Professional Documents
Culture Documents
Fractures of The Base of The Fifth Metatarsal.4
Uploaded by
RAHUL CHOUDHARIOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Fractures of The Base of The Fifth Metatarsal.4
Uploaded by
RAHUL CHOUDHARICopyright:
Available Formats
|
Fractures of the Base of the Fifth
Metatarsal Bone
A Critical Analysis Review
Downloaded from http://journals.lww.com/jbjsreviews by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZkD2PQTEnA3Z5k45NO+rAW3MozZ+QL8NPB6EWHTil9dgxc3V4BTfMcj09FIgM6S6/NBzg5ThlhF44kswtoLci5tLXTJedyj2QthqOc27xq/h0ud5iNHp+nk85Lzb23fod on 11/22/2021
Kamila Bušková, MD Abstract
» Fractures of the proximal fifth metatarsal (PFMT) are one of the most
Jan Bartonı́ček, MD, DSc
common foot injuries, accounting for 61% to 78% of all foot fractures,
Stefan Rammelt, MD, PhD but full consensus on their classification, diagnosis, and treatment has
not yet been reached.
» The most commonly accepted classification is that of Lawrence and
Botte, who divided the location of PFMT fractures into 3 zones with
respect to their healing potential.
» Avulsion fractures of the tuberosity of the base (zone 1) generally
heal well, and nonoperative treatment is commonly recommended.
» Internal fixation may be considered for displaced fractures that
extend into the fourth-fifth intermetatarsal joint (zone 2) as well as for
nondisplaced fractures in athletes or high-demand patients, with the
aims of reducing the healing time and expediting return to sport or
work.
» Stress fractures of the proximal diaphysis (zone 3) are preferably
treated operatively, particularly in the presence of signs of delayed
union. With nonoperative treatment, supportive measures such as
ultrasonography or external/extracorporeal shockwave therapy have
been demonstrated to have limited potential for the enhancement of
fracture-healing.
M
anagement of fractures of 1927, Carp25 found delayed union in 4 of
the proximal fifth meta- 21 cases of PFMT fracture and proposed an
tarsal (PFMT) has been association with the particular blood supply
intensively debated in of the fifth metatarsal as described in detail
the literature since the 1970s1-6. Although by Lexer et al. in 190426. In 1960, Stewart
the first case series of PFMT fractures was published a series of 51 patients with a
published .100 years ago7,8, no universal PMFT fracture1. Several larger studies fol-
consensus has yet been reached on their lowed between 1975 and 19842-6. In 1993,
classification, diagnosis, and treatment9-23. Lawrence and Botte divided the location of
In 1847, Malgaigne was probably the PFMT fractures into 3 zones with respect to
first surgeon who briefly mentioned a their healing potential27, a system that has
PFMT fracture24. In 1902, Robert Jones been commonly accepted since.
described 6 such fractures according to
radiographs, including his own injury that Anatomy
he had sustained while dancing; hence, the The fifth metatarsal forms the lateral border
eponym a “Jones (or dancer) fracture.”7 In of the forefoot. Its robust proximal aspect
COPYRIGHT © 2021 BY THE
JOURNAL OF BONE AND JOINT Disclosure: The Disclosure of Potential Conflicts of Interest forms are provided with the online
SURGERY, INCORPORATED version of the article (http://links.lww.com/JBJSREV/A750).
JBJS REVIEWS 2021;9(10) :e21.00010 · http://dx.doi.org/10.2106/JBJS.RVW.21.00010 1
| Fractures of the Base of the Fifth Metatarsal Bone
receives the attachments of multiple plantar (Lisfranc) ligament originates the tuberosity with respect to radio-
ligaments and muscles, and it is the end from the fifth metatarsal base in 62% of graphic appearance and healing poten-
part of Hellpap’s so-called “supination patients37. tial, which was divided into 3 types
line”28-31. The fifth metatarsal is formed The fifth metatarsal base is sup- without explicitly using the term stress
by the base, the shaft, the neck, and the plied by the terminal branches of the fracture6:
head32. The base is the prominent anterior and posterior tibial arteries,
1. Type I: early (a narrow fracture
proximal part that forms a tuberosity on specifically through dorsal metatarsal
line and absence of intramedullary
its lateral aspect, also called the styloid arteries arising from the lateral plantar
sclerosis or cortical reaction),
process. The tuberosity markedly over- artery and the plantar metatarsal arteries
2. Type II: delayed union (widening
laps the lateral aspect of the cuboid. The that are derived from the arcuate artery
of the fracture line with bone
proximal part of the base carries a tri- or the dorsalis pedis artery26,38,39. The
resorption and sclerosis), and
angular articular facet for the cuboid. On tuberosity is supplied by the metaphy-
3. Type III: nonunion (a wide frac-
the medial surface, there is an oval seal arteries. The shaft is supplied by a
ture line, a periosteal reaction,
articular facet that articulates with the nutrient artery arising from the fourth
and complete obliteration of the
lateral articular facet of the fourth met- plantar artery. This artery enters the fifth
medullary canal).
atarsal base. A groove for the abductor metatarsal from the medioplantar
digiti minimi muscle lies on the plantar aspect, which is approximately 2 cm In 1993, Lawrence and Botte27
surface. The joint capsule to the cuboid distal to the tuberosity, and provides a published a classification based on the
is reinforced by relatively thin dorsal and retrograde blood supply to the proximal location of the fracture line (Fig. 2):
plantar tarsometatarsal ligaments33,34. metaphysis. This creates a vascular
1. Tuberosity avulsion fracture (zone
The joint to the fourth metatarsal base is watershed area in the metaphyseal-
1): an acute fracture exiting
stabilized by dorsal, interosseous, and diaphyseal region that is considered a
proximal to the fourth-fifth
plantar intermetatarsal ligaments35. predisposition for delayed fracture-
intermetatarsal joint, frequently
Recently, a lateral Lisfranc ligament has healing in this zone40,41. The base of the
involving the cuboid-metatarsal
been described; it spans from the fifth to fifth metatarsal is the site of ramification
joint,
the second metatarsal base on the plantar of the sural nerve42,43.
2. Jones fracture (metaphyseal-
aspect and blends with the long plantar Fractures and nonunions of the
diaphyseal: zone 2): an acute
ligament, thus stabilizing both the longi- fifth metatarsal base must be distin-
fracture passing transversely or
tudinal and transverse arches of the foot36. guished from accessory bones such as the
obliquely through the fifth met-
All 3 of the articulating bones are part of os peroneum44 and the os vesalianum45.
atarsal base to the fourth-fifth
the lateral pillar of the foot (Fig. 1).
intermetatarsal joint, and
The peroneus brevis tendon atta- Classification
3. Proximal diaphyseal stress fracture
ches to the dorsolateral surface of the In 1916, Tanton developed the first
(zone 3): a transverse fracture line
tuberosity. The peroneus tertius tendon binary classification, dividing PFMT
passing distal to the fourth-fifth
attaches to its dorsal surface, just distal to fractures into fractures of the base (1°)
intermetatarsal joint.
the peroneus brevis tendon27,33,34. The and fractures of the styloid (2°)46. Sim-
plantar surface receives insertions of the ilar classifications were subsequently At the proximal metaphyseal-
lateral band of the plantar aponeurosis presented by Stewart in 19601 and diaphyseal junction, this classification
and the terminal fibers of the long Dameron in 19752. distinguishes between traumatic (zone
plantar ligament and is the site of origin In 1984, Torg et al. published a 2) and stress (zone 3) fractures. As both
of the flexor digiti minimi. The lateral classification of PFMT fractures distal to are typically nondisplaced and have a
Fig. 1
Figs. 1-A and 1-B Anatomy of the fifth meta-
tarsal base. Fig. 1-A Attachments of the pero-
neal muscles. Fig. 1-B Articulations of the
base of the fifth metatarsal. Cu 5 cuboid,
PB 5 peroneus brevis, PT 5 peroneus tertius,
4. mtt 5 fourth metatarsal, 5. mtt 5 fifth
metatarsal, red arrow 5 cuboid-metatarsal liga-
ment, and yellow arrow 5 intermetatarsal
ligament.
2 OCTOBER 2021 · VOLUME 9, ISSUE 10 · e 21.00010
Fractures of the Base of the Fifth Metatarsal Bone |
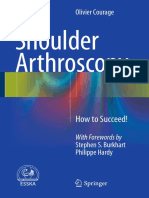
Fig. 2
Lawrence and Botte classification of fractures
of the proximal fifth metatarsal on a radio-
graph (Fig. 2-A) and an anatomical specimen
(Fig. 2-B). I 5 zone 1 (tuberosity fractures), II
5 zone 2 (Jones fractures), and III 5 zone 3
(stress fractures of the fifth metatarsal base).
similar poor healing potential, many Epidemiology forefoot adduction as risk factors for
authors have called this discrimination PFMT fractures account for 61% to sustaining a Jones fracture68.
into question and refer to all fractures of 78% of all foot fractures56-63. The Fractures of the metaphyseal-
the metaphysis and proximal shaft as reported rates range from 46% to 73% diaphyseal junction beyond the fourth-
Jones fractures, thereby returning to the in zone 1, 14% to 39% in zone 2, and fifth intermetatarsal joint (zone 3) are
simple classifications of Tanton and 8% to 15% in zone 3. In professional typically stress fractures. During normal
football players, the incidence of PFMT walking, the lateral aspect of the foot is
Dameron46-50. Others hold that acute
stress fractures has been calculated to be exposed to a substantial load; the con-
fractures (zones 1 and 2) have a similar
0.04 injuries per 1,000 hours of expo- centration of the load at the
prognosis and therefore need not be
sure. Therefore, a team of 25 players metaphyseal-diaphyseal junction also is
differentiated51,52. enhanced by the attachment of the per-
Overall, there is considerable con- might expect such a fracture to occur
oneal muscles and the hinge that is
fusion about the nomenclature of every fifth season64.
provided by the fourth-fifth intermeta-
PFMT fractures, particularly the term tarsal ligaments2,5,33,66. Risk factors
Mechanism of Injury
“Jones fracture,” which is frequently include hindfoot varus alignment69,70,
Tuberosity fractures (zone 1) are caused
used for acute fractures in zone 2 and metatarsus adductus68, and pes cavus, as
by avulsion resulting from the pull of the
stress fractures in zone 3, thereby mak- well as neuropathic conditions71-73.
lateral band of the plantar fascia29,33,65.
ing multiple studies difficult to interpret
These “tennis fractures” typically occur
and compare. In the original report by Diagnosis
after a misstep or a fall with the foot in
Jones7, the 4 images demonstrated at There are several steps in the diagnosis of
supination, adduction, and plantar
least 2, if not 3, different fracture pat- a PFMT fracture, which may include a
flexion2,3,49,58,66. The pull of the per-
terns50,53. In our article, we use the term detailed history and physical examina-
oneus brevis tendon may further dis- tion, radiographs, computed tomogra-
“Jones fracture” exclusively for acute place these fractures33,67. phy (CT), magnetic resonance imaging
fractures that are in zone 2. Jones fractures (zone 2) are acute (MRI), ultrasonography, and bone
Fractures and dislocations at the injuries that are believed to be caused scintigraphy.
fifth metatarsal base may also occur in mainly by an adduction force to the During the history-taking, patients
the wake of tarsometatarsal (Lisfranc) forefoot with the ankle in plantar flex- are questioned about the injury mecha-
injuries and must be classified accord- ion. The result is a transverse fracture, nism, any previous injuries, the intensity
ingly54. Injuries to the lateral tarsomet- sometimes with medial comminution1, of previous activities, and the nature and
27
atarsal joints are beyond the scope of this . In a case-control study of 51 athletes, onset of pain. Systemic metabolic, neu-
review and discussions may be found Karnovsky et al. identified a long, rologic, rheumatologic, or oncologic
elsewhere55. straight, narrow fifth metatarsal and disease should be ruled out.
OCTOBER 2021 · VOLUME 9, ISSUE 10 · e21.00010 3
| Fractures of the Base of the Fifth Metatarsal Bone
TABLE I Recommendations for Care
Recommendation
Recommendation Grade*
MRI is highly efficient in diagnosing stress fractures before they are visible on radiographs. A
Avulsion fractures of the tuberosity (zone 1) have good healing potential, and nonoperative treatment is generally B
recommended.
Internal fixation may be considered for displaced fractures extending into the fourth-fifth intermetatarsal joint (zone 2) B
and for nondisplaced fractures in athletes or high-demand patients, with the aim to reduce the time to heal and
expedite return to sport or work.
Stress fractures at the proximal metaphysis (zone 3) are preferably treated operatively. The most commonly used B
method is implantation of an intramedullary screw.
With nonoperative treatment, supportive measures like ultrasonography and external/extracorporeal shockwave B
therapy have demonstrated some value for the enhancement of fracture-healing.
*According to Wright190, grade A indicates good evidence (Level-I studies with consistent findings) for or against recommending intervention; grade B,
fair evidence (Level-II or III studies with consistent findings) for or against recommending intervention; grade C, poor-quality evidence (Level-IV or V
studies with consistent findings) for or against recommending intervention; and grade I, insufficient or conflicting evidence not allowing a recom-
mendation for or against intervention.
With acute fractures, the clinical Principles of Treatment ing the articular facet to the cuboid13,52,
94,98-100
findings include limping with offloading Despite an ever-increasing number of . One prospective randomized
of the lateral edge of the foot, pain on clinical studies, there is limited eviden- study comparing nonoperative and
weight-bearing and inversion, swelling, tial guidance regarding the choice of operative treatment in zone-1 fractures
hematoma, and tenderness on palpation PFMT fracture treatment (Table I). A with displacement of $2 mm did not
at the fifth metatarsal base. wide array of nonoperative and operative reveal any significant difference in visual
The basic radiographic examina- methods is available. Treatment must analog scale (VAS) pain and American
tion consists of anteroposterior, 30° be tailored individually to the fracture Orthopaedic Foot & Ankle Society
oblique, and lateral radiographs of the pattern, the displacement, the local con- (AOFAS) scores98. Another prospective
foot. Stress fractures are usually seen as ditions, and the health status and func- randomized study in young adults and
radiolucent zones on radiographs at a tional demand of each patient. Abnormal athletes found significantly higher (p ,
minimum of 10 days after the onset of metabolic or hormonal conditions like 0.05) AOFAS scores at 6 weeks, lower
symptoms. Only 9% of cases are vitamin D deficiency, osteoporosis, VAS scores at 12 months, and an earlier
detected on the initial radiographs74,75. poorly controlled diabetes, and thyroid return to work after minimally invasive
CT is indicated with complex hormone deficiency should be treated screw fixation when compared with
intra-articular fractures, including lat- simultaneously to improve the chance nonoperative treatment in a cast101.
eral Lisfranc injuries. CT also may be of healing80-83. In cases of severe Similar results were seen in a non-
used to evaluate the phase of healing of underlying foot and ankle deformities, randomized prospective cohort study in
these fractures76. especially cavovarus or equinovarus in athletes102. Nonunion after nonopera-
MRI is highly efficient in diag- recalcitrant PFMT nonunions, correc- tive treatment that required revision
nosing stress fractures before they are tive osteotomies or fusions should be surgery has been reported repeatedly in
visible on radiographs and in assessing considered70,84. athletes103-105. Based on these data,
the surrounding tissues74,75. operative treatment has been advocated
Ultrasonography is less demanding Treatment of Tuberosity Fractures— for athletes and young high-demand
to perform and more readily available Zone 1 patients with displaced tuberosity
than MRI. In addition to associated soft- Nonoperative Treatment fractures.
tissue alterations, ultrasonography may Avulsion fractures of the tuberosity have Nonoperative treatment is based
demonstrate early periosteal reactions good healing potential, and nonopera- on the RICE (rest, ice, compression, and
that accompany a stress fracture77,78. tive treatment is generally recom- elevation) regimen. Most authors allow
Bone scintigraphy, using the radi- mended53. This is particularly true for weight-bearing as tolerated immedi-
onuclide isotope technetium-99m extra-articular and nondisplaced frac- ately after the injury. The foot is pro-
(99mTc), was a former gold standard in tures2,12,51,85-97. In the nonathletic tected with various types of bandages,
the diagnosis of stress fractures, but has a population, excellent results with union braces, hard-soled or cast shoes, air-
lower sensitivity and specificity, rates of 100% have been reported for cast walking boots, or below-the-knee
although a lower cost, than MRI79. displaced fractures and fractures involv- casts2,52,86,89,91,93,95-97. Better
4 OCTOBER 2021 · VOLUME 9, ISSUE 10 · e 21.00010
Fractures of the Base of the Fifth Metatarsal Bone |
Fig. 3
Figs. 3-A through 3-D Internal fixation of tuberosity (zone-1) fractures with tension-band wiring (Fig. 3-A), a locking compression plate (LCP, or hook plate) for the distal aspect
of the ulna (Fig. 3-B), an intramedullary screw (Fig. 3-C), and a headless screw (Fig. 3-D).
functional outcomes have been exceeding 2 to 3 mm or separation of recently, anchors125 are available. In a
achieved with the use of an elastic ban- .30% of the joint surface between the biomechanical study, a single 4.0-mm
dage or a walking brace than with cuboid and fifth metatarsal, particularly bicortical partially threaded cancel-
immobilization in a short leg cast56,87,88, in athletes and high-demand patients lous screw was significantly (p , 0.02)
92,96,97,106
. In a recent prospective ran- and in fractures with wide fragment more stable than a tension-band
domized trial, the time to return to displacement, resulting in soft-tissue wire construct for avulsion fracture
preinjury activity was significantly incarceration56,76,85,101,103,108-110. fixation109. A bicortical screw is bio-
shorter when patients were treated with Options for internal fixation include mechanically more stable than an
use of a hard-soled shoe than after Kirschner wires111,112, simple intraosse- intramedullary screw126.
treatment with a short leg cast107. ous wire fixation30,113, and tension-band Opinions vary on postoperative
wiring alone76,109,114 or in combination protection and weight-bearing. Hei-
Operative Treatment with interfragmentary lag screws115,116. neck et al. recommended partial
Numerous authors have proposed Several custom or preshaped plates for weight-bearing while wearing an elas-
operative treatment for intra-articular tuberosity fractures117-121, various types tic ankle orthosis for 6 weeks127.
tuberosity fractures with a displacement of screws101,120-124 (Fig. 3), and, A below-the-knee cast is not required.
Fig. 4
Figs. 4-A, 4-B, and 4-C Internal fixation of a
Jones fracture with an intramedullary screw.
Fig. 4-A Postinjury radiograph. Fig. 4-B Fixa-
tion with an intramedullary 4.0-mm cancellous
screw that breached the distal aspect of the
cortex during insertion but had no impact on
the course of healing. Fig. 4-C Radiographic
evidence of complete bone-healing at 6 weeks
after surgery.
OCTOBER 2021 · VOLUME 9, ISSUE 10 · e21.00010 5
| Fractures of the Base of the Fifth Metatarsal Bone
Fig. 5
Figs. 5-A through 5-G Intramedullary fixation by different types of screws, including a cortical 3.5-mm screw (Fig. 5-A), a cortical 4.5-mm screw (Fig. 5-B), a cancellous 6.5-mm
screw (Fig. 5-C), a 4.5-mm locking compression plate (LCP) screw (Fig. 5-D), a cancellous 4.0-mm screw (Fig. 5-E), a cannulated cancellous 4.0-mm screw (Fig. 5-F), and a cannulated
cancellous 6.5-mm screw (Fig. 5-G).
Treatment outcomes have been excel- loading or partial weight-bearing (20 kg) Multiple studies have been con-
lent, regardless of the implant that for 6 to 8 weeks in a boot or a cast27,49,56, ducted to optimize internal fixation of
was used101,111,112,118-125. 86
. One study reported delayed union in PFMT fractures with an intramedullary
18% of patients with non-weight- screw142,143,146,147. In CT-based stud-
Treatment of Jones Fractures—Zone 2 bearing for 4 to 6 weeks49. The patient- ies, the medullary canal diameter aver-
Nonoperative Treatment reported outcomes are uniformly good aged 4.0 mm at the apex of the curvature
Nonoperative treatment for non- and similar to those with tuberosity and 5.0 mm at the isthmus142,143. As
displaced true zone-2 fractures (i.e., an fractures49,86,99,119,128. most authors have proposed using the
acute transverse or short oblique fracture largest possible screw diameter, the most
exiting through the fourth-fifth inter- Operative Treatment frequently recommended diameter is
metatarsal joint) is generally indicated in Operative treatment is generally favored 4.5 mm, with recommendations rang-
the nonathletic population27,49,56,86,89, with zone-2 fractures that are displaced ing from 4.0 to 6.5 mm in a systematic
94,95,99,128
. There is no evidence that by .2 mm49,76,99. Internal fixation also review148. Larger screw diameters have
nonoperative treatment substantially has been advocated for nondisplaced greater bending fatigue strength144 and
increases the risk of refracture49,53,99, zone-2 fractures in athletes, high-demand pullout strength136. In some biome-
129
. However, the time to heal and re- patients, and young active patients, with chanical investigations, this did not
turn to full activities can be decreased the aim of reducing the healing time translate into relevant differences in
with operative treatment, which is of and expediting return to sport or clinical studies regarding nonunion,
particular interest for athletes and young work6,27,49,50,56,76,85,86,108,110,129-132. refracture, or screw breakage71,140.
high-demand patients47,64,130. In a The method of choice for most Porter et al. found bending in 3 of
recent systematic review, pooled out- authors is an intramedullary screw27,49, twenty 4.5-mm screws and no bending
123,131,133,134
comes for nonoperative versus operative (Fig. 4). Various types of in twenty-three 5.5-mm screws71. Horst
treatment of zone-2 fractures revealed cortical, cancellous, and locking (solid or et al. found an equal torsional stiffness
union rates of 77% versus 96% and cannulated) screws of appropriate with 5.0 and 6.5-mm screws149. How-
mean time to union of 11 versus 9 diameters, thread length (partially or ever, to achieve stability, the 5.0-mm
weeks129. fully threaded screws), and materials are screw had to reach the metatarsal neck.
Recommendations differ for the available40,71,135-144 (Fig. 5). Other The required screw length tended to
postoperative protocol. Numerous types of internal fixation include a bi- straighten the normally curved fifth
authors have reported union rates cortical screw123, tension-band wiring, metatarsal bone and caused lateral gap-
between 96% and 100% with full Kirschner wires120, and plates118,119, ping of the fracture. Solid screws have a
145
weight-bearing as tolerated by the . The latter are preferred for commi- higher fatigue bending strength than
patient for 6 to 8 weeks with the use of an nuted fractures, and designs include cannulated screws144, but, again, to our
elastic bandage or a hard-soled shoe52,89, ulnar locking compression119 and hook knowledge, no correlation between
94,95,99,128
. Others recommend off- plates145. screw design and nonunion rate has been
6 OCTOBER 2021 · VOLUME 9, ISSUE 10 · e 21.00010
Fractures of the Base of the Fifth Metatarsal Bone |
found in clinical studies140. Neverthe- lated a clinically achievable screw length Most of the recent literature has
less, variable-pitch headless compression of 48 mm and a thread length of recommended postoperative weight-
screws, although they generate 30% less 28 mm153. They also found that the bearing as tolerated in a brace50,131,159,
163,164
compression150 and have inferior fatigue screw path compromised the peroneus , while earlier studies favored
strength144 than partially threaded brevis and plantar fascia insertions in partial or no weight-bearing for 5 to 12
constant-pitch screws, led to excellent 33% and 62% of cases, respectively153. weeks49,56,85,109,123,133. Return to sport
outcomes in a study of 60 Japanese The optimal site for screw insertion is on a professional level is achieved after 6
athletes, with a 97% union rate and no 10.5 mm dorsal to the inferior margin to 8 weeks50,131,159,163.
refractures139. Indication-specific and 5.3 mm medial to the lateral margin The reported results have been
screws have improved biomechanical of the tuberosity, just medial to the good, but the problem with several
properties over traditional screws144,151, insertion of the peroneus brevis ten- studies is that they included stress frac-
152
, with less adverse events demon- don154. The screw should be directed tures131,134 or tuberosity fractures119,
strated in 1 clinical study141. upward at an angle of ,10°5,85. Khur- 123
in the category of Jones fractures.
Another important parameter is ana et al. found that lateral and inferior
screw length, which should be neither insertion was associated with fracture Treatment of Stress Fractures—
too short, resulting in insufficient sta- site distraction155. Patients with a plan- Zone 3
bility, nor too long, risking medial cortex tar gap had an increased risk of delayed Nonoperative Treatment
perforation, straightening of the meta- union17,156. The treatment of stress fractures is the
tarsal, and lateral opening of the frac- There is evidence from numerous subject of lively debate. Torg et al. rec-
ture136,142,143,149. When using partially studies that minimally invasive intra- ommended nonoperative treatment of
threaded screws, the threads should be medullary screw fixation allows early type-I and II fractures, except in young
situated completely in the distal frag- postoperative weight-bearing, with athletes (type II)6. Operative treatment
ment in order to achieve compression union rates ranging from 89% to 100% was recommended for type-III frac-
across the fracture. In CT-based studies, and no need for bone-grafting3,5,49,50,99, tures6,85. Historically, nonoperative
DeSandis et al.143 measured an average 133,137,157-159
. The main disadvan- treatment of these fractures is associated
distance of 42.6 mm from the apex to the tages of intramedullary screws are a with a prolonged period of immobiliza-
base in the anteroposterior view, and demanding insertion technique, the risk tion, a long healing time4,6,27,110,165, a
Ochenjele et al.142 measured an average of irritation of the sural nerve, and higher incidence of delayed healing and
straight segment length of 52 mm. In a symptomatic prominence of the screw nonunion in 25% to 67% of cases3,4,6,
cadaveric study, van Dijk et al. calcu- head3,5,49,122,130,133,158,160-163. 13,49,53,56
, and refracture rates of up to
Fig. 6
Figs. 6-A, 6-B, and 6-C A stress fracture that
was treated by an intramedullary 4.5-mm
cortical screw. Fig. 6-A Postinjury radiograph.
Fig. 6-B Postoperative radiograph. Fig. 6-C The
healed fracture at 2 months after surgery.
OCTOBER 2021 · VOLUME 9, ISSUE 10 · e21.00010 7
| Fractures of the Base of the Fifth Metatarsal Bone
Fig. 7
Figs. 7-A through 7-E Nonunion of a stress fracture after intramedullary screw fixation. Fig. 7-A A stress fracture (with pain persisting for 5 months).
Fig. 7-B Fixation with a 4.5-mm cortical screw (the patient refused non-weight-bearing after surgery). Fig. 7-C Migration of the screw at 5 months after
surgery. Fig. 7-D Refixation with an intramedullary 6.5-mm cancellous screw. Fig. 7-E Healed fracture at 3 months after refixation.
50% if the patients are followed for a published by Furia et al.166, Albisetti healing76,132. Plate fixation has been
longer time period3,49,53,85,130. Inter- et al.167, Alvarez et al.168, and Taki successfully employed for Torg type-II
pretation of these data is difficult since et al.169. Nolte et al. used LIPUS in 594 and III fractures176,178. In cases of de-
most of these studies combined the metatarsal fractures, of which 161 were layed healing or nonunion (Torg type-II
results of zone-2 and 3 fractures under Jones fractures, and achieved a healing and III fractures), several authors have
the term “Jones fracture.” rate of 97.3%170. Holmes reported that combined internal fixation with the
Nonoperative treatment usually 9 fifth metatarsal stress fractures healed application of bone marrow aspirate
consists of non-weight-bearing on the with the use of PEMF therapy171. concentrate (BMAC) to the fracture
foot and protection in a short leg cast6,49, site134,141,161,172,179 or cancellous bone-
130,165
. Other authors have recom- Operative Treatment grafting from the calcaneus, the tibia, or
mended limited weight-bearing, or full From the available evidence, operative the iliac crest6,40,56,141,162,175,178-182.
weight-bearing as tolerated, in a hard- treatment is recommended for Torg
Popovic et al. found less refractures
soled shoe, a walking cast, or a molded type-II and III stress fractures of the
(0 versus 27%) in professional football
orthosis, or with strapping47,52. How- PFMT3-5,49,71,76,130,131,157,159,172. In
players with Torg type-I and II fractures
ever, if patients fail to comply with the professional athletes and other high-
when 4.5-mm screw fixation was sup-
protocol of limited or non-weight- demand patients, operative treatment is
plemented by local bone-grafting40.
bearing, the risk of delayed healing or recommended for all zone-3 fractures
Bone grafts may be applied as
nonunion is markedly higher6. The because it reduces the time to return to
sliding (local) grafts from the fifth met-
period of immobilization is 6 to 12 unlimited sporting activities3-5,71,130,
131,148,157,159,172,173 atarsal2,4,6 or as corticocancellous grafts
weeks, the time to return to sport activ- .
that have been harvested from the iliac
ities is 15 to 26 weeks, and the period of Currently, the most commonly
radiographic healing is 3.1 to 8.4 used method is insertion of an intra- crest, the calcaneus, or the tibia40,141,162,
175,179,181,182
months4,6,49,130,165. medullary screw3,5,71,131,137,158,159,174 .
Several methods have been em- (Fig. 6). Plates175,176 or tension-band The time to clinical healing is
ployed to enhance fracture-healing in wiring114,115 are used less frequently. reported to be between 3 and 13 weeks5,
40,49,131,137,157-159
fifth metatarsal stress fractures and de- Some authors practice minimally inva- . The time to radio-
layed unions, including ESWT sive screw fixation (e.g., in zone-2 frac- graphic union ranges from 6 to 24
(external/extracorporeal shockwave tures) without surgical preparation of weeks3,5,40,49,131,134,157,161,172,175.
therapy), LIPUS (low-intensity pulsed the nonunion site177. Drilling of the Patients returned to full activities,
ultrasound), and PEMF (pulsed elec- medullary canal has been advocated in including sports, within 8 to 15 weeks5,
71,131,134,137,157,159,172
tromagnetic field) therapy. Good out- cases of cortical thickening, with partial . A delay of full
comes after ESWT, with healing rates obliteration of the canal (Torg type-II weight-bearing, and a delay of return to
similar to screw fixation, have been fractures) in order to enhance bone- sport, did not seem to have a relevant
8 OCTOBER 2021 · VOLUME 9, ISSUE 10 · e 21.00010
Fractures of the Base of the Fifth Metatarsal Bone |
impact on radiographic healing127,159, required in up to 30% of cases after treatment of the fractures and their
172 complications in athletes. Am J Sports Med.
. intramedullary screw fixation5,130,133 1979 Mar-Apr;7(2):95-101.
Several authors recorded excellent and in up to 31% of cases following plate 5. DeLee JC, Evans JP, Julian J. Stress fracture of
results after use of a single screw3,5,40,71, fixation175,185. Prominence of the screw the fifth metatarsal. Am J Sports Med. 1983 Sep-
122,131,137,157-159,174 Oct;11(5):349-53.
, use of a screw in head can be prevented by countersink-
6. Torg JS, Balduini FC, Zelko RR, Pavlov H, Peff
combination with BMAC134,161,172, ing it into the bone. After removal of the TC, Das M. Fractures of the base of the fifth
and use of a screw in combination with plating, screw holes will remain as a metatarsal distal to the tuberosity.
Classification and guidelines for non-surgical
cancellous bone-grafting or a solid bone stress riser and may lead to refracture in and surgical management. J Bone Joint Surg
graft40,141,162,175,179,181,182. Reported athletes50,175. Screw breakage, nonun- Am. 1984 Feb;66(2):209-14.
union rates after operative treatment of ion, and refracture require reoperation 7. Jones R. I. Fractures of the base of the fifth
metatarsal bone by indirect violence. Ann Surg.
zone-3 fractures and nonunions have (Fig. 7). 1902 Jun;35(6):697-700: 2.
ranged between 86% and 100%5,49,50, Refractures or nonunions have 8. Wharton HR. Fracture of the proximal end of
133,158,172,175 the fifth metatarsal bone. Ann Surg. 1908;47:
. Lee et al. found a longer been successfully treated with larger-
824-6.
time to union if a preoperative plantar diameter screws and additional aug- 9. Pearson JB. Fractures of base of fifth
gap of 1 mm was present17,156. mentation with either BMAC or metatarsal. Br Med J. 1962 Apr 14;1(5284):
1052-4.
bone-grafting48,179,186,187 or with
10. Lehman RC, Torg JS, Pavlov H, DeLee JC.
Complications plantar plating and autograft178. Exci- Fractures of the base of the fifth metatarsal
Intraoperative complications comprise sion of small tuberosity fragments distal to the tuberosity: a review. Foot Ankle.
1987 Feb;7(4):245-52.
injuries to the sural nerve or the lateral has been successfully employed for
11. Rosenberg GA, Sferra JJ. Treatment
dorsal cutaneous nerve99,111,119,122,134, painful nonunion after a zone-1 frac- strategies for acute fractures and nonunions of
159,160
, injuries to the peroneus brevis ture103,104,188,189 as well as for sympto- the proximal fifth metatarsal. J Am Acad Orthop
Surg. 2000 Sep-Oct;8(5):332-8.
tendon with difficult insertion of the matic accessory bones44,45.
12. Nunley JA. Fractures of the base of the fifth
intramedullary screw3,162, breakage of metatarsal: the Jones fracture. Orthop Clin
the drill bit162, straightening of the Source of Funding North Am. 2001 Jan;32(1):171-80.
metatarsal136,142,143, perforation of the There was no source of external funding 13. Egol K, Walsh M, Rosenblatt K, Capla E, Koval
KJ. Avulsion fractures of the fifth metatarsal
medial cortex40, breakage of the metatar- for this study. base: a prospective outcome study. Foot Ankle
sal136, suboptimal insertion of the im- Int. 2007 May;28(5):581-3.
plant that is potentially associated with Kamila Bušková, MD1, 14. Chee-Kidd C, Vivek AS. Is nonoperative
Jan Bartonı́ček, MD, DSc1,2, treatment still indicated for Jones fracture? Eur J
the risk of damage of the cortex distal to Trauma Emerg Surg. 2009 Aug;35(4):407. Epub
Stefan Rammelt, MD, PhD3
the fracture3,40, and fracture of the base158. 2009 Feb 14.
Postoperative complications 1Department
15. Smith TO, Clark A, Hing CB. Interventions for
of Orthopaedics, First treating proximal fifth metatarsal fractures in
include wound-healing disorders Faculty of Medicine Charles University and adults: a meta-analysis of the current evidence-
(seroma, hematoma, superficial infec- Military University Hospital Prague, base. Foot Ankle Surg. 2011 Dec;17(4):300-7.
Prague, Czech Republic Epub 2011 Feb 20.
tion)99,162,172, paresthesia99,111,119,
122,134,159
16. Dobrindt O, Hoffmeyer B, Ruf J,
, painful prominence of the 2Department Seidensticker M, Steffen IG, Fischbach F, Zarva
of Anatomy, First Faculty of
implant3,5,49,122,130,134,159,161, screw Medicine, Charles University Prague,
A, Wieners G, Ulrich G, Lohmann CH, Amthauer
H. Estimation of return-to-sports-time for ath-
breakage 3,22 , a ruptured wire Prague, Czech Republic letes with stress fracture - an approach com-
band 123 , and fracture of the medial bining risk level of fracture site with severity
3University Center of Orthopaedics and based on imaging. BMC Musculoskelet Disord.
cortex distal to the fracture line 40. 2012 Aug 6;13:139.
Traumatology, University Hospital Carl
Sural neuritis has been reported 17. Lee KT, Park YU, Jegal H, Park JW, Choi JP,
Gustav Carus Dresden, Dresden, Germany
in 5% to 25% of cases after open Kim JS. Prognostic classification of fifth
metatarsal stress fracture using plantar gap.
exposure of the PFMT, but mostly Email for corresponding author: Foot Ankle Int. 2013 May;34(5):691-6. Epub
resolves spontaneously within 6 kamila.buskova@uvn.cz 2013 Feb 4.
weeks 178 . 18. Thevendran G, Deol RS, Calder JD. Fifth
metatarsal fractures in the athlete: evidence for
Delayed healing was observed after References management. Foot Ankle Clin. 2013 Jun;18(2):
both operative99,119,121,134,137,172,174 1. Stewart IM. Jones’s fracture: fracture of base 237-54.
of fifth metatarsal. Clin Orthop. 1960;16(16): 19. Ferguson KB, McGlynn J, Jenkins P, Madeley
and nonoperative treatment3,4,47,49,93, 190-8.
99,130
NJ, Kumar CS, Rymaszewski L. Fifth metatarsal
. Refractures were seen after both 2. Dameron TB Jr. Fractures and anatomical fractures - Is routine follow-up necessary? Injury.
operative40,115,134,156,161,162,172,175, variations of the proximal portion of the fifth 2015 Aug;46(8):1664-8. Epub 2015 May 27.
182-184 metatarsal. J Bone Joint Surg Am. 1975 Sep; 20. Cheung CN, Lui TH. Proximal fifth
and nonoperative3,4,47,130 57(6):788-92. metatarsal fractures: anatomy, classification,
treatment. 3. Kavanaugh JH, Brower TD, Mann RV. The treatment and complications. Arch Trauma Res.
Prominent implants may be Jones fracture revisited. J Bone Joint Surg Am. 2016 Jun 13;5(4):e33298.
1978 Sep;60(6):776-82. 21. Le M, Anderson R. Zone II and III fifth
removed after union of the bone has 4. Zelko RR, Torg JS, Rachun A. Proximal metatarsal fractures in athletes. Curr Rev
been achieved. This is reported to be diaphyseal fractures of the fifth metatarsal— Musculoskelet Med. 2017 Mar;10(1):86-93.
OCTOBER 2021 · VOLUME 9, ISSUE 10 · e21.00010 9
| Fractures of the Base of the Fifth Metatarsal Bone
22. Bušková K, Kuběnová D, Tuček M. [Fractures fifth metatarsal osteotomy. Foot Ankle Int. 2013 58. Petrisor BA, Ekrol I, Court-Brown C. The
of the fifth metatarsal base]. Rozhl Chir. 2018 Jan;34(1):117-23. epidemiology of metatarsal fractures. Foot
Winter;97(2):60-6. [Czech]. 40. Popovic N, Jalali A, Georis P, Gillet P. Ankle Int. 2006 Mar;27(3):172-4.
23. Wang Y, Gan X, Li K, Ma T, Zhang Y. Proximal fifth metatarsal diaphyseal stress 59. Shuen WM, Boulton C, Batt ME, Moran C.
Comparison of operative and non-operative fracture in football players. Foot Ankle Surg. Metatarsal fractures and sports. Surgeon. 2009
management of fifth metatarsal base fracture: A 2005;11(3):135-41. Apr;7(2):86-8.
meta-analysis. PLoS One. 2020 Aug 13;15(8): 41. Ramponi DR. Proximal fifth metatarsal 60. Cakir H, Van Vliet-Koppert ST, Van Lieshout
e0237151. fractures. Adv Emerg Nurs J. 2013 Oct-Dec; EM, De Vries MR, Van Der Elst M, Schepers T.
24. Malgaigne JF. Traité des fractures et des 35(4):287-92. Demographics and outcome of metatarsal
luxations. Paris: JB Baillière; 1847. p 836. 42. Lawrence SJ, Botte MJ. The sural nerve in fractures. Arch Orthop Trauma Surg. 2011 Feb;
the foot and ankle: an anatomic study with 131(2):241-5. Epub 2010 Aug 17.
25. Carp L. Fracture of the fifth metatarsal bone:
with special reference to delayed union. Ann clinical and surgical implications. Foot Ankle Int. 61. Zhang Y. Foot fractures. In: Zhang Y (ed).
Surg. 1927 Aug;86(2):308-20. 1994 Sep;15(9):490-4. Clinical epidemiology of orthopedic trauma.
43. Fansa AM, Smyth NA, Murawski CD, Stuttgart: Thieme; 2012. p 507-24.
26. Lexer E, Kuliga P, Türk W. Untersuchungen
über Knochenarterien mittelst Kennedy JG. The lateral dorsal cutaneous 62. Kane JM, Sandrowski K, Saffel H, Albanese A,
Röntgenaufnahmen injizierter Knochen und branch of the sural nerve: clinical importance of Raikin SM, Pedowitz DI. The epidemiology of
ihre Bedeutung für einzelne pathologische the surgical approach to proximal fifth fifth metatarsal fracture. Foot Ankle Spec. 2015
Vorgänge am Knochensysteme. Berlin: metatarsal fracture fixation. Am J Sports Med. Oct;8(5):354-9. Epub 2015 Feb 9.
Hirschwald; 1904. 2012 Aug;40(8):1895-8. Epub 2012 Jun 7. 63. Court-Brown C, Clement ND. The
27. Lawrence SJ, Botte MJ. Jones’ fractures and 44. Muehleman C, Williams J, Bareither ML. A epidemiology of muskloskletal injury. In:
related fractures of the proximal fifth radiologic and histologic study of the os Tornetta P, Ricci WM, Ostrum RF, McKee MD,
metatarsal. Foot Ankle. 1993 Jul-Aug;14(6): peroneum: prevalence, morphology, and McQueen M, Court-Brown CH (eds). Rockwood
358-65. relationship to degenerative joint disease of the and Green’s Fractures in Adults. 9th edition.
foot and ankle in a cadaveric sample. Clin Anat. Philadelphia: Wolters Kluwer; 2020. p 123-87.
28. Hellpap W. The neglected lower ankle. The
2009 Sep;22(6):747-54. 64. Ekstrand J, van Dijk CN. Fifth metatarsal
“fracture” line of supination. Arch Orthop
Unfallchir. 1963 Jul 8;55:289-300. [German]. 45. Rammelt S, Manke E. Symptomatic os fractures among male professional footballers:
vesalianum. [German]. Fuss Sprungg. 2019;17: a potential career-ending disease. Br J Sports
29. Pearson JR. Combined fracture of the base Med. 2013 Aug;47(12):754-8. Epub 2013 Apr 9.
103-12.
of the fifth metatarsal and the lateral malleolus.
J Bone Joint Surg Am. 1961 Jun;43(4):513-6. 46. Tanton J. Fractures – fractures du membre 65. Richli WR, Rosenthal DI. Avulsion fracture of
inférieur. Paris: JB Bailliere; 1916. p 13-5. the fifth metatarsal: experimental study of
30. Heim U, Pfeiffer KM. Periphere pathomechanics. AJR Am J Roentgenol. 1984
Osteosynthese. Berlin: Springer; 1972. p 254-5. 47. Josefsson PO, Karlsson M, Redlund-Johnell
Oct;143(4):889-91, doi:10.2214/ajr.143.4.889.
I, Wendeberg B. Closed treatment of Jones
31. Schepers T, van Schie-van der Weert EM, de 66. Ding BC, Weatherall JM, Mroczek KJ,
fracture. Good results in 40 cases after 11-26
Vries MR, van der Elst M. Foot and ankle frac- Sheskier SC. Fractures of the proximal fifth
years. Acta Orthop Scand. 1994 Oct;65(5):545-7.
tures at the supination line. Foot (Edinb). 2011 metatarsal: keeping up with the Joneses. Bull
Sep;21(3):124-8. Epub 2010 Dec 23. 48. Glasgow MT, Naranja RJ Jr, Glasgow SG,
NYU Hosp Jt Dis. 2012;70(1):49-55.
Torg JS. Analysis of failed surgical management
32. Fick R. Handbuch der Anatomie und 67. Morris PM, Francois AG, Marcus RE, Farrow
of fractures of the base of the fifth metatarsal
Mechanik der Gelenke. Erster Teil: Anatomie der LD. The effect of peroneus brevis tendon
distal to the tuberosity: the Jones fracture. Foot
Gelenke. Jena: Fischer; 1904. anatomy on the stability of fractures at the fifth
Ankle Int. 1996 Aug;17(8):449-57.
33. Theodorou DJ, Theodorou SJ, Kakitsubata Y, 49. Chuckpaiwong B, Queen RM, Easley ME,
metatarsal base. Foot Ankle Int. 2015 May;36(5):
Botte MJ, Resnick D. Fractures of proximal 579-84. Epub 2014 Dec 30.
Nunley JA. Distinguishing Jones and proximal
portion of fifth metatarsal bone: anatomic and 68. Karnovsky SC, Rosenbaum AJ, DeSandis B,
diaphyseal fractures of the fifth metatarsal. Clin
imaging evidence of a pathogenesis of avulsion Johnson C, Murphy CI, Warren RF, Taylor SA,
Orthop Relat Res. 2008 Aug;466(8):1966-70.
of the plantar aponeurosis and the short Drakos MC. Radiographic analysis of national
Epub 2008 Mar 25.
peroneal muscle tendon. Radiology. 2003 football league players’ fifth metatarsal
;226(3):857-65. 50. Lareau CR, Anderson RB. Jones Fractures:
morphology relationship to proximal fifth
Pathophysiology and treatment. JBJS Rev. 2015
34. Kaneko F, Edama M, Ikezu M, Matsuzawa K, metatarsal fracture risk. Foot Ankle Int. 2019
Jul 28;3(7):01874474-201503070-00004.
Hirabayashi R, Kageyama I. Anatomic Mar;40(3):318-22. Epub 2018 Nov 7.
characteristics of tissues attached to the fifth 51. Polzer H, Polzer S, Mutschler W, Prall WC.
69. Raikin SM, Slenker N, Ratigan B. The
metatarsal bone. Orthop J Sports Med. 2020 Acute fractures to the proximal fifth metatarsal
association of a varus hindfoot and fracture of
Sep 18;8(9):2325967120947725. bone: development of classification and
the fifth metatarsal metaphyseal-diaphyseal
treatment recommendations based on the
35. Castro M, Melão L, Canella C, Weber M, junction: the Jones fracture. Am J Sports Med.
current evidence. Injury. 2012 Oct;43(10):
Negrão P, Trudell D, Resnick D. Lisfranc joint 2008 Jul;36(7):1367-72. Epub 2008 Apr 28.
1626-32. Epub 2012 Mar 30.
ligamentous complex: MRI with anatomic 70. Manoli AM, Graham B. Clinical and new
correlation in cadavers. AJR Am J Roentgenol. 52. Baumbach SF, Urresti-Gundlach M, Böcker aspects of the subtle cavus foot: a review of an
2010 Dec;195(6):W447-55. W, Vosseller JT, Polzer H. Results of functional
additional twelve-year experience. Fuss-
treatment of epi-metaphyseal fractures of the Sprungg. 2018;16(1):3-29.
36. Mason L, Jayatilaka MLT, Fisher A, Fisher L, base of the fifth metatarsal. Foot Ankle Int. 2020
Swanton E, Molloy A. Anatomy of the lateral Jun;41(6):666-73. Epub 2020 Feb 26. 71. Porter DA, Duncan M, Meyer SJ. Fifth
plantar ligaments of the transverse metatarsal metatarsal Jones fracture fixation with a 4.5-
arch. Foot Ankle Int. 2020 Jan;41(1):109-14. 53. Coleman MM, Guyton GP. Jones fracture in mm cannulated stainless steel screw in the
Epub 2019 Sep 10. the nonathletic population. Foot Ankle Clin. competitive and recreational athlete: a clinical
2020 Dec;25(4):737-51. Epub 2020 Oct 6. and radiographic evaluation. Am J Sports Med.
37. Edama M, Takabayashi T, Hirabayashi R,
Yokota H, Sekine C, Inai T, Matsuzawa K, Otsuki 54. Schepers T, Rammelt S. Classifying the 2005 May;33(5):726-33. Epub 2005 Feb 16.
T, Maruyama S, Kageyama I. Morphological Lisfranc injury: literature overview and a new 72. Lee KT, Kim KC, Park YU, Kim TW, Lee YK.
features of the lateral plantar ligament of the classification. FussSprungg. 2018;16(3):151-9. Radiographic evaluation of foot structure
transverse metatarsal arch. Clin Anat. 2020 Sep 55. Engelmann EWM, Rammelt S, Schepers T. following fifth metatarsal stress fracture. Foot
30. Epub 2020 Sep 30. Fractures of the cuboid bone: a critical analysis Ankle Int. 2011 Aug;32(8):796-801.
38. Smith JW, Arnoczky SP, Hersh A. The review. JBJS Rev. 2020 Apr;8(4):e0173. 73. Fujitaka K, Tanaka Y, Taniguchi A, Ogawa M,
intraosseous blood supply of the fifth 56. Dameron TB Jr. Fractures of the proximal fifth Isomoto S, Otuki S, Okubo M. Pathoanatomy of
metatarsal: implications for proximal fracture metatarsal: Selecting the best treatment option. J the Jones Fracture in Male University Soccer
healing. Foot Ankle. 1992 Mar-Apr;13(3):143-52. Am Acad Orthop Surg. 1995 Mar;3(2):110-4. Players. Am J Sports Med. 2020 Feb;48(2):
39. McKeon KE, Johnson JE, McCormick JJ, Klein 57. Nielsen TR, Lindblad BE, Faun P. Long-term 424-31. Epub 2019 Dec 30.
SE. The intraosseous and extraosseous vascular results after fracture of the fifth metatarsal. Foot 74. Hatch RL, Alsobrook JA, Clugston JR.
supply of the fifth metatarsal: implications for Ankle Surg. 1998;4(4):227-32. Diagnosis and management of metatarsal
10 OCTOBER 2021 · VOLUME 9, ISSUE 10 · e 21.00010
Fractures of the Base of the Fifth Metatarsal Bone |
fractures. Am Fam Physician. 2007 Sep 15;76(6): options for tuberosity fractures of the proximal nonunions of proximal fifth metatarsal avulsion
817-26. fifth metatarsal. Foot (Edinb). 2008 Sep;18(3): fractures in elite athletes. Am J Sports Med.
75. Sormaala MJ, Ruohola JP, Mattila VM, 156-8. Epub 2008 May 19. 2011 Nov;39(11):2466-9. Epub 2011 Aug 12.
Koskinen SK, Pihlajamäki HK. Comparison of 92. Shahid MK, Punwar S, Boulind C, Bannister 106. Akimau PI, Cawthron KL, Dakin WM,
1.5T and 3T MRI scanners in evaluation of acute G. Aircast walking boot and below-knee walk- Chadwick C, Blundell CM, Davies MB.
bone stress in the foot. BMC Musculoskelet ing cast for avulsion fractures of the base of the Symptomatic treatment or cast immobilisation
Disord. 2011 Jun 6;12:128. fifth metatarsal: a comparative cohort study. for avulsion fractures of the base of the fifth
76. Rammelt S, Heineck J, Zwipp H. Metatarsal Foot Ankle Int. 2013 Jan;34(1):75-9. metatarsal: a prospective, randomised, single-
fractures. Injury. 2004 Sep;35(Suppl 2):SB77-86. 93. Park JY, Kim HN, Hyun YS, Park JS, Kwon HJ, blinded non-inferiority controlled trial. Bone
Kang SH, Kim GL. Effect of weight-bearing in Joint J. 2016 Jun;98-B(6):806-11.
77. Banal F, Gandjbakhch F, Foltz V, Goldcher A,
Etchepare F, Rozenberg S, Koeger AC, conservative and operative management of 107. Choi YR, Kim BS, Kim YM, Park JY, Cho JH,
Bourgeois P, Fautrel B. Sensitivity and specificity fractures of the base of the fifth metatarsal Kim S, Kim HN. Hard-soled shoe versus short leg
of ultrasonography in early diagnosis of bone. Biomed Res Int. 2017;2017:1397252. cast for a fifth metatarsal base avulsion fracture:
metatarsal bone stress fractures: a pilot study of Epub 2017 Dec 26. a multicenter, noninferiority, randomized
37 patients. J Rheumatol. 2009 Aug;36(8): 94. Baumbach SF, Prall WC, Braunstein M, controlled trial. J Bone Joint Surg Am. 2021 Jan
1715-9. Epub 2009 Jun 30. Böcker W, Polzer S, Polzer H. [Fractures of the 6;103(1):23-9.
78. Drakonaki EE, Garbi A. Metatarsal stress base of the V metatarsal bone-current concepts 108. Strayer SM, Reece SG, Petrizzi MJ.
fracture diagnosed with high-resolution revised]. Unfallchirurg. 2018 Sep;121(9):723-9. Fractures of the proximal fifth metatarsal. Am
sonography. J Ultrasound Med. 2010 Mar;29(3): [German]. Fam Physician. 1999 May 1;59(9):2516-22.
473-6. 95. Biz C, Zamperetti M, Gasparella A, Dalmau- 109. Husain ZS, DeFronzo DJ. Relative stability
79. Ishibashi Y, Okamura Y, Otsuka H, Nishizawa Pastor M, Corradin M, de Guttry G, Ruggieri P.
of tension band versus two-cortex screw fixa-
K, Sasaki T, Toh S. Comparison of scintigraphy Early radiographic and clinical outcomes of
tion for treating fifth metatarsal base avulsion
and magnetic resonance imaging for stress minimally displaced proximal fifth metatarsal
fractures. J Foot Ankle Surg. 2000 Mar-Apr;39(2):
injuries of bone. Clin J Sport Med. 2002 Mar; fractures: cast vs functional bandage. Muscles
89-95.
12(2):79-84. Ligaments Tendons J. 2018 Jan 10;7(3):532-40.
96. Pituckanotai K, Arirachakaran A, 110. Zwitser EW, Breederveld RS. Fractures of
80. Brinker MR, O’Connor DP, Monla YT, the fifth metatarsal; diagnosis and treatment.
Earthman TP. Metabolic and endocrine Piyapittayanun P, Tuchinda H,
Peradhammanon E, Kongtharvonskul J. Injury. 2010 Jun;41(6):555-62. Epub 2009 Jun 30.
abnormalities in patients with nonunions. J
Orthop Trauma. 2007 Sep;21(8):557-70. Comparative outcomes of cast and removable 111. Thomas JL, Davis BC. Three-wire fixation
support in fracture fifth metatarsal bone: technique for displaced fifth metatarsal base
81. Taylor PN, Razvi S, Pearce SH, Dayan CM. systematic review and meta-analysis. J Foot fractures. J Foot Ankle Surg. 2011 Nov-Dec;
Clinical review: A review of the clinical Ankle Surg. 2018 Sep - Oct;57(5):982-6. 50(6):776-9. Epub 2011 Sep 10.
consequences of variation in thyroid function
within the reference range. J Clin Endocrinol 97. Khan S, Axelrod D, Paul R, Catapano M, 112. Kim J, Kim JW, Lee JI, Kim SK, Rhee SH.
Metab. 2013 Sep;98(9):3562-71. Epub 2013 Jul Stephen D, Henry P, Wasserstein D. Acute fifth Surgical treatment of the fifth metatarsal base
3. metatarsal tuberosity fractures: A systematic fracture using multiple Kirschner wires. J
review of nonoperative treatment. PM R. 2021 Korean Foot Ankle Soc. 2014 Mar;18(1):24-8.
82. Smith JT, Halim K, Palms DA, Okike K, Apr;13(4):405-11. Epub 2020 Aug 25.
Bluman EM, Chiodo CP. Prevalence of vitamin D 113. Giordano AR, Fallat LM. Strength analysis
deficiency in patients with foot and ankle 98. Lee TH, Lee JH, Chay SW, Jang KS, Kim HJ. of intraosseous wire fixation for avulsion
injuries. Foot Ankle Int. 2014 Jan;35(1):8-13. Comparison of clinical and radiologic outcomes fractures of the fifth metatarsal base. J Foot
Epub 2013 Oct 14. between non-operative and operative treat- Ankle Surg. 2004 Jul-Aug;43(4):225-30.
ment in 5th metatarsal base fractures (Zone 1).
83. Clutton J, Perera A. Vitamin D insufficiency Injury. 2016 Aug;47(8):1789-93. Epub 2016 May 114. Sarimo J, Rantanen J, Orava S, Alanen J.
and deficiency in patients with fractures of the 20. Tension-band wiring for fractures of the fifth
fifth metatarsal. Foot (Edinb). 2016 Jun;27:50-2. metatarsal located in the junction of the
Epub 2015 Aug 21. 99. Monteban P, van den Berg J, van Hees J, Nijs proximal metaphysis and diaphysis. Am J
S, Hoekstra H. The outcome of proximal fifth Sports Med. 2006 Mar;34(3):476-80. Epub 2005
84. Jones CP. Cavovarus: Fifth Metatarsal metatarsal fractures: redefining treatment
Fractures and Revision Open Reduction Internal Nov 22.
strategies. Eur J Trauma Emerg Surg. 2018 Oct;
Fixation. Clin Sports Med. 2020 Oct;39(4):793-9. 44(5):727-34. Epub 2017 Oct 12. 115. Lee KT, Park YU, Young KW, Kim JS, Kim JB.
85. Quill GE Jr. Fractures of the proximal fifth Surgical results of 5th metatarsal stress fracture
100. Nishikawa DRC, Aires Duarte F, Saito GH, using modified tension band wiring. Knee Surg
metatarsal. Orthop Clin North Am. 1995 Apr; Bang KE, Monteiro AC, Prado MP, de Cesar Netto
26(2):353-61. Sports Traumatol Arthrosc. 2011 May;19(5):
C. Treatment of zone 1 fractures of the proximal
853-7. Epub 2011 Feb 3.
86. Clapper MF, O’Brien TJ, Lyons PM. Fractures fifth metatarsal with CAM-walker boot vs hard-
of the fifth metatarsal. Analysis of a fracture soled shoes. Foot Ankle Int. 2020 May;41(5): 116. D’Hooghe P, Caravelli S, Massimi S, Calder
registry. Clin Orthop Relat Res. 1995 Jun;(315): 508-12. Epub 2020 Feb 5. J, Dzendrowskyj P, Zaffagnini S. A novel method
238-41. for internal fixation of basal fifth metatarsal
101. Wu GB, Li B, Yang YF. Comparative study of
fracture in athletes: a cadaveric study of the
87. Wiener BD, Linder JF, Giattini JF. Treatment surgical and conservative treatments for fifth
of fractures of the fifth metatarsal: a prospective metatarsal base avulsion fractures (type I) in F.E.R.I. technique (Fifth metatarsal, Extra-portal,
study. Foot Ankle Int. 1997 May;18(5):267-9. young adults or athletes. J Orthop Surg (Hong Rigid, Innovative). J Exp Orthop. 2019 Nov 11;
Kong). 2018 Jan-Apr;26(1):2309499017747128. 6(1):45.
88. Zenios M, Kim WY, Sampath J, Muddu BN.
Functional treatment of acute metatarsal 102. Sokkar SM, Abdelkafy A. Operative versus 117. Carpenter B, Garrett A. Using a hook plate
fractures: a prospective randomised nonoperative treatment of type 1 fifth as alternate fixation for fifth metatarsal base
comparison of management in a cast versus metatarsal fracture in nonprofessional athletes. fracture. J Foot Ankle Surg. 2003 Sep-Oct;42(5):
elasticated support bandage. Injury. 2005 Jul; Egypt Orthop J. 2016;51:319-22. 315-6.
36(7):832-5. Epub 2005 Mar 21. 103. Rettig AC, Shelbourne KD, Wilckens J. The 118. Choi JH, Lee KT, Lee YK, Lee JY, Kim HR.
89. Van Aaken J, Berli MC, Noger M, Gambirasio surgical treatment of symptomatic nonunions Surgical results of zones I and II fifth metatarsal
R, Fritschy D. [Symptomatic treatment of non- of the proximal (metaphyseal) fifth metatarsal base fractures using hook plates. Orthopedics.
displaced avulsion and Jones fractures of the in athletes. Am J Sports Med. 1992 Jan-Feb; 2013 Jan;36(1):e71-4.
fifth metatarsal: a prospective study]. [French]. 20(1):50-4. 119. Lee SK, Park JS, Choy WS. LCP distal ulna
Rev Med Suisse. 2007 Aug 2;3(120):1792-4. 104. Lee KT, Kim JB, Young KW, Park YU, Kim J, hook plate as alternative fixation for fifth
90. Vorlat P, Achtergael W, Haentjens P. Jegal H. Surgical excision of symptomatic metatarsal base fracture. Eur J Orthop Surg
Predictors of outcome of non-displaced frac- nonunion of fifth metatarsal base avulsion Traumatol. 2013 Aug;23(6):705-13. Epub 2012
tures of the base of the fifth metatarsal. Int Or- fracture in athletes. Korean J Sports Med. 2011 Aug 22.
thop. 2007 Feb;31(1):5-10. Epub 2006 May 23. Dec;29(2):118-21. 120. Kim JB, Ahn C, Park BS. Which surgical
91. Gray AC, Rooney BP, Ingram R. A 105. Ritchie JD, Shaver JC, Anderson RB, method is more effective in the fifth metatarsal
prospective comparison of two treatment Lawrence SJ, Mair SD. Excision of symptomatic base fracture? Foot Ankle Orthop. 2017;2(3).
OCTOBER 2021 · VOLUME 9, ISSUE 10 · e21.00010 11
| Fractures of the Base of the Fifth Metatarsal Bone
121. Xie L, Guo X, Zhang SJ, Fang ZH. Locking Jones fractures. Foot Ankle Int. 2001 Jul;22(7): 152. Willegger M, Benca E, Hirtler L, Moser L,
compression plate distal ulna hook plate 585-9. Zandieh S, Windhager R, Schuh R. Peroneus
fixation versus intramedullary screw fixation for 137. Reese K, Litsky A, Kaeding C, Pedroza A, brevis as source of instability in Jones fracture
displaced avulsion fifth Metatarsal Base Shah N. Cannulated screw fixation of Jones fixation. Int Orthop. 2020 Jul;44(7):1409-16.
fractures: a comparative retrospective cohort fractures: a clinical and biomechanical study. Epub 2020 May 5.
study. BMC Musculoskelet Disord. 2017 Sep 26; Am J Sports Med. 2004 Oct-Nov;32(7):1736-42. 153. van Dijk PA, Breuking S, Guss D, Johnson H,
18(1):405. DiGiovanni CW, Vopat B. Optimizing surgery of
138. DeVries JG, Cuttica DJ, Hyer CF.
122. Leumann A, Pagenstert G, Fuhr P, Cannulated screw fixation of Jones fifth metaphyseal-diaphyseal fractures of the fifth
Hintermann B, Valderrabano V. Intramedullary metatarsal fractures: a comparison of titanium metatarsal: a cadaveric study on implications of
screw fixation in proximal fifth-metatarsal and stainless steel screw fixation. J Foot Ankle intramedullary screw position, screw parame-
fractures in sports: clinical and biomechanical Surg. 2011 Mar-Apr;50(2):207-12. ters and surrounding anatomic structures. Injury.
analysis. Arch Orthop Trauma Surg. 2008 Dec; 2020 Dec;51(12):2887-92. Epub 2020 Sep 16.
139. Nagao M, Saita Y, Kameda S, Seto H,
128(12):1425-30. Epub 2008 Aug 2. 154. Johnson JT, Labib SA, Fowler R.
Sadatsuki R, Takazawa Y, Yoshimura M, Aoba Y,
123. Mahajan V, Chung HW, Suh JS. Fractures of Ikeda H, Kaneko K, Nozawa M, Kim SG. Headless Intramedullary screw fixation of the fifth
the proximal fifth metatarsal: percutaneous compression screw fixation of jones fractures: metatarsal: an anatomic study and improved
bicortical fixation. Clin Orthop Surg. 2011 Jun; an outcomes study in Japanese athletes. Am J technique. Foot Ankle Int. 2004 Apr;25(4):274-7.
3(2):140-6. Epub 2011 May 12. Sports Med. 2012 Nov;40(11):2578-82. Epub 155. Khurana A, Alexander B, Pitts C,
124. Chon JG, Choi H, Kim JB, Sun DH, Shin SY. 2012 Sep 18. Brahmbhatt A, Cage B, Greco E, McGwin G, Shah
The short term outcome of surgical treatment 140. Carreira DS, Sandilands SM. Radiographic AB. Predictors of Malreduction in Zone II and III
for the fifth metatarsal base fracture using a factors and effect of fifth metatarsal Jones and Fifth Metatarsal Fractures Fixed With an
headless cannulated compression screw. J diaphyseal stress fractures on participation in Intramedullary Screw. Foot Ankle Int. 2020 Dec;
Korean Foot Ankle Soc. 2016 Sep;20(3):131-4. the NFL. Foot Ankle Int. 2013 Apr;34(4):518-22. 41(12):1537-45. Epub 2020 Aug 14.
125. Hong CC, Nag K, Yeow H, Lin AZ, Tan KJ. Epub 2013 Feb 15. 156. Lee KT, Park YU, Young KW, Kim JS, Kim JB.
Suture anchor fixation for fifth metatarsal 141. Metzl J, Olson K, Davis WH, Jones C, Cohen The plantar gap: another prognostic factor for
tuberosity avulsion fractures: A case series and B, Anderson R. A clinical and radiographic fifth metatarsal stress fracture. Am J Sports Med.
review of literature. J Foot Ankle Surg. 2018 Sep comparison of two hardware systems used to 2011 Oct;39(10):2206-11. Epub 2011 Jul 14.
- Oct;57(5):1030-3. Epub 2018 May 18. treat Jones fracture of the fifth metatarsal. Foot 157. Mindrebo N, Shelbourne KD, Van Meter
126. Moshirfar A, Campbell JT, Molloy S, Jasper Ankle Int. 2013 Jul;34(7):956-61. CD, Rettig AC. Outpatient percutaneous screw
LE, Belkoff SM. Fifth metatarsal tuberosity 142. Ochenjele G, Ho B, Switaj PJ, Fuchs D, fixation of the acute Jones fracture. Am J Sports
fracture fixation: a biomechanical study. Foot Goyal N, Kadakia AR. Radiographic study of the Med. 1993 Sep-Oct;21(5):720-3.
Ankle Int. 2003 Aug;24(8):630-3. fifth metatarsal for optimal intramedullary 158. Fernández Fairen M, Guillen J, Busto JM,
screw fixation of Jones fracture. Foot Ankle Int. Roura J. Fractures of the fifth metatarsal in
127. Heineck J, Wolz M, Haupt C, Rammelt S,
2015 Mar;36(3):293-301. Epub 2014 Sep 24. basketball players. Knee Surg Sports Traumatol
Schneiders W. Fifth metatarsal avulsion
fracture: a rational basis for postoperative 143. DeSandis B, Murphy C, Rosenbaum A, Arthrosc. 1999;7(6):373-7.
treatment. Arch Orthop Trauma Surg. 2009 Aug; Levitsky M, O’Malley Q, Konin G, Drakos M. 159. Waverly BJ, Sorensen MD, Sorensen TK.
129(8):1089-92. Epub 2008 Sep 26. Multiplanar CT analysis of fifth metatarsal Early weightbearing protocol in operative
morphology: implications for operative fixation of acute Jones fractures. J Foot Ankle
128. Marecek GS, Earhart JS, Croom WP, Merk
management of zone II fractures. Foot Ankle Int. Surg. 2018 May - Jun;57(3):489-93.
BR. Treatment of acute Jones fractures without
2016 May;37(5):528-36. Epub 2015 Dec 17.
weightbearing restriction. J Foot Ankle Surg. 160. Donley BG, McCollum MJ, Murphy GA,
2016 Sep-Oct;55(5):961-4. Epub 2016 Jun 11. 144. Jastifer J, McCullough KA. Fatigue Richardson EG. Risk of sural nerve injury with
bending strength of Jones fracture specific intramedullary screw fixation of fifth metatarsal
129. Rikken QGH, Dahmen J, Hagemeijer NC, screw fixation. Foot Ankle Int. 2018 Apr;39(4):
Sierevelt IN, Kerkhoffs GMMJ, DiGiovanni CW. fractures: a cadaver study. Foot Ankle Int. 1999
493-9. Epub 2017 Dec 18. Mar;20(3):182-4.
Adequate union rates for the treatment of acute
proximal fifth metatarsal fractures. Knee Surg 145. Seyidova N, Hirtler L, Windhager R, Schuh 161. O’Malley M, DeSandis B, Allen A, Levitsky
Sports Traumatol Arthrosc. 2021 Apr;29(4): R, Willegger M. Peroneus brevis tendon in M, O’Malley Q, Williams R. Operative treatment
1284-93. Epub 2020 May 30. proximal 5th metatarsal fractures: Anatomical of fifth metatarsal Jones fractures (zones II and
considerations for safe hook plate placement. III) in the NBA. Foot Ankle Int. 2016 May;37(5):
130. Mologne TS, Lundeen JM, Clapper MF, Injury. 2018 Mar;49(3):720-5. Epub 2018 Jan 8.
O’Brien TJ. Early screw fixation versus casting in 488-500. Epub 2016 Jan 18.
the treatment of acute Jones fractures. Am J 146. Ebraheim NA, Haman SP, Lu J, Padanilam 162. Lemos LPV, Baumfeld TS, Macedo BD,
Sports Med. 2005 Jul;33(7):970-5. Epub 2005 TG, Yeasting RA. Anatomical and radiological Nery CAS, Batista JP, Baumfeld DS. Mid-term
May 11. considerations of the fifth metatarsal bone. follow-up after surgical treatment of fifth met-
Foot Ankle Int. 2000 Mar;21(3):212-5. atarsal base fractures in professional soccer
131. Massada MM, Pereira MA, de Sousa RJ,
147. Huh J, Glisson RR, Matsumoto T, Easley ME. players. Scientific J Foot Ankle. 2019;13(2):
Costa PG, Massada JL. Intramedullary screw
Biomechanical comparison of intramedullary 154-159.
fixation of proximal fifth metatarsal fractures in
athletes. Acta Ortop Bras. 2012;20(5):262-5. screw versus low-profile plate fixation of a 163. Watson S, Trammell A, Tanner S, Martin S,
Jones fracture. Foot Ankle Int. 2016 Apr;37(4): Bowman L. Early return to play after
132. Ruta DJ, Parker D. Jones fracture 411-8. Epub 2015 Dec 4. intramedullary screw fixation of acute Jones
management in athletes. Orthop Clin North
148. Roche AJ, Calder JD. Treatment and return fractures in collegiate athletes: 22-year
Am. 2020 Oct;51(4):541-53. Epub 2020 Aug 12.
to sport following a Jones fracture of the fifth experience. Orthop J Sports Med. 2020 Apr 24;
133. Portland G, Kelikian A, Kodros S. Acute metatarsal: a systematic review. Knee Surg 8(4):2325967120912423.
surgical management of Jones’ fractures. Foot Sports Traumatol Arthrosc. 2013 Jun;21(6): 164. Looney AM, Renehan JR, Dean DM,
Ankle Int. 2003 Nov;24(11):829-33. 1307-15. Epub 2012 Sep 6. Murthy A, Sanders TH, Neufeld SK, Cuttica DJ.
134. Murawski CD, Kennedy JG. Percutaneous 149. Horst F, Gilbert BJ, Glisson RR, Nunley JA. Rate of delayed union with early weightbearing
internal fixation of proximal fifth metatarsal Torque resistance after fixation of Jones following intramedullary screw fixation of
jones fractures (Zones II and III) with Charlotte fractures with intramedullary screws. Foot Jones fractures. Foot Ankle Int. 2020 Nov;41(11):
Carolina screw and bone marrow aspirate Ankle Int. 2004 Dec;25(12):914-9. 1325-34. Epub 2020 Jul 21.
concentrate: an outcome study in athletes. Am J
150. Orr JD, Glisson RR, Nunley JA. Jones 165. Zogby RG, Baker BE. A review of
Sports Med. 2011 Jun;39(6):1295-301. Epub nonoperative treatment of Jones’ fracture. Am J
fracture fixation: a biomechanical comparison
2011 Jan 6. Sports Med. 1987 Jul-Aug;15(4):304-7.
of partially threaded screws versus tapered
135. Pietropaoli MP, Wnorowski DC, Werner variable pitch screws. Am J Sports Med. 2012 166. Furia JP, Juliano PJ, Wade AM, Schaden W,
FW, Fortino MD. Intramedullary screw fixation Mar;40(3):691-8. Epub 2012 Jan 6. Mittermayr R. Shock wave therapy compared
of Jones fractures: a biomechanical study. Foot 151. Nunley JA, Glisson RR. A new option for with intramedullary screw fixation for
Ankle Int. 1999 Sep;20(9):560-3. intramedullary fixation of Jones fractures: the nonunion of proximal fifth metatarsal
136. Kelly IP, Glisson RR, Fink C, Easley ME, Charlotte Carolina Jones Fracture System. Foot metaphyseal-diaphyseal fractures. J Bone Joint
Nunley JA. Intramedullary screw fixation of Ankle Int. 2008 Dec;29(12):1216-21. Surg Am. 2010 Apr;92(4):846-54.
12 OCTOBER 2021 · VOLUME 9, ISSUE 10 · e 21.00010
Fractures of the Base of the Fifth Metatarsal Bone |
167. Albisetti W, Perugia D, De Bartolomeo O, 174. Habbu RA, Marsh RS, Anderson JG, Bohay Jones fractures. Analysis of failure. Am J Sports
Tagliabue L, Camerucci E, Calori GM. Stress DR. Closed intramedullary screw fixation for Med. 2002 Jan-Feb;30(1):55-60.
fractures of the base of the metatarsal bones in nonunion of fifth metatarsal Jones fracture. 183. Lee KT, Park YU, Jegal H, Kim KC, Young
young trainee ballet dancers. Int Orthop. 2010 Foot Ankle Int. 2011 Jun;32(6):603-8. KW, Kim JS. Factors associated with recurrent
Feb;34(1):51-5. Epub 2009 May 5. 175. Young KW, Kim JS, Lee HS, Jegal H, Park fifth metatarsal stress fracture. Foot Ankle Int.
168. Alvarez RG, Cincere B, Channappa C, YU, Lee KT. Operative results of plantar plating 2013 Dec;34(12):1645-53. Epub 2013 Nov 11.
Langerman R, Schulte R, Jaakkola J, Melancon K, for fifth metatarsal stress fracture. Foot Ankle
184. Lee KT, Kim KC, Young KW, Jegal H, Park
Shereff M, Cross GL 3rd. Extracorporeal shock Int. 2020 Apr;41(4):419-27. Epub 2020 Jan 6.
YU, Lee HS, Roh Y. Conservative treatment of
wave treatment of non- or delayed union of 176. Müller SA, Gösele-Koppenburg A, Farkas
proximal metatarsal fractures. Foot Ankle Int. refractures after modified tension band wiring
G. Plate osteosynthesis of a fifth metatarsal of fifth metatarsal base stress fractures in
2011 Aug;32(8):746-54.
stress fracture in a professional soccer player. athletes. J Orthop Surg (Hong Kong). 2020 Jan-
169. Taki M, Iwata O, Shiono M, Kimura M, [German]. Dtsch Z Sportmed. 2011;62(12): Apr;28(2):2309499020926282.
Takagishi K. Extracorporeal shock wave therapy 386-9.
for resistant stress fracture in athletes: a report 185. Kadar A, Ankory R, Karpf R, Luger E, Elias S.
177. Grant MJ, Molloy AP, Mason LW. The use of Plate fixation of proximal fifth metatarsal
of 5 cases. Am J Sports Med. 2007 Jul;35(7):
percutaneous screw fixation without fracture fracture. J Am Podiatr Med Assoc. 2015 Sep;
1188-92. Epub 2007 Feb 9.
site preparation in the treatment of fifth 105(5):389-94.
170. Nolte P, Anderson R, Strauss E, Wang Z, Hu metatarsal base nonunion. J Foot Ankle Surg.
L, Xu Z, Steen RG. Heal rate of metatarsal 2020 Jul - Aug;59(4):753-7. Epub 2020 Mar 12. 186. Granata JD, Berlet GC, Philbin TM, Jones G,
fractures: A propensity-matching study of Kaeding CC, Peterson KS. Failed surgical
178. Bernstein DT, Mitchell RJ, McCulloch PC, management of acute proximal fifth metatarsal
patients treated with low-intensity pulsed
Harris JD, Varner KE. Treatment of proximal fifth
ultrasound (LIPUS) vs. surgical and other treat- (Jones) fractures: a retrospective case series and
metatarsal fractures and refractures with
ments. Injury. 2016 Nov;47(11):2584-90. Epub literature review. Foot Ankle Spec. 2015 Dec;
plantar plating in elite athletes. Foot Ankle Int.
2016 Sep 13. 8(6):454-9. Epub 2015 Jun 30.
2018 Dec;39(12):1410-5. Epub 2018 Aug 6.
171. Holmes GB Jr. Treatment of delayed 187. Wright RW, Fischer DA, Shively RA, Heidt
179. Hunt KJ, Anderson RB. Treatment of Jones
unions and nonunions of the proximal fifth RS Jr, Nuber GW. Refracture of proximal fifth
fracture nonunions and refractures in the elite
metatarsal with pulsed electromagnetic fields. metatarsal (Jones) fracture after intramedullary
athlete: outcomes of intramedullary screw
Foot Ankle Int. 1994 Oct;15(10):552-6. screw fixation in athletes. Am J Sports Med.
fixation with bone grafting. Am J Sports Med.
172. Miller D, Marsland D, Jones M, Calder J. 2011 Sep;39(9):1948-54. Epub 2011 Jun 1. 2000 Sep-Oct;28(5):732-6.
Early return to playing professional football 188. Young JK. Fracture of the proximal end of
following fixation of 5th metatarsal stress
180. Lichtblau S. Painful nonunion of a fracture
of the 5th metatarsal. Clin Orthop Relat Res. the fifth metatarsal bone. Ann Surg. 1908;47:
fractures may lead to delayed union but does 826.
not increase the risk of long-term non-union. 1968 Jul-Aug;59(59):171-5.
Knee Surg Sports Traumatol Arthrosc. 2019 Sep; 181. Seidenstricker CL, Blahous EG, Bouché RT, 189. Solan M, Davies M. Nonunion of
27(9):2796-801. Epub 2018 Aug 28. Saxena A. Plate fixation with autogenous fifth metatarsal fractures. Foot Ankle
calcaneal dowel grafting proximal fourth and Clin. 2014 Sep;19(3):499-519. Epub 2014
173. Yates J, Feeley I, Sasikumar S, Rattan G,
fifth metatarsal fractures: technique and case Jul 19.
Hannigan A, Sheehan E. Jones fracture of the
fifth metatarsal: Is operative intervention series. J Foot Ankle Surg. 2017 Sep - Oct;56(5): 190. Wright JG. Revised grades of
justified? A systematic review of the literature 975-81. Epub 2017 Jun 9. recommendation for summaries or reviews of
and meta-analysis of results. Foot (Edinb). 2015 182. Larson CM, Almekinders LC, Taft TN, orthopaedic surgical studies. J Bone Joint Surg
Dec;25(4):251-7. Epub 2015 Aug 11. Garrett WE. Intramedullary screw fixation of Am. 2006;88(5):1161-2.
OCTOBER 2021 · VOLUME 9, ISSUE 10 · e21.00010 13
You might also like
- Medidas Medical Clinic Emergency Room PoliciesDocument3 pagesMedidas Medical Clinic Emergency Room PoliciesEduardo Anerdez100% (5)
- Structural and Dynamic Bases of Hand Surgery by Eduardo Zancolli 1969Document1 pageStructural and Dynamic Bases of Hand Surgery by Eduardo Zancolli 1969khox0% (1)
- PP 1 Intellicare Orientation SM PDFDocument59 pagesPP 1 Intellicare Orientation SM PDFJohn Reigh CatipayNo ratings yet
- Gynecomastia Surgery: Know Everything About The ProcedureDocument2 pagesGynecomastia Surgery: Know Everything About The ProcedureTandon ClinicNo ratings yet
- Paediatric Contact LenseDocument63 pagesPaediatric Contact LenseGurria NaheedNo ratings yet
- Atlas of Orthopaedic Surgical Approaches To The Lower Limbs (Rosa Ballis, Bujar H. Shabani, Dafina Bytyqi) Bibis - IrDocument88 pagesAtlas of Orthopaedic Surgical Approaches To The Lower Limbs (Rosa Ballis, Bujar H. Shabani, Dafina Bytyqi) Bibis - IrFarhan M. SalimNo ratings yet
- The External Fixator AOASIF-Threaded Rod System Spine-Fixator (Prof. Dr. Bernhard G. Weber Etc.) (Z-Library)Document385 pagesThe External Fixator AOASIF-Threaded Rod System Spine-Fixator (Prof. Dr. Bernhard G. Weber Etc.) (Z-Library)Asogaa MeteranNo ratings yet
- Lower Leg Pain Differential Diagnosis - NeuromuscularDocument14 pagesLower Leg Pain Differential Diagnosis - Neuromuscularapi-619359087No ratings yet
- Anatomic Exposures For Vascular InjuriesDocument32 pagesAnatomic Exposures For Vascular Injurieseztouch12No ratings yet
- Calcaneal-Stop Procedure For Treatment of Pediatric Flexible FlatfootDocument6 pagesCalcaneal-Stop Procedure For Treatment of Pediatric Flexible FlatfootEmiel AwadNo ratings yet
- Radionuclide Imaging of Infection and Inflammation - A Pictorial Case-Based Atlas (PDFDrive)Document342 pagesRadionuclide Imaging of Infection and Inflammation - A Pictorial Case-Based Atlas (PDFDrive)Emmanuel CabreraNo ratings yet
- Total Hip Replacement: Presented By: Atillio Castellani Brendan Cochren Trevor Kelly Shuntaro Maruyama Mustafa SharifDocument30 pagesTotal Hip Replacement: Presented By: Atillio Castellani Brendan Cochren Trevor Kelly Shuntaro Maruyama Mustafa SharifSaurabh AgarwalNo ratings yet
- Transition To Anterior Approach in Primary Total Hip Arthroplasty Learning Curve ComplicationsDocument7 pagesTransition To Anterior Approach in Primary Total Hip Arthroplasty Learning Curve ComplicationsAthenaeum Scientific PublishersNo ratings yet
- Lower Limb FracturesDocument120 pagesLower Limb FracturesAnda Madalina Zaharia100% (1)
- James P. Stannard Et La - Knee Surgery Tricks of the TradeDocument739 pagesJames P. Stannard Et La - Knee Surgery Tricks of the TradeFernanda NoraNo ratings yet
- 2015 OS - Fanelli Surgery PowerpointDocument24 pages2015 OS - Fanelli Surgery PowerpointMamedNo ratings yet
- Retrograde Tibia Intramedullary Nailing in Tibiotalocalcaneal ArthrodesisDocument14 pagesRetrograde Tibia Intramedullary Nailing in Tibiotalocalcaneal ArthrodesisAthenaeum Scientific PublishersNo ratings yet
- AN Outline To Bones and Tissue Injuries Management - 4 PDFDocument70 pagesAN Outline To Bones and Tissue Injuries Management - 4 PDFAlphamaleagainNo ratings yet
- Imagin For Students 2012Document307 pagesImagin For Students 2012yNo ratings yet
- Arthrodesis in The Charcot FooDocument6 pagesArthrodesis in The Charcot Foolatifa adluNo ratings yet
- Fracture and Dislocation of FootDocument67 pagesFracture and Dislocation of FootYi MaoNo ratings yet
- PFO UpdateDocument33 pagesPFO UpdateMitesh PatelNo ratings yet
- Pagine Da Master - Techniques - in - Orthopaedic - Surgery - Relevant - Surgical - Exposures - Master - Techniques - in - Orthopaedic - Surgery1Document100 pagesPagine Da Master - Techniques - in - Orthopaedic - Surgery - Relevant - Surgical - Exposures - Master - Techniques - in - Orthopaedic - Surgery1Χρόνης Σακαλής100% (1)
- Esquina Posteromedial RodillaDocument9 pagesEsquina Posteromedial RodillaSebastian RamirezNo ratings yet
- Journal of The Foot & AnkleDocument109 pagesJournal of The Foot & AnkleLyneth LacourtNo ratings yet
- Special Test KNEE UnaDocument25 pagesSpecial Test KNEE Unasingle_ladyNo ratings yet
- Dry needlingDocument147 pagesDry needlingabhinavbarua.abNo ratings yet
- JB6 4 121 727Document3 pagesJB6 4 121 727Rhizka djitmauNo ratings yet
- Ecografia 2Document324 pagesEcografia 2Angelo Dell'AnnaNo ratings yet
- Dupuytrens DiseaseDocument103 pagesDupuytrens DiseasefiestaNo ratings yet
- Pelvic FractureDocument31 pagesPelvic Fracturepoe3No ratings yet
- 1578.2-GLBL-En Persona Kinematically Aligned TKA SurgTech-digital1Document64 pages1578.2-GLBL-En Persona Kinematically Aligned TKA SurgTech-digital1mamyeu1801No ratings yet
- Hip Dislocation: Evaluation and Management: Review ArticleDocument11 pagesHip Dislocation: Evaluation and Management: Review ArticleFadhli Aufar KasyfiNo ratings yet
- AAOS Orthopaedic Board Preparation and Review and Analysis of Spine Sae andDocument6 pagesAAOS Orthopaedic Board Preparation and Review and Analysis of Spine Sae andICH KhuyNo ratings yet
- Afting in Revision Arthroplasty 3HAXAP PDFDocument466 pagesAfting in Revision Arthroplasty 3HAXAP PDFAndrés KnubelNo ratings yet
- Fractures Around The Knee: Filippo Castoldi Davide Edoardo BonasiaDocument164 pagesFractures Around The Knee: Filippo Castoldi Davide Edoardo BonasiaFabiano CardosoNo ratings yet
- Plates and ScrewsDocument96 pagesPlates and ScrewsFathy AlhallagNo ratings yet
- Pelvic Fractures. Part 2. Contemporary Indications and Techniques For Definitive Surgical Management PDFDocument11 pagesPelvic Fractures. Part 2. Contemporary Indications and Techniques For Definitive Surgical Management PDFJulio Cesar Guillen MoralesNo ratings yet
- Surgical Treatment of Cavus FootDocument25 pagesSurgical Treatment of Cavus FootRaeni Dwi Putri100% (1)
- IlizarovDocument2 pagesIlizarovsunshinehospitalNo ratings yet
- Management Tibial Plateau FractureDocument45 pagesManagement Tibial Plateau FracturePurushothama Rao NalamatiNo ratings yet
- Humero FX Holstein Lewis - Data Journals JBJS 445 1382Document8 pagesHumero FX Holstein Lewis - Data Journals JBJS 445 1382pai_sergNo ratings yet
- Soft Tissue Tumors - KransdorfDocument964 pagesSoft Tissue Tumors - Kransdorfsashop521No ratings yet
- Podiatry Res ManualDocument180 pagesPodiatry Res ManualJacob Dougherty50% (2)
- Disinfection GuidelinesDocument48 pagesDisinfection GuidelinesSlavica Gjurceska-GorjanskaNo ratings yet
- Treatment of SLAC-CartagenaDocument40 pagesTreatment of SLAC-CartagenaProfesseur Christian DumontierNo ratings yet
- 2002, Vol.33, Issues 1, Treatment of Complex FracturesDocument280 pages2002, Vol.33, Issues 1, Treatment of Complex FracturesSitthikorn StrikerrNo ratings yet
- Campbell's - Open FracturesDocument7 pagesCampbell's - Open FracturesMeroly QPNo ratings yet
- Meniscal Injuries - Management and Surgical Techniques (2014, Springer-Verlag New York)Document141 pagesMeniscal Injuries - Management and Surgical Techniques (2014, Springer-Verlag New York)okida192No ratings yet
- STP 1560-2013Document346 pagesSTP 1560-2013HieuHTNo ratings yet
- Shoulder Arthroscopy: How To Succeed!Document119 pagesShoulder Arthroscopy: How To Succeed!Btoaew BtoaewNo ratings yet
- Sheety PDFDocument378 pagesSheety PDFLakshita PrajapatiNo ratings yet
- Cavus Foot Deformity Evaluation and Surgical TechniquesDocument13 pagesCavus Foot Deformity Evaluation and Surgical TechniquesRadu StoenescuNo ratings yet
- Lewy Body Dementias Dementia With Lewy Bodies And.9Document29 pagesLewy Body Dementias Dementia With Lewy Bodies And.9Cristina GhizdavetNo ratings yet
- Hollerman Et Al 2013 Gunshot Wounds 2 RadiologyDocument12 pagesHollerman Et Al 2013 Gunshot Wounds 2 RadiologyMathisNo ratings yet
- CAA and Stroke in PregnancyDocument27 pagesCAA and Stroke in PregnancysaudNo ratings yet
- Harvesting Rib Cartilage Grafts For Secondary Rhinoplasty: Background: MethodsDocument7 pagesHarvesting Rib Cartilage Grafts For Secondary Rhinoplasty: Background: MethodsLuiggi Fayad100% (1)
- Flexor Tendon Repair, Rehabilitation, and Reconstruction: Preoperative AssessmentDocument11 pagesFlexor Tendon Repair, Rehabilitation, and Reconstruction: Preoperative AssessmentAdRiaNa JuLIetH LoZaDa PaTiÑoNo ratings yet
- TLIF Approaches ExplainedDocument8 pagesTLIF Approaches ExplainedAlex Cortes100% (1)
- GENETIC CLASSIFICATION OF BRECCIASDocument1 pageGENETIC CLASSIFICATION OF BRECCIASZulfa SabilyNo ratings yet
- Síndrome de Charcot-Marie-ToothDocument7 pagesSíndrome de Charcot-Marie-ToothXDbr xdNo ratings yet
- R02Y2002N01A0003Document27 pagesR02Y2002N01A0003Roseck BlackNo ratings yet
- The Value of The Tip Apex Distance in Predicting.12 PDFDocument7 pagesThe Value of The Tip Apex Distance in Predicting.12 PDFCrn HmdNo ratings yet
- Neoplastic Myelopathies: Continuumaudio Interviewavailable OnlineDocument22 pagesNeoplastic Myelopathies: Continuumaudio Interviewavailable OnlineDalwadi1No ratings yet
- Y To Use Epker Fish 2 ReasonsDocument10 pagesY To Use Epker Fish 2 ReasonsMuhammad AleemNo ratings yet
- EZIO ProtocolDocument1 pageEZIO ProtocolMary Janine Joy RimanoNo ratings yet
- Functional Outcome of Tardy Ulnar Nerve Palsy Manifests 2024 InternationalDocument4 pagesFunctional Outcome of Tardy Ulnar Nerve Palsy Manifests 2024 InternationalRonald QuezadaNo ratings yet
- RaVoR™ - Bipolar Radiofrequency Volume Reduction (RaVoR™) of The Inferior Turbinates - M. SarteDocument2 pagesRaVoR™ - Bipolar Radiofrequency Volume Reduction (RaVoR™) of The Inferior Turbinates - M. Sartediana mistraNo ratings yet
- LEEP 1000 Workstation Operating Manual 220vDocument24 pagesLEEP 1000 Workstation Operating Manual 220vpatrickNo ratings yet
- Endoscopy of GI TractDocument358 pagesEndoscopy of GI TractEngin UçarNo ratings yet
- Forceps and VentouseDocument28 pagesForceps and VentousePulkit JainNo ratings yet
- Season 7 Grys AnatomyDocument41 pagesSeason 7 Grys AnatomyAugusto CastellanoNo ratings yet
- Modern Management of Systolic Anterior Motion of The Mitral ValveDocument11 pagesModern Management of Systolic Anterior Motion of The Mitral ValveRodri EspinNo ratings yet
- Exhibitor DirectoryDocument44 pagesExhibitor DirectoryParul SabharwalNo ratings yet
- Hernia - Femoral Hernia, Epigastric Hernia, Paraumbilical Hernia, Incisional HerniaDocument29 pagesHernia - Femoral Hernia, Epigastric Hernia, Paraumbilical Hernia, Incisional HerniaKuruNo ratings yet
- Margareta Nordin, Gunnar B. J. Andersson, M. H. Pope - Musculoskeletal Disorders in The Workplace - Principles and Practice, 2nd Edition (2006)Document403 pagesMargareta Nordin, Gunnar B. J. Andersson, M. H. Pope - Musculoskeletal Disorders in The Workplace - Principles and Practice, 2nd Edition (2006)Kings AndrewNo ratings yet
- Assessment of Sentinel Lymph Node Biopsy Vs Lymphadenectomy For Intermediate - and High-Grade Endometrial Cancer StagingDocument8 pagesAssessment of Sentinel Lymph Node Biopsy Vs Lymphadenectomy For Intermediate - and High-Grade Endometrial Cancer StagingEzequiel GonzalezNo ratings yet
- Christian Rupal's ResumeDocument2 pagesChristian Rupal's ResumesaumiljoshilondonNo ratings yet
- CV JD Ghosh 20-08-2021Document32 pagesCV JD Ghosh 20-08-2021Jay Deep GhoshNo ratings yet
- Swimmer 'S Shoulder: Painful Shoulder in The Competitive SwimmerDocument10 pagesSwimmer 'S Shoulder: Painful Shoulder in The Competitive SwimmerGerardo EsäuNo ratings yet
- Reimbursement Claim Process & Checklist of Documents To Be SubmittedDocument4 pagesReimbursement Claim Process & Checklist of Documents To Be SubmittedRahul MalhotraNo ratings yet
- Gnyan Dental Healthcare Services Provider (DHSP) - NABH Standards SummaryDocument2 pagesGnyan Dental Healthcare Services Provider (DHSP) - NABH Standards Summarywriterlakshmiv100% (1)
- Sterile Processing Technician ResumeDocument4 pagesSterile Processing Technician Resumeusuoezegf100% (1)
- Factors That Influence Venous Leg Ulcer Healing and Recurrence Rate After Endovenous Radiofrequency Ablation of Incompetent Saphenous VeinDocument6 pagesFactors That Influence Venous Leg Ulcer Healing and Recurrence Rate After Endovenous Radiofrequency Ablation of Incompetent Saphenous VeinHan's OfficialNo ratings yet
- Bedah II PDFDocument71 pagesBedah II PDFAnggitNo ratings yet
- Forefoot Amputation Techniques for Diabetic PatientsDocument8 pagesForefoot Amputation Techniques for Diabetic PatientsmarkNo ratings yet
- Cleaning A Sutured Wound & Changing A Dressing On A Wound With A Drain Procedure ChecklistDocument3 pagesCleaning A Sutured Wound & Changing A Dressing On A Wound With A Drain Procedure ChecklistMonicaElizadePazNo ratings yet
- Vitreous Floaters: Publication DetailsDocument6 pagesVitreous Floaters: Publication Detailsmithaa octoviagnesNo ratings yet
- Silicon Induced LymphoafenopathyDocument5 pagesSilicon Induced LymphoafenopathyDiana RomanovaNo ratings yet
- 10 Tips About Aesthetic ImplantologyDocument16 pages10 Tips About Aesthetic ImplantologyMario Troncoso Andersenn0% (1)