- Core Clinical ProblemsDocument57 pagesCore Clinical ProblemsPatriciaChRistianiNo ratings yet
- Ddslab RX CNBDocument1 pageDdslab RX CNBstartupsagar16No ratings yet
- 4Document1 page4alnoel tordillaNo ratings yet
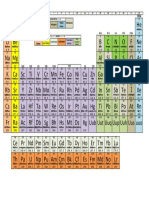
- New Periodic TableDocument1 pageNew Periodic Tableharpal_abhNo ratings yet
- Az 1575Document41 pagesAz 1575Arleig Augusto de MatosNo ratings yet
- Scheda MDS02 PDFDocument1 pageScheda MDS02 PDFThomas RiatoNo ratings yet
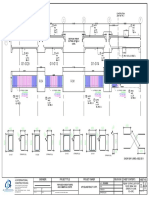
- Poligonal 20 - A3Document1 pagePoligonal 20 - A3ABDIASmamanigallegosNo ratings yet
- 2 Kiks-ModelDocument1 page2 Kiks-ModelAndeNo ratings yet
- Denah Lantai 1 - Gedung Fis Um: Shaft Shaft Lift Barang Shaft Shaft Lift BarangDocument1 pageDenah Lantai 1 - Gedung Fis Um: Shaft Shaft Lift Barang Shaft Shaft Lift BarangRegi WahyuNo ratings yet
- Denah Lantai Basement & 1Document1 pageDenah Lantai Basement & 1Ivan GeovaniNo ratings yet
- Affri enDocument56 pagesAffri enDeepak KumarNo ratings yet
- Relative Material HardnessDocument1 pageRelative Material HardnessrizkiNo ratings yet
- Elevation Isometric View: Section Aa'Document2 pagesElevation Isometric View: Section Aa'44 khushi DhuriNo ratings yet
- Schwarzkopf Mar Apr 2014 PromosDocument24 pagesSchwarzkopf Mar Apr 2014 PromosVansh LuthrraNo ratings yet
- Soldering Plating Stonesetting ENDocument16 pagesSoldering Plating Stonesetting ENAsia MarinoNo ratings yet
- Metal Composition PDFDocument3 pagesMetal Composition PDFVijendra Singh JhalaNo ratings yet
- Group Housing: North Pooja Yadav Ar. Manish GuptaDocument1 pageGroup Housing: North Pooja Yadav Ar. Manish GuptavijetaNo ratings yet
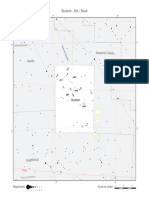
- Scutum - SCT - Scuti: Serpens Cauda AquilaDocument1 pageScutum - SCT - Scuti: Serpens Cauda Aquilaefrain dalmagroNo ratings yet
- R1 Donor Cut Tower: Waste Hexane Drum Item No. D-718Document1 pageR1 Donor Cut Tower: Waste Hexane Drum Item No. D-718NoppolNorasriNo ratings yet
- JardinDocument1 pageJardinHIND SANOGONo ratings yet
- Khoidaudam 2Document1 pageKhoidaudam 2tai taiNo ratings yet
- 5322-01-01 - Rigla 1Document1 page5322-01-01 - Rigla 1CezzarinoNo ratings yet
- Material P-Number - Chai (Rev3)Document3 pagesMaterial P-Number - Chai (Rev3)Chaitanya Sai TNo ratings yet
- Project 1 - 57 Jean Street, Seven Hills - Site SurveyDocument1 pageProject 1 - 57 Jean Street, Seven Hills - Site SurveyAlbert LiuNo ratings yet
- Worm IntroductionDocument4 pagesWorm IntroductionRoby MastreNo ratings yet
- Gold Note: 30 October 2007Document10 pagesGold Note: 30 October 2007anamq1No ratings yet
- 2014MAFord CatalogCountersinksDocument25 pages2014MAFord CatalogCountersinksBeto CovasNo ratings yet
- Khushi Dhuri Special Skills Workshop 2000701044Document3 pagesKhushi Dhuri Special Skills Workshop 200070104444 khushi DhuriNo ratings yet
- A340 Parker GasketsDocument6 pagesA340 Parker GasketsjckfNo ratings yet
- Spheroidal Graphite (Nodular) Cast Iron:: Product Type Grade of Product Sub GradeDocument5 pagesSpheroidal Graphite (Nodular) Cast Iron:: Product Type Grade of Product Sub GradeAnonymous iztPUhIiNo ratings yet
- Lever Style Plungers Locking Non Locking Stainless SteelDocument3 pagesLever Style Plungers Locking Non Locking Stainless SteelPedro CaraveoNo ratings yet
- 364+650 Proposed PlanDocument3 pages364+650 Proposed PlanVivek G. AbhyankarNo ratings yet
- Material Design Properties For Structural Steel S235, S275, S355, S420, S450, S460 According To EN1993-1-1 3.2.6Document2 pagesMaterial Design Properties For Structural Steel S235, S275, S355, S420, S450, S460 According To EN1993-1-1 3.2.6yusuf akkuşNo ratings yet
- Winter MTB Tour/ BMX Otjiwarongo Winter MTB Tour/ BMX OtjiwarongoDocument2 pagesWinter MTB Tour/ BMX Otjiwarongo Winter MTB Tour/ BMX Otjiwarongojohanita de waalNo ratings yet
- EN-Dimensional-and-shape-tolerances-according EN 10131:2006Document6 pagesEN-Dimensional-and-shape-tolerances-according EN 10131:2006Tri-Sure More Than ClosuresNo ratings yet
- SRC 2018-2019Document8 pagesSRC 2018-2019Dina CalungsodNo ratings yet
- Ann Whs ElevationsDocument1 pageAnn Whs Elevationssimbwa2016No ratings yet
- GudangDocument1 pageGudangAji PrayogaNo ratings yet
- Citymap - Textured - Modified Copy03Document1 pageCitymap - Textured - Modified Copy03GabrielNo ratings yet
- Residência - Fernanda de Lima Sobreiro: FURO R100Document1 pageResidência - Fernanda de Lima Sobreiro: FURO R100MARIONo ratings yet
- TW BF 01 - Barstock Flanged Type Thermowell (Straight) : TWBF - 01Document17 pagesTW BF 01 - Barstock Flanged Type Thermowell (Straight) : TWBF - 01Mangesh MohiteNo ratings yet
- Adr PC ZZ S 22 01 000Document1 pageAdr PC ZZ S 22 01 000mechanasNo ratings yet
- Aluminum Selecti TTQVGDocument1 pageAluminum Selecti TTQVGa.kamyabiNo ratings yet
- Autocad Sample WorkDocument1 pageAutocad Sample WorkrobinNo ratings yet
- Rebar Physical PropertiesDocument2 pagesRebar Physical PropertiesJuan RodriguezNo ratings yet
- ABS Grade AH36, ABS Grade EH36, ABS Grade DH36, ABS Grade FH36 Steel Plate For Shipbuidling and RepairingDocument2 pagesABS Grade AH36, ABS Grade EH36, ABS Grade DH36, ABS Grade FH36 Steel Plate For Shipbuidling and Repairingaini lutunaNo ratings yet
- Katalog-KTS en 2018 14Document1 pageKatalog-KTS en 2018 14Alomaki KismaNo ratings yet
- FPD 2020Document23 pagesFPD 2020franchi-paoloNo ratings yet
- SV 23 0512Document1 pageSV 23 0512Simon CelestinaNo ratings yet
- RJTT PDFDocument34 pagesRJTT PDFReanaldy Ibrahim Masudi PutraNo ratings yet
- Rhcaeta: Structural Design Calculation Sheet For Block of Duplex FOR MR & Mrs Adokiye Precious CharlesDocument17 pagesRhcaeta: Structural Design Calculation Sheet For Block of Duplex FOR MR & Mrs Adokiye Precious CharlesEze NonsoNo ratings yet
- Steel Resource Guide LTR - 230914 - 091953Document6 pagesSteel Resource Guide LTR - 230914 - 091953MarllonDiluNo ratings yet
- Wuxi Lekanghao Steel Co., LTDDocument3 pagesWuxi Lekanghao Steel Co., LTDRicardo Rivas RemonNo ratings yet
- Matriz de Ensaios, Ligas AlbaDocument4 pagesMatriz de Ensaios, Ligas AlbaMarco A. R. JimenesNo ratings yet
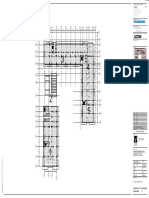
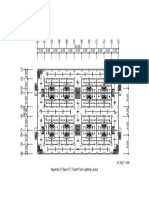
- Sample of Lighting Layout For High Rise BuildingDocument1 pageSample of Lighting Layout For High Rise BuildingLester SarmientoNo ratings yet
- Furnace Coil DrawingDocument1 pageFurnace Coil DrawingpurNo ratings yet
- OM Assignment 2 - 22MBAB52Document3 pagesOM Assignment 2 - 22MBAB5222MBAB53 ThiruchittambalamNo ratings yet
- Kebutuhan Obat Jiwa Tahun 2022Document3 pagesKebutuhan Obat Jiwa Tahun 2022PUSKESMAS ROKAN 2No ratings yet
- Orifice Plate With Carrier Ring Assembly PDFDocument1 pageOrifice Plate With Carrier Ring Assembly PDFRajeev ChaudNo ratings yet
- Orifice Plate With Carrier Ring Assembly PDFDocument1 pageOrifice Plate With Carrier Ring Assembly PDFaravindNo ratings yet
- Social Psychology: Changing Attitudes Through PersuationDocument7 pagesSocial Psychology: Changing Attitudes Through PersuationChin SilverNo ratings yet
- Hoklas SC-26Document9 pagesHoklas SC-26YY CheungNo ratings yet
- Chapter 2 WorksheetDocument3 pagesChapter 2 WorksheetjessNo ratings yet
- ANTIVIRALEDocument4 pagesANTIVIRALEVladStefanescuNo ratings yet
- Made 407Document5 pagesMade 407tu nguyen thiNo ratings yet
- Tce 3Document6 pagesTce 3Yasser Mahdi AbdelhamidNo ratings yet
- Cerebellar Dizziness and Vertigo - Etiologies, Diagnostic and TratmentDocument10 pagesCerebellar Dizziness and Vertigo - Etiologies, Diagnostic and Tratmentrafael rocha novaesNo ratings yet
- United States District Court Northern District of New YorkDocument22 pagesUnited States District Court Northern District of New YorkRicca PrasadNo ratings yet
- Ergonomics of Minimally Invasive SurgeryDocument9 pagesErgonomics of Minimally Invasive SurgeryFlaviu Ionuț FaurNo ratings yet
- HLTH 101 Research PaperDocument9 pagesHLTH 101 Research Paperapi-566289467No ratings yet
- DE Thi HKI - 2019-2020 - TN - 11DDocument7 pagesDE Thi HKI - 2019-2020 - TN - 11DChi MaiNo ratings yet
- База Тестів на ПМК2 з анатомії УКР і АНГDocument183 pagesБаза Тестів на ПМК2 з анатомії УКР і АНГAnzhelika BondarenkoNo ratings yet
- Instruction Manual: Autoclaves & SterilizersDocument61 pagesInstruction Manual: Autoclaves & SterilizersSàkâtã ÁbéŕàNo ratings yet
- Perceived Stress ScaleDocument3 pagesPerceived Stress Scalevinn sam phangNo ratings yet
- National Health AccountsDocument4 pagesNational Health AccountsMyat MinNo ratings yet
- Vander Ver Joyce Literature ReviewDocument4 pagesVander Ver Joyce Literature ReviewJoyce NicoleNo ratings yet
- Understanding The Construction of Behavior in Smartphone 2023 Addictive BeDocument9 pagesUnderstanding The Construction of Behavior in Smartphone 2023 Addictive BejohnhansonNo ratings yet
- Inflammatory Bowel DiseaseDocument3 pagesInflammatory Bowel DiseaseDivine ParagasNo ratings yet
- Prof Erica-Global HemovigilanceDocument38 pagesProf Erica-Global HemovigilanceHandoko HalimNo ratings yet
- Employee BenefitsDocument28 pagesEmployee BenefitsJedea Joy LactaoenNo ratings yet
- Catálogo de Soluções Hospitalares - COMPANY PRESENTATIONDocument34 pagesCatálogo de Soluções Hospitalares - COMPANY PRESENTATIONMarlos Vanni BorbaNo ratings yet
- Unit 301 Understanding The Principles and Practices of AssessmentDocument32 pagesUnit 301 Understanding The Principles and Practices of AssessmentحيدرالركابيNo ratings yet
- Equipment Booking Form 1Document5 pagesEquipment Booking Form 1api-479589840No ratings yet